Embarazo Gemelar y Parto Prematuro ¿Qué podemos hacer en ... · Embarazo Gemelar y Parto...
54
+ Embarazo Gemelar y Parto Prematuro ¿Qué podemos hacer en prevención? Dra. Camila Fernández Niklitschek Residente MMF. 2016
Transcript of Embarazo Gemelar y Parto Prematuro ¿Qué podemos hacer en ... · Embarazo Gemelar y Parto...

+
Embarazo Gemelar y Parto Prematuro ¿Qué podemos hacer en prevención?
Dra. Camila Fernández Niklitschek Residente MMF. 2016

+Importancia PP Gemelar
Predicción PP
Longitud cervical y Fibronectina
Prevención PP
Progesterona
Cerclaje
Pesario
Conclusiones

+Introducción
n Incidencia 1 a 2% (Chile 2009 1,84%).
n 1 cada 70-90 embarazos
n En aumento
n Alto riesgo Obstetrico n 10% de toda la morbimortalidad perinatal.
S.G. Brubaker and C. Gyamfi. Prediction and Prevention of Spontaneous Preterm Birth in Twin Gestations. Semin Perinatol 36:190-194 © 2012 Elsevier
Gonzalez R. Et al. ¿Existe un aumento de los nacimientos en chile en el período 2000-2009?. Rev chil obstet ginecol 2011; 76(6): 404 – 411.

+Introducción
n Parto prematuro en EEUU: n 85% de la morbi-mortalidad perinatal n Costo de 5,6 millones de dólares por año. n Aumento del 20% en los últimos 15 años.
n Gemelar y PP 50% (vs único)
n Embarazo Múltiple n 3% Nacimientos en EEUU n 17% de los < 37 sem n 23% de los < 32 sem.
S.G. Brubaker and C. Gyamfi. Prediction and Prevention of Spontaneous Preterm Birth in Twin Gestations. Semin Perinatol 36:190-194 © 2012 Elsevier

+Introducción Chile
408 REV CHIL OBSTET GINECOL 2011; 76(6)
Tabla IVEVOLUCIÓN DEL EMBARAZO MÚLTIPLE Y PREMATUREZ. CHILE 2000-2009
Año
2000200120022003200420052006200720082009
NV
248350245698238678234005229021230366231218239958245661251187
Múltiples =2
1,661,781,781,771,741,751,771,811,871,84
Múltiples >2
0,060,050,050,050,050,040,050,040,040,05
Total múltiples
1,721,831,831,821,791,791,831,851,911,89
<37 s (%)
50,5651,1953,4854,2957,3259,0859,4960,0861,8962,47
32-36 s (%)
43,1043,7845,3845,8149,6649,8348,9349,6352,0452,60
NV: nacidos vivos.
Año
2000200120022003200420052006200720082009
Tabla V aEVOLUCIÓN DEL PESO AL NACER. CHILE 2000-2009
NV
247816245396238479233887228849230244231050239958245660251187
PN (g)
3355335833523353335133353324333433263334
BPN (%)
5,185,205,375,545,635,425,725,735,905,91
MBPN (%)
0,820,820,880,950,930,941,050,991,020,99
PN<p10
7,527,317,367,267,136,976,977,006,947,10
PN<p3
2,182,092,082,022,001,741,821,841,811,84
PN>p90
9,429,529,389,389,128,108,888,748,828,78
NV: nacidos vivos totales. PN: mediana del peso al nacer. BPN: bajo peso al nacer (<2500 g). MBPN: muy bajo peso al nacer (<1500 g). PN<p10: peso bajo percentil 10, Alexander (%). PN<p3: peso bajo percentil 3, Oken (%). PN>p90: peso sobre percentil 90, Alexander (%).
Tabla V bEVOLUCIÓN DE LA MORTALIDAD NEONATAL PRECOZ SEGÚN PESO AL NACER. CHILE 2000-2009
Año
2000200120022003200420052006200720082009
MNP / BPN
63,1454,0050,5055,7956,0260,3053,1955,4956,0952,24
MNP / MBPN
320,10284,33243,92276,13313,22310,43254,14287,49285,35279,32
MNP / <p10
15,4413,3613,7715,5914,5515,4114,1514,2116,3113,59
MNP / <p3
26,8023,3822,7130,9325,1125,5819,9721,7022,9323,49
MNP / >p90
1,461,031,571,101,581,292,051,341,341,23
MNP: mortalidad neonatal precoz (x 1000 NV). BPN: bajo peso al nacer (<2500 g). MBPN: muy bajo peso al nacer (<1500 g). <p10: peso bajo percentil 10, Alexander (%). <p3: peso bajo percentil 3, Oken (%). >p90: peso sobre percentil 90, Alexander (%).
Aumento 11% del total de embarazos múltiples. Aumento 12% en la prematurez de embarazos múltiples.
Gonzalez R. Et al. ¿Existe un aumento de los nacimientos en chile en el período 2000-2009?. Rev chil obstet ginecol 2011; 76(6): 404 – 411.

+Predicción parto prematuro

+Factores de Riesgo
n Embarazos únicos pesquisa 20-30% población.
n Embarazos Múltiples poca asociación n Longitud Cervical n Fibronectina n Infección Tracto urinario
Goldenberg RL, Iams JD, Miodovnik M, et al: The preterm prediction study: Risk factors in twin gestations. National Institute of Child Health and Human Development maternal-Fetal medicine units network. Am J Obstet Gynecol 175:1047-1053, 1996

+Longitud Cervical
n ¿Es Útil en Embarazo Gemelar?
n ¿Qué punto de corte deberíamos usar?
n ¿Cuándo realizarlo?

