Clase 5 stemi
25
Síndrome Coronario Agudo STEMI ST Elevation Myocardial Infarction
-
Upload
daniel-alejandro -
Category
Education
-
view
633 -
download
0
Transcript of Clase 5 stemi
Síndrome Coronario Agudo
STEMIST Elevation Myocardial Infarction
Un reconocimiento
La piedra angular del enfoque diagnóstico y terapéutico actual del STEMI, se estableció con la confirmación de que en la arteria perfusora de la zona comprometida se encuentra una trombosis desde los primeros síntomas en el 90% de los pacientes.DeWood MA, Spores J, Notske RN, et al. Prevalence of total coronary artery occlusion during the early hours of transmural myocardial infarction.
N Engl J Med. 1980; 303: 897-902.
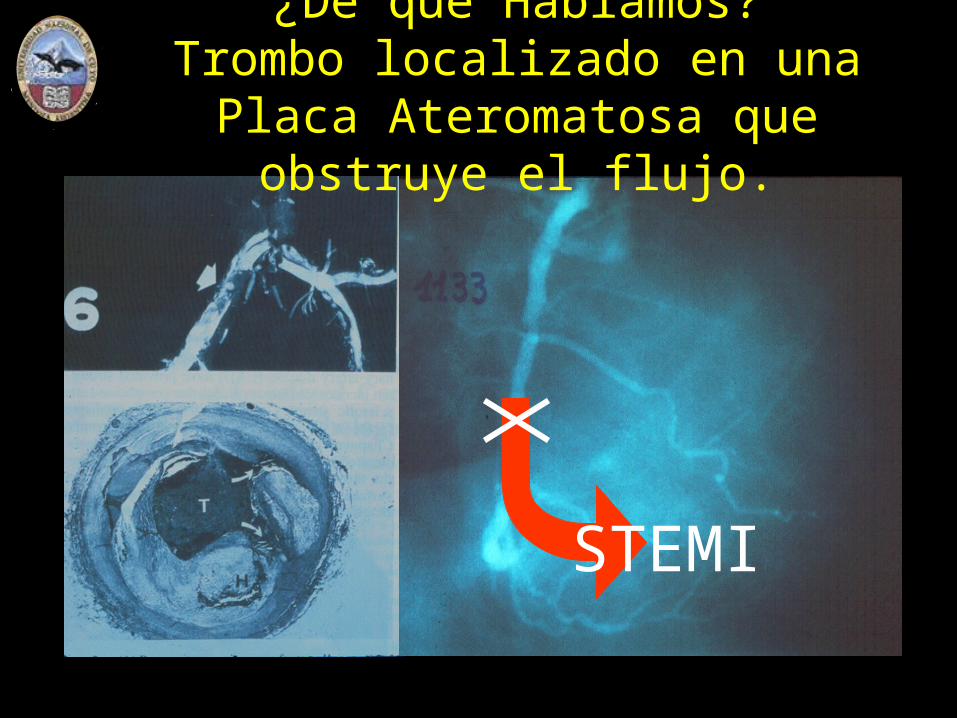
STEMI
¿De qué Hablamos?Trombo localizado en una Placa
Ateromatosa que obstruye el flujo.

