4_SINDROME DE LA SEGUNDA NEURONA MOTORA.pptx
48
SÍNDROME NEURONA MOTORA INFERIOR II: SÍNDROMES ALTERNOS - SÍNDROME MIOPÁTICO - SÍNDROME EXTRAPIRAMIDAL: PARKINSON/ATETOSIS
-
Upload
jaime-alvitez-izquierdo -
Category
Documents
-
view
1.071 -
download
11
Transcript of 4_SINDROME DE LA SEGUNDA NEURONA MOTORA.pptx

SÍNDROME NEURONA MOTORA INFERIOR II:
SÍNDROMES ALTERNOS - SÍNDROME MIOPÁTICO -
SÍNDROME EXTRAPIRAMIDAL: PARKINSON/ATETOSIS

Se denomina síndrome de la segunda neurona motora al causado por la lesión de la segunda neurona de la vía motora, neurona motriz periférica o neurona espinomuscular y tienes dos formas: Si la lesión asienta sobre los núcleos de origen de
la segunda neurona a nivel del tallo cerebral o de la medula espinal se habla de parálisis nuclear.
Si la lesión asienta en algún punto del trayecto de las fibras que conforman la vía motora después de su emergencia en el núcleo de origen y hasta en el efector periférico se dice que la parálisis es infranuclear.
DEFINICION:

MANIFESTACIONES CLÍNICAS
El síndrome de la segunda neurona solo suele presentarse en cuatro formas posibles:paraplejia o paraparesia, monoplejía o monoparesia, polineuropatía y parálisis nerviosa aislada.

PARAPLEJÍA O PARAPARESIA
Paraplejía flácida medular:La lesión asienta en el cuerpo de la segunda motoneurona a nivel de las astas medulares anteriores, en el inicio de la parálisis suele ser rápido y con los signos respectivos del síndrome de la segunda neurona descritos se pueden asociar a los siguientes:
Signos de piramidalismo. Sucedáneos y reflejos de automatismo
medular. Anestesia total distal hasta el nivel de la
lesión. Trastornos esfinterianos.

SIGNOS Y SINTOMAS
Paresia o paralisis Atrofia, la atrofia por desuso.Hipotonía.Disminución de los reflejos Osteotendinosos.Aparición de fasciculaciones, cuando la segundo Motoneuronas se hace inestable comienza a descargar en forma espontanea y esa descarga produce que la unidad motora que depende de ella se contraiga y esa contracción uno la puede ver a través de la piel como una contracción de un seguimiento del músculo.Aparición de Calambres Patológicos, causas no claras. Exaltación de los reflejos superficiales.


NOMENCLATURA
FBC: facio braquialC: cefalicoB: braquial.


EJEMPLOS

SÍNDROMES ALTERNOS DEL TALLO.

SINDROMES ALTERNOS
Combinación de hemiplejía con lesiones de uno o varios nervios
craneales del lado opuesto

SINDROMES ALTERNOS
• Síndromes Mesencefalicos.
• Síndromes Pontinos.
• Síndromes bulbares.

Mesencéfalo
Puente
Bulbo

III
IV
V
VI
VII
VIII
IX
X
XI
XII

SINDROMES MESENCEFALICOS
.

SÍNDROME DE WEBER:
Afecta la via piramidal y III nervio craneal, dando lugar a hemiparesia contralateral y paresia del III NC del lado de la lesión con pupila dilatada arreactiva.

SÍNDROME DE CLAUDE:
La lesión se sitúa posterior a nivel del núcleo rojo (atravesado por el III NC). Consiste en paresia delIII NC del lado lesional y ataxia contralateral..

SÍNDROME DE BENEDIKT:
Cursa con III NC ipsilateral asociado
a movimientos anormales (corea, temblor y balismo) de los miembros
contralaterales a la lesión.

SÍNDROME DE PARINAUD:
El dato más característico es
una parálisis de la mirada conjugada hacia arriba, con
pupilas generalmente
dilatadas y acomodación conservada.

Sx piramidal + III NC ipsilateral + parálisis de la
mirada hacia el lado opuesto de
la lesión
SÍNDROME DE FOVILLE SUPERIOR:

SINDROME FOVILLE SUPERIOR
HEMIANESTESIA
HEMIPLEJIA
MIRADA HACUA EL LADO DE LA LESIÓN

SINDROMES PONTINOS.

SÍNDROME DE MILLARD GUBLER:
Se caracteriza por hemiplejía contralateralque respeta la cara y paresia de VI y VII pares cranealesipsilaterales.

SÍNDROME DE FOVILLE INFERIOR:
VII ipsilateral periférico + parálisis de la mirada lateral hacia el mismo lado de la lesión + sx piramidal

SINDROME DE FOVILLE INFERIOR
HEMIANESTESIA
MIRADA HACIA LA PARALISIS (huye de su
lesion)PARALISIS FACIAL
CENTRAL
HEMIPLEJIA

SÍNDROME DE BRISSAUD-SICCARD:
Hemiespasmos faciales asociado a Sx piramidal contralateral.

SINDROMES BULBARES.

SÍNDROME DE AVELLIS:
Afección del X NC ipsilateral (afección del núcleo ambiguo) + sx piramidal contralateral.
..Hemiplejía que respeta la cara, parálisis de cuerda vocal y hemivelopalatina

SÍNDROME DE SCHMIDT:
Afección del XI NC ipsilateral + Sx piramidal... Hemiplejía que respeta la cara, parálisis de cuerda vocal y hemivelopalatina + parálisis del trapecio y esternocleidomastoideo.