+¿Qué punto de corte usar?
LC (mm)
Sensibilidad
Especificidad
35 78% 66%
30 41% 87%
25 36% 94%
20 30% 94%
14 Lim et al.
Table 2 Study quality
Study Design
Adequatedescription oftest procedure
Cut-off pointsdeterminedwith ROCcurve
Practitionerblinded tomeasurementresults
Interventionbased oncervicallength
Exclusion ofpatients withintervention orindicated PTB
Arabin et al.20 Prospective cohort Yes Unclear No Yes YesFait et al.21 Retrospective cohort Yes No Unclear No YesGibson et al.22 Prospective cohort Yes Yes Yes No YesGoldenberg et al.23 Prospective cohort Yes No Yes No NoGuzman et al.24 Prospective cohort No Yes No Yes YesGuzman et al.35 Prospective cohort No Yes No Yes YesImseis et al.25 Retrospective cohort Yes Yes No Yes YesKlein et al.26 Retrospective cohort Yes Unclear Unclear No UnclearMaslovitz et al.36 Retrospective cohort Yes No No Unclear YesMaymon et al.37 Prospective cohort Yes Yes Unclear Unclear YesMcMahon et al.27 Prospective cohort No Yes* Yes No YesMissfelder-Lobos et al.38 Retrospective cohort Yes No† No Yes UnclearNaba28 Prospective cohort No Unclear Unclear Unclear NoRobyr et al.29 Retrospective cohort No No No Yes YesSayin et al.30 Retrospective cohort Yes No No Yes UnclearSoriano et al.31 Prospective cohort Yes Unclear Yes No YesSouka et al.32 Retrospective cohort Yes No No Yes YesSperling et al.33 Prospective cohort Yes No No‡ Yes YesTo et al.39 Retrospective cohort Yes No No Yes YesVayssiere et al.34 Prospective cohort Yes Yes Yes No NoYang et al.9 Prospective cohort Yes No No Yes Yes
*Cut-off point determined with receiver–operating characteristics (ROC) curve at 27 mm, but adjusted to 30 mm for optimal clinicalusefulness. †No cut-off points used, original data available. ‡Measurements ! 5 mm were blinded to the caregiver, patients withmeasurements < 15 mm received treatment. PTB, preterm birth.
1.00
0.75
0.50
0.25
0
Sens
itivi
ty
0.25 0.50 0.75 1.001 – Specificity
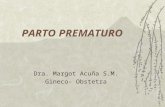
Figure 2 Summary receiver–operating characteristics curve for allstudies (twin and triplet). Reported accuracy: preterm birth at: ,34–37 weeks; , 30–34 weeks; , < 30 weeks; gestational age atcervical length measurement: , < 20 weeks; , 20–24 weeks; ,> 24 weeks; cervical length cut-off: , 20 mm; , 25 mm;
, 30 mm; , 35 mm. , Estimated accuracy, summaryreceiver–operating characteristics curve.
Data analysis
Figure 2 shows an ROC space of the individual studies, aswell as the bootstrapped sROC curve plot for all studiesin asymptomatic women with a twin or triplet pregnancy.
1.00
0.75
0.50
0.25
0
Sens
itivi
ty
0.25 0.50 0.75 1.001 – Specificity
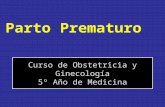
Figure 3 Summary receiver–operating characteristics space fordifferent cut-off points of cervical length. Reported accuracy forcervical length in individual studies: , 35 mm; , 30 mm;, 25 mm; , 20 mm. Summary receiver–operating characteristics
per cut-off: , 35 mm; , 30 mm; , 25 mm; , 20 mm., 95% CIs.
Studies in which cervical length was measured before20 weeks show an overall high specificity, but sensitivityin these studies does not exceed 70%. The overall sROCcurve shows a moderate accuracy, with sensitivity beingslightly better than specificity.
Figure 3 shows summary point estimates for sensitivityand specificity with 95% CIs for four different cut-offs
Copyright ! 2011 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2011; 38: 10–17.
Predicción PP < 34 sem
Cervical length measurement for the prediction of preterm birth in multiple pregnancies: a systematic review and bivariate meta-analysis. A. C. LIM, Ultrasound Obstet Gynecol 2011; 38: 10–17.

+
tween 0.56-1.17, respectively, to predictspontaneous preterm birth from !32 to!37 weeks of gestation in asymptomaticwomen by using cutoff values for CLranging between 20-35 mm at 20-24weeks of gestation. Pooled positive andnegative likelihood ratios for predictingpreterm birth at !34 weeks of gestationin asymptomatic women using cutoffvalues for CL ranging between 25-35mm at "24 weeks of gestation varied be-tween 1.8-2.1 and between 0.29-0.83, re-spectively. This review, however, in-cluded 2 studies with duplicate data and1 study in which a cervical cerclage wasplaced in women with a CL !30 mm at!27 weeks of gestation.
The results of our systematic reviewsuggest that transvaginal sonographicmeasurement of CL is a better predictorof spontaneous preterm birth in twinpregnancies than in singleton pregnan-cies. In fact, the metaanalysis by Honestet al4 reported that among asymptomaticwomen with singleton pregnancies, a CL!25 mm at 20-24 weeks of gestation hadpooled positive and negative likelihoodratios of 4.2 and 0.40, and 4.4 and 0.67,respectively, to predict preterm birth!32 and !34 weeks of gestation, respec-
tively. At !20 weeks of gestation, a CL!25 mm had pooled positive and nega-tive likelihood ratios of 4.1 and 0.75, and6.3 and 0.79, respectively, to predict pre-term birth !32 and !34 weeks of gesta-tion, respectively, whereas at "24 weeksof gestation the pooled positive and neg-ative likelihood ratios for predicting pre-term birth at !34 weeks of gestationwere 4.1 and 0.62, respectively. In con-trast, the present study showed thatamong asymptomatic women with twinpregnancies, a CL !20 mm at 20-24weeks of gestation had pooled positiveand negative likelihood ratios of 10.1 and0.64, and 9.0 and 0.64, respectively, topredict preterm birth at !32 and !34weeks of gestation, respectively.
Although our metaanalyses have dem-onstrated that transvaginal sonographicmeasurement of CL is predictive of pre-term birth in asymptomatic women withtwin pregnancies, it is unclear if antena-tal management of these pregnanciesbased on the results of this test can pre-vent preterm birth. In 2006, Gordon etal42 conducted a study in which 125women with twin pregnancies were ran-domly assigned to undergo a transvagi-nal sonographic CL measurement and a
cervical digital examination every 4weeks starting at 16-20 weeks until 28weeks of gestation (n # 63) or to a digitalcervical examination without cervical as-sessment by ultrasound at the same in-tervals (n # 62). Women who under-went transvaginal sonographic cervicalexaminations were treated with a prede-termined algorithm for the use of cer-clage and bed rest. Treatment decisionsof women allocated to the control groupwere not based upon a predetermined al-gorithm. There was no significant differ-ence between groups in mean length ofgestation (35.7 $ 2.2 weeks in the studygroup vs 35.5 $ 3.1 weeks in the controlgroup, P # .60) but life table analysis re-vealed that preterm birth !35 weeks ofgestation in the transvaginal sono-graphic CL group was significantly re-duced (P # .02). In addition, it should beemphasized that as of late 2009, there is notherapy that effectively prevents pretermbirth in twin pregnancies. This includesthe use of bed rest,43 oral betamimetics,44
cervical cerclage,45 and progesterone.46
Further well-designed randomizedcontrolled trials are required to evaluatethe effectiveness of antenatal treatmentof women with twin pregnancies based
TABLE 3Pooled estimates of pretest probabilities, likelihood ratios, and posttest probabilities for cervicallength in prediction of spontaneous preterm birth in women with twin pregnancies
OutcomeCervical lengthcutoff, mm
Pretestprobability, %
Likelihood ratios Posttest probabilities, %
Positive testresult
Negative testresult
Positive testresult
Negative testresult
Asymptomatic women (testing at 20-24 wks’ gestation).......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !28 wk 25 3.5 9.6 0.40 25.8 1.4.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !32 wk 20 6.8 10.1 0.64 42.4 4.5.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !34 wk 20 15.3 9.0 0.74 61.9 11.8.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !37 wk 25 41.2 4.4 0.83 75.5 36.8................................................................................................................................................................................................................................................................................................................................................................................
Asymptomatic women (testing "24 wks’ gestation).......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !32 wk 25 6.1 2.7 0.47 14.9 3.0.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !34 wk 25 18.2 2.3 0.70 33.9 13.5.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !37 wk 25 53.6 1.8 0.75 67.5 46.4................................................................................................................................................................................................................................................................................................................................................................................
Women with symptoms of threatened labor.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !34 wk 30 35.9 1.2 0.67 40.2 27.3.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !37 wk 25 67.2 1.9 0.69 79.6 58.6................................................................................................................................................................................................................................................................................................
30 67.2 1.2 0.65 71.1 57.1................................................................................................................................................................................................................................................................................................................................................................................Conde-Agudelo. Transvaginal sonographic CL for the prediction of spontaneous preterm birth in twin pregnancies. Am J Obstet Gynecol 2010.
www.AJOG.org Obstetrics Research
AUGUST 2010 American Journal of Obstetrics & Gynecology 128.e10