Placas “Vulnerables”Esquema de Peter Libby
From Vulnerable Plaque to Vulnerable Patient
A Call for New Definitions and Risk Assessment Strategies Circulation 2003;108:1664-1672
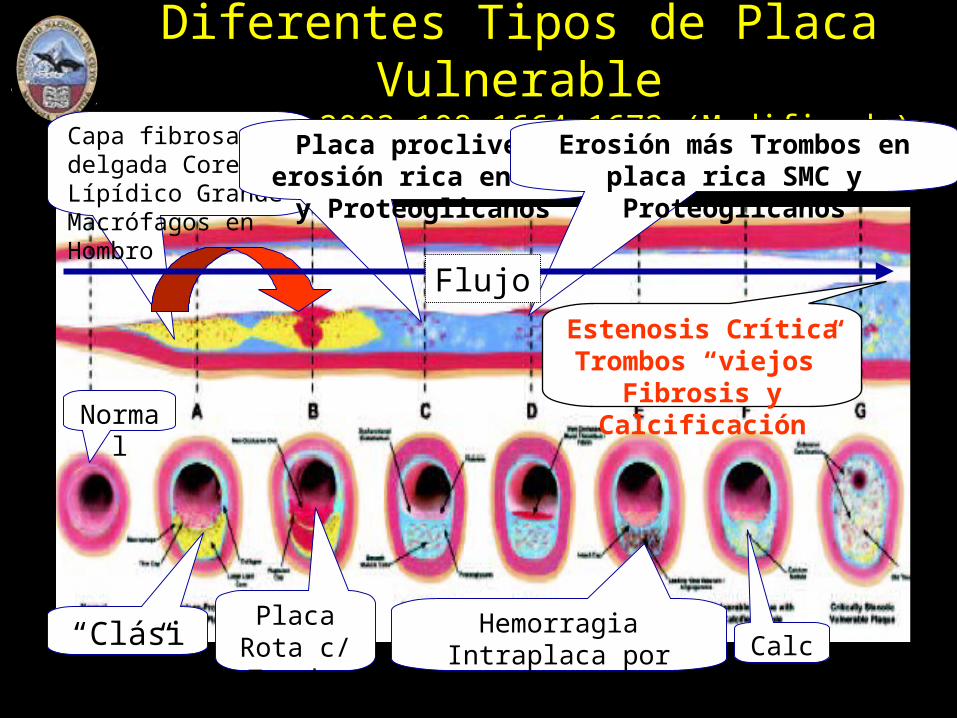
Diferentes Tipos de Placa Vulnerable Circulation 2003;108:1664-1672 (Modificado)
Normal
“Clásica”
Capa fibrosa delgada Core Lípídico GrandeMacrófagos en Hombro
Placa Rota c/ Trombo
Placa proclive a erosión rica en SMC y Proteoglicanos
Erosión más Trombos en placa rica SMC y Proteoglicanos
Hemorragia Intraplaca por Ruptura de Vasa Vasorum Calcio
Estenosis CríticaTrombos “viejos”
Fibrosis y Calcificación
Flujo
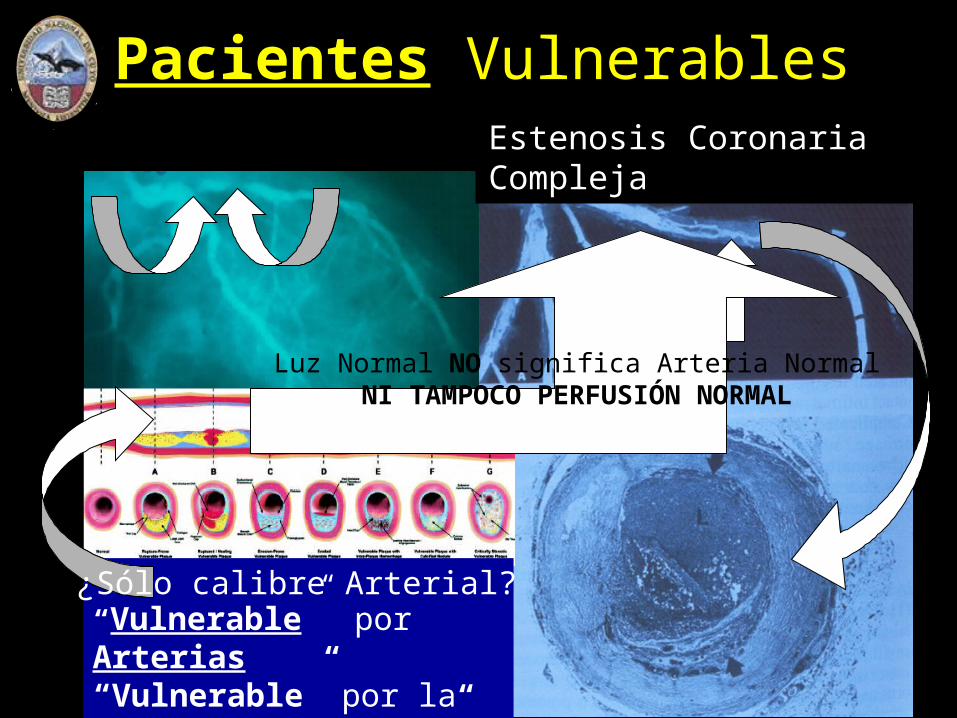
“Vulnerable” por Arterias “Vulnerable” por la Sangre “Vulnerable” por el Miocardio
Luz Normal NO significa Arteria NormalNI TAMPOCO PERFUSIÓN NORMAL
¿Sólo calibre Arterial?