SÍNDROME DE JACKSON:
afección XII ipsilateral + síndrome piramidal... Hemiplejía que respeta la cara, parálisis de cuerda vocal y hemivelopalatina + parálisis del trapecio y esternocleidomastoideo + hemiparálisis y hemiatrofia lingual

SÍNDROME DE BABINSKI-NAGEOTTE:
Sx cerebeloso ipsilateral + alteraciones simpáticas ipsilaterales + hemianestesia contralateral + sx piramidal.

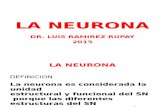
SÍNDROME DE WALLENBERG:
afección ipsilateral V, IX, X, XI + Sx Horner + Sx cerebeloso + afección sensitiva propioceptiva; contralateral afección sensitiva exteroceptiva

Sindrome de Wallemberg

MONOPLEJÍA O MONOPARESIA
Puede ser medular o radicular según que la lesión asiente en la medula o en las raíces anteriores, de manera similar a la descrita para la paraplejia; la paraplejia se encuentra clasificarse en distintos tipos:
Monoplejía radicular braquial: lesión en C5 a D1.
Monoplejía radicular crural: lesión en L1 a S2

POLINEUROPATÍA
La afectación troncular del nervio periférico tiene su expresión más característica en las polineuropatías, en las que se comprometen varios nervios de manera simultánea y simétrica, tanto en sus fibras motoras como sensitivas. Las causas mas frecuentes son:
trastornos metabólicos: diabetes periférica. Tóxicos: alcohol, plomo, arsénico, insecticida clorados, talio,
mercurio. Trastornos carenciales: vitamina B. Polirradiculoneuropatia. Infecciones: enfermedades virales o bacterianas. Colagenopatia y vascularitis. Enfermedades neoplásicas: linfomas, síndrome paraneoplasicos.
Al compromiso nervioso sucesivo y asimétrico se lo designa, en cambio mononeuritis, los signos de estos trastornos son los correspondientes al síndrome de la segunda motoneurona.

PARÁLISIS NERVIOSA AISLADA
Implica la lesión exclusiva de un nervio periférico, algunas parálisis aisladas de nervios periféricos suelen tener signos característicos: La parálisis del nervio radial, cuya función la extensión del miembro superior.
La parálisis del nervio mediano por lesión proximal, afecta la mortalidad de los músculos de la eminencia tenar.
La parálisis del nervio del nervio cubital, produce la llamada mano en garra o garra cubital.
La parálisis del ciática poplíteo externo impide la flexión del pie y es responsable de la marcha denominada en steppage.

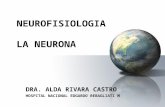
SINDROME MIOPÁTICO Debilidad motora proximal, en cinturas
escapular y pelvica Trofismo afectado con Hipotrofia o
PseudohipertrofiaPuede haber dolor de tipo muscularSigno de Gowers +, en distrofias musculares Etiologia: Polimiosisits, Distrofia de
Duchenne, Becker, Dreyfus, oculofaringea.

SIGNO DE GOWERS

Signod e Gowers

Signo de Gowers

Signo de Gowers

SINDROME EXTRAPIRAMIDAL:PARKIN
SON/ATETOSIS

El sistema extrapiramidal interviene en el control del movimiento voluntario y del tono muscular, y participa en la producción de movimientos automáticos y asociados. Los primeros son aquellos en los que no interviene la voluntad; puede ser :a) Emocionales; b) Institivos: defensivos o reactivos (como levantarse ante un
ruido fuerte); c) Aprendidos: primero se aprende por la voluntad y luego se
vuelven automáticos (como andar en bicicleta o nadar). Los movimientos asociados son en realidad movimientos
automáticos complejos, que acompañan al movimiento voluntario (como el balanceo de los brazos al caminar).
SISTEMA EXTRAPIRAMIDAL:

Por lesión de los núcleos basales (Núcleo Lenticular, Núcleo Caudado, Tálamo, Hipotálamo, Sustancia Negra, Núcleo Rojo) y/o sus vías nerviosas de conexión. Se produce una alteración en el tono muscular y en los movimientos automáticos y asociados. SÍNDROME PARKINSONIANO:Signos:
Actitud: flexión involuntaria de tronco, extremidades y cuello.Marcha: a pequeños pasos (festinante).Temblor distal de reposo: cuatro a cinco ciclos por segundo.Hipertonia muscular: rigidez (rueda dentada o caño de plomo). Hipocinesia: pobreza de movimientos (facie inexpresiva,
reducción de los movimientos automáticos habituales, sialorrea por menor deglución).
Bradicinesia: lentitud de los movimientos (aumenta el tiempo de reacción entre una orden y la ejecución del movimiento)
Otros: seborrea, hipercrinia lagrimal.

DESDE EL PUNTO DE VISTA SEMIOLÓGICO, LAS DISFUNCIONES DEL SISTEMA EXTRAPIRAMIDAL SE
MANIFIESTAN POR: Trastornos del movimiento:
a) voluntario híper cinéticos (aparición de movimiento anormales involuntarios: corea, atetosis, mioclonias, tics, temblores) o hipocinéticos (bradicinesia, acinesia);
b) automáticos y asociados: perdida de la mímica emocional, desaparición de movimientos asociados (como el balanceo de los brazos al caminar).
Trastornos del tono: hipotonía e hipertonía. Trastorno de la postura: distonía.

TIPOS DE MOVIMIENTOS ANORMALES trastornos del movimiento (hipocinesias e hipercinecias).
Trastornos del tono (hipertonía e hipotonía)
Trastornos de la postura (distonía).


SINDROME EXTRAPIRAMIDAL
Distonia cervical