+Longitud Cervical
n Máxima acuciosidad en predicción PP < 32 sem LC <20 mm realizada 20-24 sem
n Máxima acuciosidad en predicción PP < 28 sem LC < 25 mm. n Ventaja: mayor sensibilidad
n Alta frecuencia PP en gemelar, PP extremo mayor importancia
Sensibilidad 39%
Especificidad 96%
VPP 96%
VPN 97%
Conde-Agudelo A, Romero R, Hassan SS, et al. Transvaginal sonographic cervical length for the prediction of spontaneous preterm birth in twin pregnancies: a systematic review and metaanalysis. Am J Obstet Gynecol 2010;203:128.e1-12
25 mm

+Longitud Cervical
n Buen predictor PP cuando se realiza 24 sem
n LC < 20mm buen predictor PP <32 y 34 sem
n LC < 25 mm buen predictor PP < 28 sem
n Problema: n Cervicometria normal No reduce mayormente riesgo PP n LC poco útil como predictor PP en mujeres con SPP o
cervicometria realizada > 24 sem EG.
tween 0.56-1.17, respectively, to predictspontaneous preterm birth from !32 to!37 weeks of gestation in asymptomaticwomen by using cutoff values for CLranging between 20-35 mm at 20-24weeks of gestation. Pooled positive andnegative likelihood ratios for predictingpreterm birth at !34 weeks of gestationin asymptomatic women using cutoffvalues for CL ranging between 25-35mm at "24 weeks of gestation varied be-tween 1.8-2.1 and between 0.29-0.83, re-spectively. This review, however, in-cluded 2 studies with duplicate data and1 study in which a cervical cerclage wasplaced in women with a CL !30 mm at!27 weeks of gestation.
The results of our systematic reviewsuggest that transvaginal sonographicmeasurement of CL is a better predictorof spontaneous preterm birth in twinpregnancies than in singleton pregnan-cies. In fact, the metaanalysis by Honestet al4 reported that among asymptomaticwomen with singleton pregnancies, a CL!25 mm at 20-24 weeks of gestation hadpooled positive and negative likelihoodratios of 4.2 and 0.40, and 4.4 and 0.67,respectively, to predict preterm birth!32 and !34 weeks of gestation, respec-
tively. At !20 weeks of gestation, a CL!25 mm had pooled positive and nega-tive likelihood ratios of 4.1 and 0.75, and6.3 and 0.79, respectively, to predict pre-term birth !32 and !34 weeks of gesta-tion, respectively, whereas at "24 weeksof gestation the pooled positive and neg-ative likelihood ratios for predicting pre-term birth at !34 weeks of gestationwere 4.1 and 0.62, respectively. In con-trast, the present study showed thatamong asymptomatic women with twinpregnancies, a CL !20 mm at 20-24weeks of gestation had pooled positiveand negative likelihood ratios of 10.1 and0.64, and 9.0 and 0.64, respectively, topredict preterm birth at !32 and !34weeks of gestation, respectively.
Although our metaanalyses have dem-onstrated that transvaginal sonographicmeasurement of CL is predictive of pre-term birth in asymptomatic women withtwin pregnancies, it is unclear if antena-tal management of these pregnanciesbased on the results of this test can pre-vent preterm birth. In 2006, Gordon etal42 conducted a study in which 125women with twin pregnancies were ran-domly assigned to undergo a transvagi-nal sonographic CL measurement and a
cervical digital examination every 4weeks starting at 16-20 weeks until 28weeks of gestation (n # 63) or to a digitalcervical examination without cervical as-sessment by ultrasound at the same in-tervals (n # 62). Women who under-went transvaginal sonographic cervicalexaminations were treated with a prede-termined algorithm for the use of cer-clage and bed rest. Treatment decisionsof women allocated to the control groupwere not based upon a predetermined al-gorithm. There was no significant differ-ence between groups in mean length ofgestation (35.7 $ 2.2 weeks in the studygroup vs 35.5 $ 3.1 weeks in the controlgroup, P # .60) but life table analysis re-vealed that preterm birth !35 weeks ofgestation in the transvaginal sono-graphic CL group was significantly re-duced (P # .02). In addition, it should beemphasized that as of late 2009, there is notherapy that effectively prevents pretermbirth in twin pregnancies. This includesthe use of bed rest,43 oral betamimetics,44
cervical cerclage,45 and progesterone.46
Further well-designed randomizedcontrolled trials are required to evaluatethe effectiveness of antenatal treatmentof women with twin pregnancies based
TABLE 3Pooled estimates of pretest probabilities, likelihood ratios, and posttest probabilities for cervicallength in prediction of spontaneous preterm birth in women with twin pregnancies
OutcomeCervical lengthcutoff, mm
Pretestprobability, %
Likelihood ratios Posttest probabilities, %
Positive testresult
Negative testresult
Positive testresult
Negative testresult
Asymptomatic women (testing at 20-24 wks’ gestation).......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !28 wk 25 3.5 9.6 0.40 25.8 1.4.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !32 wk 20 6.8 10.1 0.64 42.4 4.5.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !34 wk 20 15.3 9.0 0.74 61.9 11.8.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !37 wk 25 41.2 4.4 0.83 75.5 36.8................................................................................................................................................................................................................................................................................................................................................................................
Asymptomatic women (testing "24 wks’ gestation).......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !32 wk 25 6.1 2.7 0.47 14.9 3.0.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !34 wk 25 18.2 2.3 0.70 33.9 13.5.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !37 wk 25 53.6 1.8 0.75 67.5 46.4................................................................................................................................................................................................................................................................................................................................................................................
Women with symptoms of threatened labor.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !34 wk 30 35.9 1.2 0.67 40.2 27.3.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !37 wk 25 67.2 1.9 0.69 79.6 58.6................................................................................................................................................................................................................................................................................................
30 67.2 1.2 0.65 71.1 57.1................................................................................................................................................................................................................................................................................................................................................................................Conde-Agudelo. Transvaginal sonographic CL for the prediction of spontaneous preterm birth in twin pregnancies. Am J Obstet Gynecol 2010.
www.AJOG.org Obstetrics Research
AUGUST 2010 American Journal of Obstetrics & Gynecology 128.e10
Cervical length measurement for the prediction of preterm birth in multiple pregnancies: a systematic review and bivariate meta-analysis. A. C. LIM, Ultrasound Obstet Gynecol 2011; 38: 10–17.