Estenosis Coronaria Compleja
Pacientes Vulnerables

Arteria Permeable (y/u Obstrucción NO crítica) No es igual a Perfusión Adecuada
Prior studies evaluating clinical and ECG outcome measures of reperfusion used angiographic TIMI 2 or 3 flow as the “gold standard”.
Angiographic assessment of epicardial flow is now considered inadequate to completely assess myocardial perfusion.
Indeed, it is now clear that microvascular perfusion may be impaired despite achievement of TIMI 3 flow and less than 50% coronary narrowing; moreover, abnormal microperfusion has negative prognostic implications.
Sigamos aprendiendo con los maestros
Placas InestablesIs There a Vulnerable Plaque?
Attilio Maseri, MD; Valentin Fuster, MD, PhD Circulation. 2003;107:2068-2071.

Patogenia de la Trombosis CoronariaAttilio Maseri, MD; Valentin Fuster, MD, PhD Circulation
2003;107:2068-2071.
Post-mortem studies in patients with ACS show that most culprit thrombi are composed of platelets or platelets and fibrin. Such composition indicates that thrombi formed gradually in flowing blood in response to weak thrombogenic stimuli, leading to local aggregation of platelets which, being only 400000/mm3 of blood, take a long time to accumulate. Often, thrombi are composed of multiple layers of different age, suggestive of recent recurrences of weak thrombogenic stimuli. Less frequently, red thrombi, rich in fibrin and red cells, are found at the site of disrupted plaques with a large pultaceous core, suggesting very strong thrombogenic stimuli. Multilayered platelet thrombi and red thrombi are likely to be related to distinct pathogenetic mechanisms.
Nota: ¿UA - NSTEMI?
Nota: ¿STEMI?
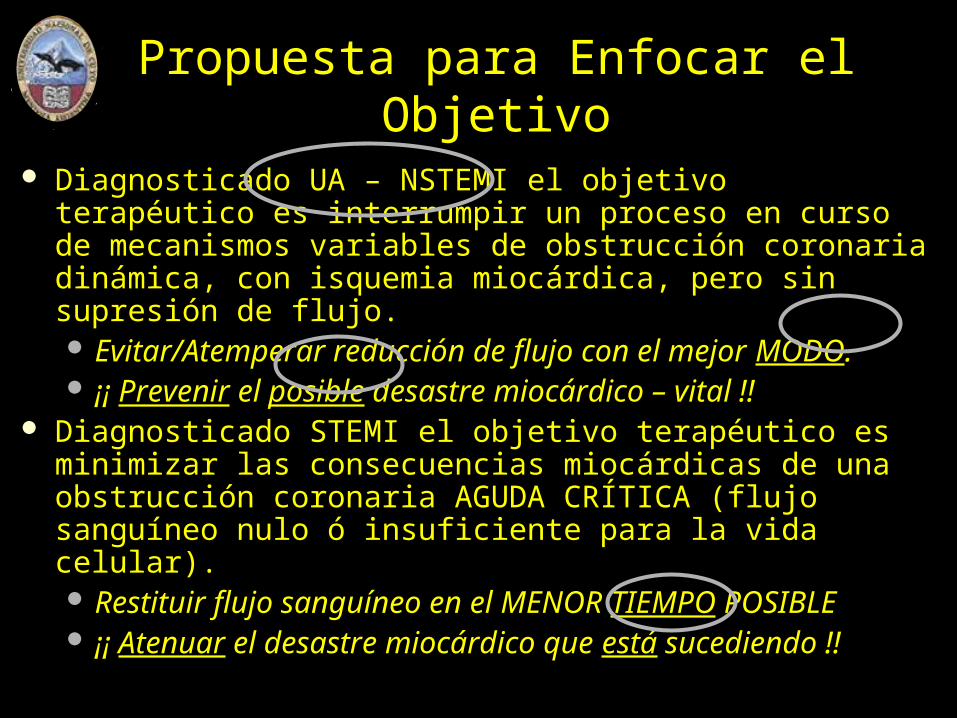
Propuesta para Enfocar el Objetivo
Diagnosticado UA – NSTEMI el objetivo terapéutico es interrumpir un proceso en curso de mecanismos variables de obstrucción coronaria dinámica, con isquemia miocárdica, pero sin supresión de flujo. Evitar/Atemperar reducción de flujo con el mejor MODO. ¡¡ Prevenir el posible desastre miocárdico – vital !!
Diagnosticado STEMI el objetivo terapéutico es minimizar las consecuencias miocárdicas de una obstrucción coronaria AGUDA CRÍTICA (flujo sanguíneo nulo ó insuficiente para la vida celular). Restituir flujo sanguíneo en el MENOR TIEMPO POSIBLE ¡¡ Atenuar el desastre miocárdico que está sucediendo !!
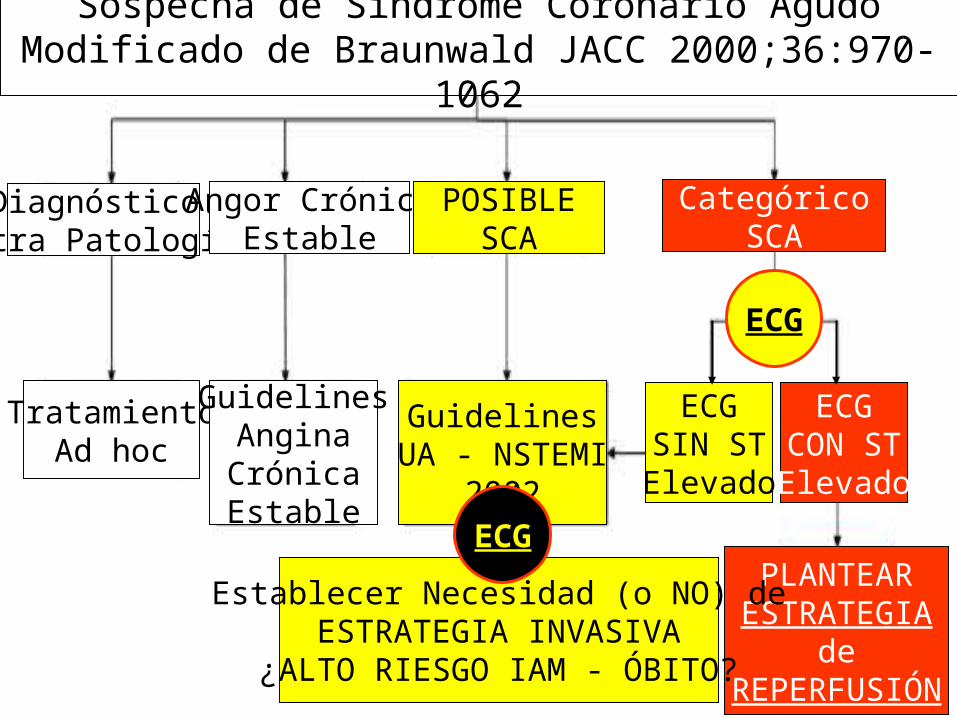
Sospecha de Síndrome Coronario AgudoModificado de Braunwald JACC 2000;36:970-1062
Diagnóstico:Otra Patología
TratamientoAd hoc
Angor CrónicoEstable
GuidelinesAnginaCrónicaEstable
POSIBLESCA
GuidelinesUA - NSTEMI
2002
CategóricoSCA
ECGSIN STElevado
ECGCON STElevado
PLANTEARESTRATEGIA
deREPERFUSIÓN
Establecer Necesidad (o NO) deESTRATEGIA INVASIVA
¿ALTO RIESGO IAM - ÓBITO?
ECG
ECG
ACC/AHA Guidelines (2004) for the Management of Patients WithST-Elevation Myocardial Infarction
A Report of the ACC / AHA Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction) Developed in Collaboration With the Canadian Cardiovascular Society
Single copies of the executive summary published in the August 4, 2004, issue of the JACC or the August 3, 2004, issue of Circulation.
Available at www.acc.org o www.americanheart.org

El Llamado al Servicio de EmergenciaMédico (SEM)
Paciente varón de 58 años que solicita SEM por dolor retroesternal, primera vez, tras emoción violenta, intenso, angustiante, de 20 min de duración con sudoración profusa.
Usted es el médico del SEM:¿Qué hace al tomar contacto con el paciente?Describa el orden de sus procedimientos
Ud Diagnostica STEMI¿Qué tiempos tiene in mente?¿Qué alternativas terapéuticas tiene in mente?
Acortar tiempo Crítico del SCA - STEMIBases para las Normas SEM – Guardia
Médica de la evaluación médica inicial del SCA
Establecer La Probabilidad de Aterosclerosis Coronaria El Perfil de Riesgo Inmediato de IAM – Muerte
¿Cómo establecer Probabilidad y Perfil de Riesgo? Historia Clínica
Características de la Molestia – Dolor: ¡¿ Duración ?!Datos Personales: Sexo y EdadAntecedentes Patológicos: Patología Cardiovascular/ DiabetesExamen Físico: ¿¡Insuficiencia Cardíaca!? - Arteriopatías
ECG Biomarcadores: Troponinas T ó I; CPK–MB ¡Masa!