+Longitud Cervical Datos Nacionales: HSR
n Estudio prospectivo de embarazo gemelar entre Enero de 2010 y Julio de 2013 en el CIMAF del Hospital Sotero del Río.
n Medición LC cada 2 sem a partir de las 14 sem de gestación
n Para el análisis se utilizó el método LMS usando el LMS ChartMaker.
n 175 embarazos gemelares n 63% (111) Bicoriales-biamnióticos n 35% (61) Monocoriales-biamnióticos
n 2% (3) Monocoriales-monoamnióticos.
Determinación de los valores normales de la longitud cervical en embarazos gemelares entre las 20-24 semanas. Fernández C, Vargas P, Díaz F, Silva K, Vera C, Kusanovic JP.

+Distribución Normal de la Longitud Cervical 20-24 sem
EG P5 p10 p25 p50 p75 p90 p95 20 sem 24 28 33 38 43 46 48
21 sem 22 26 33 38 43 46 49
22 sem 19 25 32 38 43 46 48
23 sem 17 24 31 37 42 46 48
24 sem 13 22 30 37 42 46 48
Determinación de los valores normales de la longitud cervical en embarazos gemelares entre las 20-24 semanas. Fernández C, Vargas P, Díaz F, Silva K, Vera C, Kusanovic JP.