Clínica más ECG¿Angor>20min? ¿Supra ST? ¡¡Reperfusión!!

¿En qué se emplea (y pierde) el tiempo?
¿Qué objetivos serían razonables?

Demoras admisibles actualmente desde el Contacto SEM (Guardia) - Paciente
Clase IThe delay from patient contact with the healthcare system (arrival at the ED or contact with paramedics) to initiation of fibrinolytic therapy should be less than 30 minutes.
Alternatively, if PCI is chosen, the delay from patient contact with the healthcare system (typically, arrival at the ED, or contact with paramedics) to balloon inflation should be less than 90 minutes. (Level of Evidence: B)
Optimal Strategies for EmergencyDepartment Triage
Class IHospitals should establish multidisciplinary
teams (including primary care physicians, emergency medicine physicians, cardiologists, nurses, and laboratorians) to develop guideline-based, institution-specific written protocols for triaging and managing patients who are seen in the prehospital setting or present to the ED with symptoms suggestive of STEMI. (Level of Evidence: B)
La consulta en la Guardia de un Hopital de la Comunidad
Paciente varón de 28 años que consulta en la Clínica dónde está capitado (sin Alta Complejidad), por dolor precordial, primera vez, punzante, intenso, luego de ejercicio no habitual, angustiante, de 60 min de duración y que aumenta con la inspiración.
Usted es el médico de Guardia:Interprete el siguiente ECG: ECG 1 ECG 2 ECG 3
Historia y ECG semejantes con 58 años ¡¿?!
¿Y si la Molestia no es ANGOR típico?Bases para Normas de Guardia (SEM – Hospital)
Although typical characteristics substantially raise the probability of CAD, features not characteristic of chest pain, such as sharp stabbing pain or reproduction of pain on palpation, do not exclude the possibility of ACS. In the Multicenter Chest Pain Study, acute ischemia was diagnosed in 22% of patients who presented to the ED with sharp or stabbing pain and in 13% of patients with pain with pleuritic qualities. Furthermore, 7% of patients whose pain was fully reproduced with palpation were ultimately recognized to have ACS.
Diagnóstico de STEMIErrores de Admisión y/o “Falso Negativo” In a large study on this subject, Pope et al. found that 889 of
10 689 ( 8,3% de las consultas a Guardia Médica) patients who presented to 10 US hospital EDs with chest pain or other symptoms that suggested acute cardiac ischemia had STEMI.
19 patients (2.1%, 95% CI 1.1% to 3.1%) were discharged from the ED.
Patients with STEMI were more likely not to be hospitalized if they were nonwhite (OR for discharge 4.5; 95% CI 1.8 to 11.8) or had a normal or nondiagnostic ECG (OR 7.7; 95% CI 2.9 to 20.2).
The risk-adjusted mortality ratio for MI patients who were not hospitalized compared with those who were hospitalized was 1.9 (95% CI ¿¿¡ 0.7 !?? to ¡¡ 5.2 !!).
Nosotros: ¿Tenemos algún sesgo discriminatorio?
Otra consulta en la Guardia de un Hopital de la Comunidad
Paciente varón de 60 años que consulta en la Clínica dónde está capitado (sin Alta Complejidad), por dolor precordial, primera vez, opresivo, intenso, luego de ejercicio no habitual, angustiante, de 60 min de duración y que aumenta con la inspiración.
Usted es el médico de Guardia:Interprete el siguiente ECG:
ECG 1 ECG 2 ECG 3 ECG 4 ECG 5 ECG 6 ECG 7
¡A trabajar!