+Acortamiento Longitud Cervical
patients in group A delivered at significantly earlier gestationalages compared with the patients in group B (Table 2). Thedifference between the groups remained statistically significanteven after excluding data from patients who presented with a shortcervix (CL ! 25 mm) on the second ultrasound assessment of theCL (Tables 2 and 3).
Multiple logistic regression model was performed, controllingfor age, parity, gestational diabetes, confirmed urinary tractinfection, prior PTB, in vitro fertilization and chorionicity. Cervicalshortening of "25% was the only factor significantly associatedwith spontaneous PTB with a gestation time of <32 weeks (crudeOR (95% CI) 14.71 (6.25–36.18); P-value < 0.001, adjusted OR (95%CI) 20.26 (7.93–56.91); P-value < 0.001). This result is still trueafter excluding the women with a CL ! 25 mm on the secondultrasound assessment of the CL.
There was a >7-fold increase in the rate of spontaneous pretermbirth at <32 weeks, from 4 to 28.6% (OR, 9.54; 95% CI, 3.32–27.36)(Table 2). This result is still true after excluding the women with aCL ! 25 mm from 3.5 to 26.3% (OR, 9.76; CI, 2.64–36.04) (Table 3).
The use of CL shortening by "25% has better sensitivity than theuse of CL ! 25 mm for the prediction of PTB at <28, <30, <32, and<34 weeks of gestation, respectively, but the prediction specificityis higher for CL!25 mm for the same gestation periods (Table 4).The sensitivity, specificity, and positive and negative predictivevalue of CL shortening by "25%, were 58.8%, 87%, 28.57%, and95.97%, respectively, for the prediction of spontaneous PTB at <32weeks gestation. The rates of delivery at <32 weeks of gestationwere 28.6% (unadjusted OR, 6.33; 95% CI, 1.111–36.102, and 15.4%;unadjusted OR, 5.697; 95% CI, 1.028–31.559) when the cervixmeasured !2.5 cm at 24 and 28 weeks of gestation, respectively.
Based on ROC curve analysis, the use of CL shortening by "25%was superior, but not statistically significantly, to the use of CL forthe prediction of PTB at <32 (Fig. 1 graph C, P = 0.0524), and at <34weeks (Fig. 1 graph D, P = 0.281). CL, however, was preferred for theprediction of PTB at <28 (Fig. 1 graph A, P = 0.037) and <30 weeks(Fig. 1 graph B, P = 0.0457).
4. Comment
This study confirmed the association between the shortening ofCL by "25% over two measurements and PTB in asymptomatic twinpregnancies. This test was found to be a good predictor of PTB at <28,<30, <32, and <34 weeks’ gestation. This result remained true evenafter excluding women with a short cervix (CL ! 25 mm) on the
repeated CL. Our results are similar to and consistent with those ofFox et al. [7], who found that a CL that decreases by "20% over 2measurements is a significant predictor of spontaneous pretermbirth at <28, <30, <32, and <34 weeks. This effect remained trueeven when excluding patients who exhibited a CL ! 25 mm.
With the use of CL shortening by "20% in the Fox et al. study [7],the sensitivity was 75, 60, 54.5, and 35%, and the specificity was86.3, 86.2, 88.1, and 88.1% for the prediction of PTB < 28, <30, <32,and <34 weeks respectively. Our cutoff point of CL shortening by"25% is better for the prediction of PTB < 32 and <34 weeks thanthe "20% cutoff point used by Fox et al. [7], but the "20% cutoffpoint is better for the prediction of PTB < 28 and <30 weeks.
Our study differs from both Fox et al. [7], and other previousstudies [2–6] in that we evaluated both the CL and the percentchange in CL over time to predict PTB. There are several studies thatexamined the use of single or repeated cervical length measurementas a predictor of PTB in twin gestations. Although predictiveaccuracy varies between studies, shortened cervical length usuallyhas a low sensitivity but high positive predictive value for PTB [2–6].
Goldenberg et al. [3] studied 147 sets of twins and found thatthe rates of delivery at <32 weeks of gestation were 26.9% and13.2% when the cervix measured !2.5 cm at 24 and 28 weeks ofgestation, respectively [3]. We almost have similar results, but thenumber of patients with short CL ! 25 mm in our study were only20 cases in total, which is smaller than the number in theGoldenberg et al. [3] study with 26 cases at 24 weeks and 48 casesat 28 weeks.
Souka et al. [4] found that a cervical length of !25 mm at 23weeks had sensitivities for predicting spontaneous PTB at <28, <30,<32, and <34 weeks’ gestation of 100, 80, 47, and 35%, respectively.Although our established variable of CL shortening by "25%between the two measurements have better sensitivity than theuse of the CL by Souka et al. [4] to predict PTB at <32 and 34 weeks, itwas not as effective as Souka et al.’s method at predictingspontaneous PTB at <28 and <30 weeks’ gestation. It is possiblethat the small number of patients who were delivered at <28 weeks(4 patients) and <30 weeks (5) acted as a limiting factor in our study.
In our study the high specificities and the high negativepredictive values of CL shortening by "25% for the prediction ofspontaneous PTB at <32 weeks’ gestation indicate that CLshortening was better at predicting the absence than the presenceof various degrees of spontaneous prematurity. Therefore, patientscan be informed and reassured that the risk of very PTB is quite low,potentially avoiding hospitalization, bed rest, and overtreatment.
Table 3Outcomes in all women with cervical length > 25 mm at the second examination in both groups.
Gestational age at CL shortening by "25% CL shortening by <25% P value
Delivery in weeks with cervical length > 25 mmN = 19
with cervical length > 25 mmN = 170
<28 weeks 2 (10.5%) 1 (0.6%) 0.0203"28 to <30 weeks 3 (15.8%) 2 (1.2%) 0.026"30 to <32 weeks 5 (26.3%) 6 (3.5%) <0.001"32 to <34 weeks 7 (36.8%) 17 (10.0%) 0.029"34 2 (10.5%) 144 (84.7%) <0.001
N, number; CL, cervical length.
Table 4Sensitivity and specificity for spontaneous delivery at <28, 30, 32, and 34 weeks gestation according to CL ! 25 mm, and the change in the cervical length by "25%.
<28 weeks "28 to <30 weeks "30 to <32 weeks "32 to <34 weeks
Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity
CL change by "25% 66.67 84.7 55.56 85 58.8 87 45.2 88.2CL ! 25 mm 50 91.6 44.4 92 53.3 92.7 22.6 92.7
CL, cervical length.
M.I. Khalil et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology xxx (2013) xxx–xxx 3
G Model
EURO-8017; No. of Pages 4
Please cite this article in press as: Khalil MI, et al. The use of cervical length and change in cervical length for prediction of spontaneouspreterm birth in asymptomatic twin pregnancies. Eur J Obstet Gynecol (2013), http://dx.doi.org/10.1016/j.ejogrb.2013.02.019
patients in group A delivered at significantly earlier gestationalages compared with the patients in group B (Table 2). Thedifference between the groups remained statistically significanteven after excluding data from patients who presented with a shortcervix (CL ! 25 mm) on the second ultrasound assessment of theCL (Tables 2 and 3).
Multiple logistic regression model was performed, controllingfor age, parity, gestational diabetes, confirmed urinary tractinfection, prior PTB, in vitro fertilization and chorionicity. Cervicalshortening of "25% was the only factor significantly associatedwith spontaneous PTB with a gestation time of <32 weeks (crudeOR (95% CI) 14.71 (6.25–36.18); P-value < 0.001, adjusted OR (95%CI) 20.26 (7.93–56.91); P-value < 0.001). This result is still trueafter excluding the women with a CL ! 25 mm on the secondultrasound assessment of the CL.
There was a >7-fold increase in the rate of spontaneous pretermbirth at <32 weeks, from 4 to 28.6% (OR, 9.54; 95% CI, 3.32–27.36)(Table 2). This result is still true after excluding the women with aCL ! 25 mm from 3.5 to 26.3% (OR, 9.76; CI, 2.64–36.04) (Table 3).
The use of CL shortening by "25% has better sensitivity than theuse of CL ! 25 mm for the prediction of PTB at <28, <30, <32, and<34 weeks of gestation, respectively, but the prediction specificityis higher for CL!25 mm for the same gestation periods (Table 4).The sensitivity, specificity, and positive and negative predictivevalue of CL shortening by "25%, were 58.8%, 87%, 28.57%, and95.97%, respectively, for the prediction of spontaneous PTB at <32weeks gestation. The rates of delivery at <32 weeks of gestationwere 28.6% (unadjusted OR, 6.33; 95% CI, 1.111–36.102, and 15.4%;unadjusted OR, 5.697; 95% CI, 1.028–31.559) when the cervixmeasured !2.5 cm at 24 and 28 weeks of gestation, respectively.
Based on ROC curve analysis, the use of CL shortening by "25%was superior, but not statistically significantly, to the use of CL forthe prediction of PTB at <32 (Fig. 1 graph C, P = 0.0524), and at <34weeks (Fig. 1 graph D, P = 0.281). CL, however, was preferred for theprediction of PTB at <28 (Fig. 1 graph A, P = 0.037) and <30 weeks(Fig. 1 graph B, P = 0.0457).
4. Comment
This study confirmed the association between the shortening ofCL by "25% over two measurements and PTB in asymptomatic twinpregnancies. This test was found to be a good predictor of PTB at <28,<30, <32, and <34 weeks’ gestation. This result remained true evenafter excluding women with a short cervix (CL ! 25 mm) on the
repeated CL. Our results are similar to and consistent with those ofFox et al. [7], who found that a CL that decreases by "20% over 2measurements is a significant predictor of spontaneous pretermbirth at <28, <30, <32, and <34 weeks. This effect remained trueeven when excluding patients who exhibited a CL ! 25 mm.
With the use of CL shortening by "20% in the Fox et al. study [7],the sensitivity was 75, 60, 54.5, and 35%, and the specificity was86.3, 86.2, 88.1, and 88.1% for the prediction of PTB < 28, <30, <32,and <34 weeks respectively. Our cutoff point of CL shortening by"25% is better for the prediction of PTB < 32 and <34 weeks thanthe "20% cutoff point used by Fox et al. [7], but the "20% cutoffpoint is better for the prediction of PTB < 28 and <30 weeks.
Our study differs from both Fox et al. [7], and other previousstudies [2–6] in that we evaluated both the CL and the percentchange in CL over time to predict PTB. There are several studies thatexamined the use of single or repeated cervical length measurementas a predictor of PTB in twin gestations. Although predictiveaccuracy varies between studies, shortened cervical length usuallyhas a low sensitivity but high positive predictive value for PTB [2–6].
Goldenberg et al. [3] studied 147 sets of twins and found thatthe rates of delivery at <32 weeks of gestation were 26.9% and13.2% when the cervix measured !2.5 cm at 24 and 28 weeks ofgestation, respectively [3]. We almost have similar results, but thenumber of patients with short CL ! 25 mm in our study were only20 cases in total, which is smaller than the number in theGoldenberg et al. [3] study with 26 cases at 24 weeks and 48 casesat 28 weeks.
Souka et al. [4] found that a cervical length of !25 mm at 23weeks had sensitivities for predicting spontaneous PTB at <28, <30,<32, and <34 weeks’ gestation of 100, 80, 47, and 35%, respectively.Although our established variable of CL shortening by "25%between the two measurements have better sensitivity than theuse of the CL by Souka et al. [4] to predict PTB at <32 and 34 weeks, itwas not as effective as Souka et al.’s method at predictingspontaneous PTB at <28 and <30 weeks’ gestation. It is possiblethat the small number of patients who were delivered at <28 weeks(4 patients) and <30 weeks (5) acted as a limiting factor in our study.
In our study the high specificities and the high negativepredictive values of CL shortening by "25% for the prediction ofspontaneous PTB at <32 weeks’ gestation indicate that CLshortening was better at predicting the absence than the presenceof various degrees of spontaneous prematurity. Therefore, patientscan be informed and reassured that the risk of very PTB is quite low,potentially avoiding hospitalization, bed rest, and overtreatment.
Table 3Outcomes in all women with cervical length > 25 mm at the second examination in both groups.
Gestational age at CL shortening by "25% CL shortening by <25% P value
Delivery in weeks with cervical length > 25 mmN = 19
with cervical length > 25 mmN = 170
<28 weeks 2 (10.5%) 1 (0.6%) 0.0203"28 to <30 weeks 3 (15.8%) 2 (1.2%) 0.026"30 to <32 weeks 5 (26.3%) 6 (3.5%) <0.001"32 to <34 weeks 7 (36.8%) 17 (10.0%) 0.029"34 2 (10.5%) 144 (84.7%) <0.001
N, number; CL, cervical length.
Table 4Sensitivity and specificity for spontaneous delivery at <28, 30, 32, and 34 weeks gestation according to CL ! 25 mm, and the change in the cervical length by "25%.
<28 weeks "28 to <30 weeks "30 to <32 weeks "32 to <34 weeks
Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity
CL change by "25% 66.67 84.7 55.56 85 58.8 87 45.2 88.2CL ! 25 mm 50 91.6 44.4 92 53.3 92.7 22.6 92.7
CL, cervical length.
M.I. Khalil et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology xxx (2013) xxx–xxx 3
G Model
EURO-8017; No. of Pages 4
Please cite this article in press as: Khalil MI, et al. The use of cervical length and change in cervical length for prediction of spontaneouspreterm birth in asymptomatic twin pregnancies. Eur J Obstet Gynecol (2013), http://dx.doi.org/10.1016/j.ejogrb.2013.02.019
patients in group A delivered at significantly earlier gestationalages compared with the patients in group B (Table 2). Thedifference between the groups remained statistically significanteven after excluding data from patients who presented with a shortcervix (CL ! 25 mm) on the second ultrasound assessment of theCL (Tables 2 and 3).
Multiple logistic regression model was performed, controllingfor age, parity, gestational diabetes, confirmed urinary tractinfection, prior PTB, in vitro fertilization and chorionicity. Cervicalshortening of "25% was the only factor significantly associatedwith spontaneous PTB with a gestation time of <32 weeks (crudeOR (95% CI) 14.71 (6.25–36.18); P-value < 0.001, adjusted OR (95%CI) 20.26 (7.93–56.91); P-value < 0.001). This result is still trueafter excluding the women with a CL ! 25 mm on the secondultrasound assessment of the CL.
There was a >7-fold increase in the rate of spontaneous pretermbirth at <32 weeks, from 4 to 28.6% (OR, 9.54; 95% CI, 3.32–27.36)(Table 2). This result is still true after excluding the women with aCL ! 25 mm from 3.5 to 26.3% (OR, 9.76; CI, 2.64–36.04) (Table 3).
The use of CL shortening by "25% has better sensitivity than theuse of CL ! 25 mm for the prediction of PTB at <28, <30, <32, and<34 weeks of gestation, respectively, but the prediction specificityis higher for CL!25 mm for the same gestation periods (Table 4).The sensitivity, specificity, and positive and negative predictivevalue of CL shortening by "25%, were 58.8%, 87%, 28.57%, and95.97%, respectively, for the prediction of spontaneous PTB at <32weeks gestation. The rates of delivery at <32 weeks of gestationwere 28.6% (unadjusted OR, 6.33; 95% CI, 1.111–36.102, and 15.4%;unadjusted OR, 5.697; 95% CI, 1.028–31.559) when the cervixmeasured !2.5 cm at 24 and 28 weeks of gestation, respectively.
Based on ROC curve analysis, the use of CL shortening by "25%was superior, but not statistically significantly, to the use of CL forthe prediction of PTB at <32 (Fig. 1 graph C, P = 0.0524), and at <34weeks (Fig. 1 graph D, P = 0.281). CL, however, was preferred for theprediction of PTB at <28 (Fig. 1 graph A, P = 0.037) and <30 weeks(Fig. 1 graph B, P = 0.0457).
4. Comment
This study confirmed the association between the shortening ofCL by "25% over two measurements and PTB in asymptomatic twinpregnancies. This test was found to be a good predictor of PTB at <28,<30, <32, and <34 weeks’ gestation. This result remained true evenafter excluding women with a short cervix (CL ! 25 mm) on the
repeated CL. Our results are similar to and consistent with those ofFox et al. [7], who found that a CL that decreases by "20% over 2measurements is a significant predictor of spontaneous pretermbirth at <28, <30, <32, and <34 weeks. This effect remained trueeven when excluding patients who exhibited a CL ! 25 mm.
With the use of CL shortening by "20% in the Fox et al. study [7],the sensitivity was 75, 60, 54.5, and 35%, and the specificity was86.3, 86.2, 88.1, and 88.1% for the prediction of PTB < 28, <30, <32,and <34 weeks respectively. Our cutoff point of CL shortening by"25% is better for the prediction of PTB < 32 and <34 weeks thanthe "20% cutoff point used by Fox et al. [7], but the "20% cutoffpoint is better for the prediction of PTB < 28 and <30 weeks.
Our study differs from both Fox et al. [7], and other previousstudies [2–6] in that we evaluated both the CL and the percentchange in CL over time to predict PTB. There are several studies thatexamined the use of single or repeated cervical length measurementas a predictor of PTB in twin gestations. Although predictiveaccuracy varies between studies, shortened cervical length usuallyhas a low sensitivity but high positive predictive value for PTB [2–6].
Goldenberg et al. [3] studied 147 sets of twins and found thatthe rates of delivery at <32 weeks of gestation were 26.9% and13.2% when the cervix measured !2.5 cm at 24 and 28 weeks ofgestation, respectively [3]. We almost have similar results, but thenumber of patients with short CL ! 25 mm in our study were only20 cases in total, which is smaller than the number in theGoldenberg et al. [3] study with 26 cases at 24 weeks and 48 casesat 28 weeks.