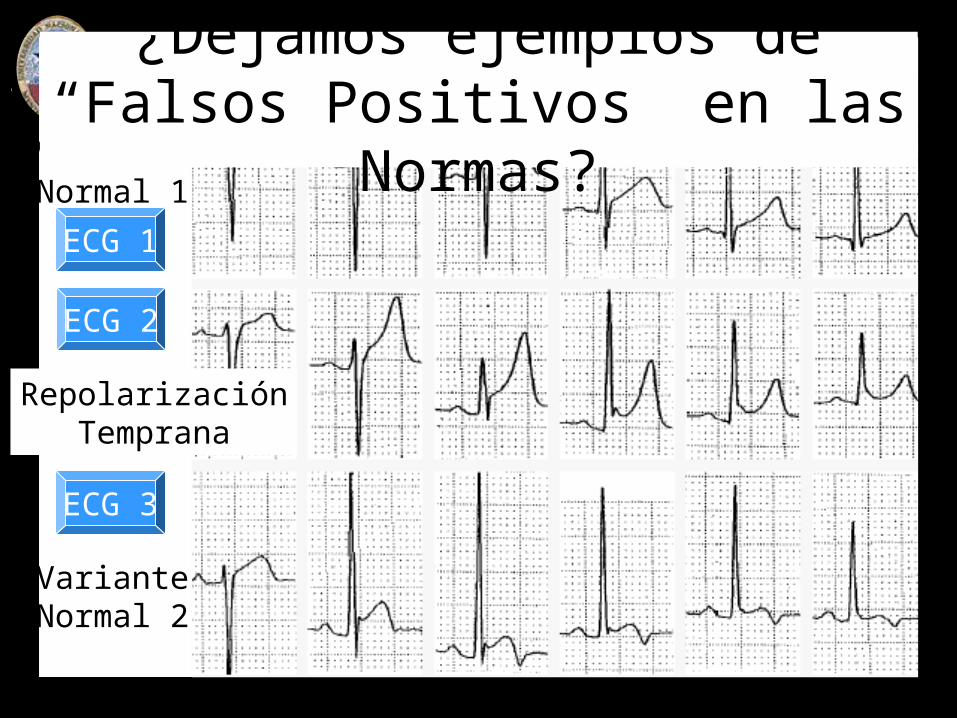
VarianteNormal 1
RepolarizaciónTemprana
VarianteNormal 2
¿Dejamos ejemplos de “Falsos Positivos” en las Normas?
ECG 1
ECG 2
ECG 3
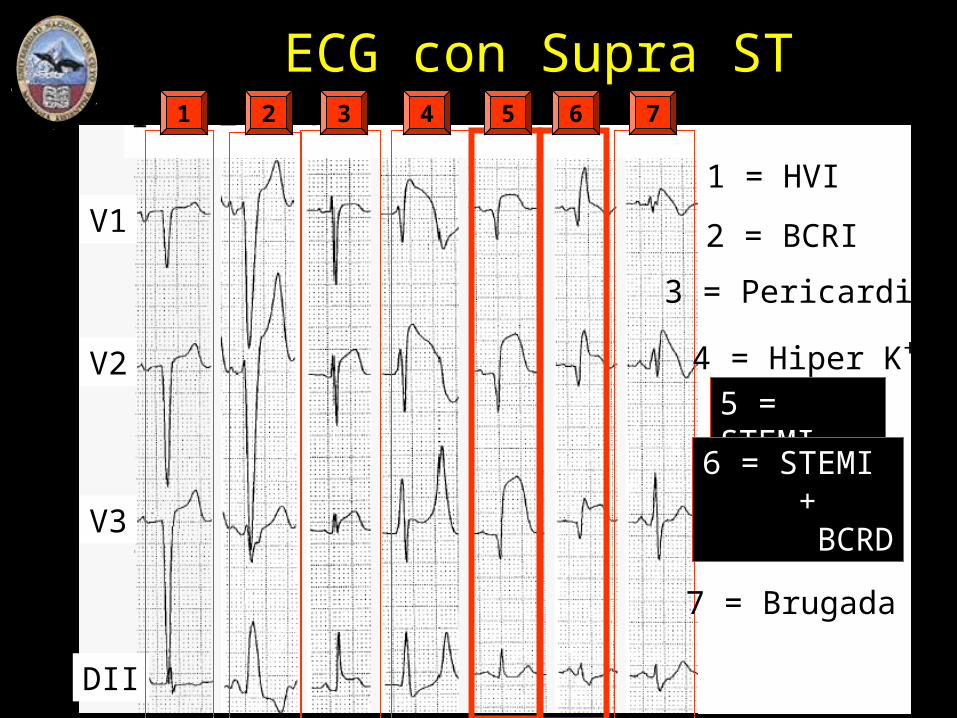
V1
V2
V3
DII
1 2 3 4 5 6 7
1 = HVI
2 = BCRI
3 = Pericarditis
4 = Hiper K+
5 = STEMI
6 = STEMI +
BCRD
7 = Brugada
1 2 3 4 5 6 7
ECG con Supra ST