Souka et al. [4] found that a cervical length of !25 mm at 23weeks had sensitivities for predicting spontaneous PTB at <28, <30,<32, and <34 weeks’ gestation of 100, 80, 47, and 35%, respectively.Although our established variable of CL shortening by "25%between the two measurements have better sensitivity than theuse of the CL by Souka et al. [4] to predict PTB at <32 and 34 weeks, itwas not as effective as Souka et al.’s method at predictingspontaneous PTB at <28 and <30 weeks’ gestation. It is possiblethat the small number of patients who were delivered at <28 weeks(4 patients) and <30 weeks (5) acted as a limiting factor in our study.
In our study the high specificities and the high negativepredictive values of CL shortening by "25% for the prediction ofspontaneous PTB at <32 weeks’ gestation indicate that CLshortening was better at predicting the absence than the presenceof various degrees of spontaneous prematurity. Therefore, patientscan be informed and reassured that the risk of very PTB is quite low,potentially avoiding hospitalization, bed rest, and overtreatment.
Table 3Outcomes in all women with cervical length > 25 mm at the second examination in both groups.
Gestational age at CL shortening by "25% CL shortening by <25% P value
Delivery in weeks with cervical length > 25 mmN = 19
with cervical length > 25 mmN = 170
<28 weeks 2 (10.5%) 1 (0.6%) 0.0203"28 to <30 weeks 3 (15.8%) 2 (1.2%) 0.026"30 to <32 weeks 5 (26.3%) 6 (3.5%) <0.001"32 to <34 weeks 7 (36.8%) 17 (10.0%) 0.029"34 2 (10.5%) 144 (84.7%) <0.001
N, number; CL, cervical length.
Table 4Sensitivity and specificity for spontaneous delivery at <28, 30, 32, and 34 weeks gestation according to CL ! 25 mm, and the change in the cervical length by "25%.
<28 weeks "28 to <30 weeks "30 to <32 weeks "32 to <34 weeks
Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity
CL change by "25% 66.67 84.7 55.56 85 58.8 87 45.2 88.2CL ! 25 mm 50 91.6 44.4 92 53.3 92.7 22.6 92.7
CL, cervical length.
M.I. Khalil et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology xxx (2013) xxx–xxx 3
G Model
EURO-8017; No. of Pages 4
Please cite this article in press as: Khalil MI, et al. The use of cervical length and change in cervical length for prediction of spontaneouspreterm birth in asymptomatic twin pregnancies. Eur J Obstet Gynecol (2013), http://dx.doi.org/10.1016/j.ejogrb.2013.02.019
patients in group A delivered at significantly earlier gestationalages compared with the patients in group B (Table 2). Thedifference between the groups remained statistically significanteven after excluding data from patients who presented with a shortcervix (CL ! 25 mm) on the second ultrasound assessment of theCL (Tables 2 and 3).
Multiple logistic regression model was performed, controllingfor age, parity, gestational diabetes, confirmed urinary tractinfection, prior PTB, in vitro fertilization and chorionicity. Cervicalshortening of "25% was the only factor significantly associatedwith spontaneous PTB with a gestation time of <32 weeks (crudeOR (95% CI) 14.71 (6.25–36.18); P-value < 0.001, adjusted OR (95%CI) 20.26 (7.93–56.91); P-value < 0.001). This result is still trueafter excluding the women with a CL ! 25 mm on the secondultrasound assessment of the CL.
There was a >7-fold increase in the rate of spontaneous pretermbirth at <32 weeks, from 4 to 28.6% (OR, 9.54; 95% CI, 3.32–27.36)(Table 2). This result is still true after excluding the women with aCL ! 25 mm from 3.5 to 26.3% (OR, 9.76; CI, 2.64–36.04) (Table 3).
The use of CL shortening by "25% has better sensitivity than theuse of CL ! 25 mm for the prediction of PTB at <28, <30, <32, and<34 weeks of gestation, respectively, but the prediction specificityis higher for CL!25 mm for the same gestation periods (Table 4).The sensitivity, specificity, and positive and negative predictivevalue of CL shortening by "25%, were 58.8%, 87%, 28.57%, and95.97%, respectively, for the prediction of spontaneous PTB at <32weeks gestation. The rates of delivery at <32 weeks of gestationwere 28.6% (unadjusted OR, 6.33; 95% CI, 1.111–36.102, and 15.4%;unadjusted OR, 5.697; 95% CI, 1.028–31.559) when the cervixmeasured !2.5 cm at 24 and 28 weeks of gestation, respectively.
Based on ROC curve analysis, the use of CL shortening by "25%was superior, but not statistically significantly, to the use of CL forthe prediction of PTB at <32 (Fig. 1 graph C, P = 0.0524), and at <34weeks (Fig. 1 graph D, P = 0.281). CL, however, was preferred for theprediction of PTB at <28 (Fig. 1 graph A, P = 0.037) and <30 weeks(Fig. 1 graph B, P = 0.0457).
4. Comment
This study confirmed the association between the shortening ofCL by "25% over two measurements and PTB in asymptomatic twinpregnancies. This test was found to be a good predictor of PTB at <28,<30, <32, and <34 weeks’ gestation. This result remained true evenafter excluding women with a short cervix (CL ! 25 mm) on the
repeated CL. Our results are similar to and consistent with those ofFox et al. [7], who found that a CL that decreases by "20% over 2measurements is a significant predictor of spontaneous pretermbirth at <28, <30, <32, and <34 weeks. This effect remained trueeven when excluding patients who exhibited a CL ! 25 mm.
With the use of CL shortening by "20% in the Fox et al. study [7],the sensitivity was 75, 60, 54.5, and 35%, and the specificity was86.3, 86.2, 88.1, and 88.1% for the prediction of PTB < 28, <30, <32,and <34 weeks respectively. Our cutoff point of CL shortening by"25% is better for the prediction of PTB < 32 and <34 weeks thanthe "20% cutoff point used by Fox et al. [7], but the "20% cutoffpoint is better for the prediction of PTB < 28 and <30 weeks.
Our study differs from both Fox et al. [7], and other previousstudies [2–6] in that we evaluated both the CL and the percentchange in CL over time to predict PTB. There are several studies thatexamined the use of single or repeated cervical length measurementas a predictor of PTB in twin gestations. Although predictiveaccuracy varies between studies, shortened cervical length usuallyhas a low sensitivity but high positive predictive value for PTB [2–6].
Goldenberg et al. [3] studied 147 sets of twins and found thatthe rates of delivery at <32 weeks of gestation were 26.9% and13.2% when the cervix measured !2.5 cm at 24 and 28 weeks ofgestation, respectively [3]. We almost have similar results, but thenumber of patients with short CL ! 25 mm in our study were only20 cases in total, which is smaller than the number in theGoldenberg et al. [3] study with 26 cases at 24 weeks and 48 casesat 28 weeks.
Souka et al. [4] found that a cervical length of !25 mm at 23weeks had sensitivities for predicting spontaneous PTB at <28, <30,<32, and <34 weeks’ gestation of 100, 80, 47, and 35%, respectively.Although our established variable of CL shortening by "25%between the two measurements have better sensitivity than theuse of the CL by Souka et al. [4] to predict PTB at <32 and 34 weeks, itwas not as effective as Souka et al.’s method at predictingspontaneous PTB at <28 and <30 weeks’ gestation. It is possiblethat the small number of patients who were delivered at <28 weeks(4 patients) and <30 weeks (5) acted as a limiting factor in our study.
In our study the high specificities and the high negativepredictive values of CL shortening by "25% for the prediction ofspontaneous PTB at <32 weeks’ gestation indicate that CLshortening was better at predicting the absence than the presenceof various degrees of spontaneous prematurity. Therefore, patientscan be informed and reassured that the risk of very PTB is quite low,potentially avoiding hospitalization, bed rest, and overtreatment.
Table 3Outcomes in all women with cervical length > 25 mm at the second examination in both groups.
Gestational age at CL shortening by "25% CL shortening by <25% P value
Delivery in weeks with cervical length > 25 mmN = 19
with cervical length > 25 mmN = 170
<28 weeks 2 (10.5%) 1 (0.6%) 0.0203"28 to <30 weeks 3 (15.8%) 2 (1.2%) 0.026"30 to <32 weeks 5 (26.3%) 6 (3.5%) <0.001"32 to <34 weeks 7 (36.8%) 17 (10.0%) 0.029"34 2 (10.5%) 144 (84.7%) <0.001
N, number; CL, cervical length.
Table 4Sensitivity and specificity for spontaneous delivery at <28, 30, 32, and 34 weeks gestation according to CL ! 25 mm, and the change in the cervical length by "25%.
<28 weeks "28 to <30 weeks "30 to <32 weeks "32 to <34 weeks
Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity
CL change by "25% 66.67 84.7 55.56 85 58.8 87 45.2 88.2CL ! 25 mm 50 91.6 44.4 92 53.3 92.7 22.6 92.7
CL, cervical length.
M.I. Khalil et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology xxx (2013) xxx–xxx 3
G Model
EURO-8017; No. of Pages 4
Please cite this article in press as: Khalil MI, et al. The use of cervical length and change in cervical length for prediction of spontaneouspreterm birth in asymptomatic twin pregnancies. Eur J Obstet Gynecol (2013), http://dx.doi.org/10.1016/j.ejogrb.2013.02.019Khalil MI, et al. The use of cervical length and change in cervical length for prediction of spontaneous preterm birth in asymptomatic twin pregnancies. Eur J Obstet Gynecol (2013)

+Fibronectina Fetal
n Similar utilidad que en embarazo único n 28 sem à OR 9.4 [1- 67,6] n 30 sem à OR 46,1 [4,2- 1381]
n Seria útil en mujeres con SPP dado su alto VPN n VPN 97% para PP < 14 días
Singer E, Pilpel S, Bsat F, et al: Accuracy of fetal fibronectin to predict preterm birth in twin gestations with symptoms of labor. Obstet Gyne- col 109:1083-1087, 2007
Goldenberg RL, Iams JD, Miodovnik M, et al: The preterm prediction study: Risk factors in twin gestations. National Institute of Child Health and Human Development maternal-Fetal medicine units network. Am J Obstet Gynecol 175:1047-1053, 1996

+Prevención PP en gemelar

+Reposo en cama Hospitalizado

+Reposo en cama Hospitalizado
n 713 mujeres (7 estudios) n Hospitalización profiláctica 30 sem v/s
Selectiva n Sin diferencia en: n Parto prematuro n Mortalidad perinatal n Tasa Cesárea
n Reducción marginal RN < 2500 g. (RR 0.92 [0,85-1])
n Costos, Estrés materno (6 v/s 18%) y Familiar
Hospitalisation and bed rest for multiple pregnancy (Review)
Crowther CA, Han S
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2010, Issue 7
http://www.thecochranelibrary.com
Hospitalisation and bed rest for multiple pregnancy (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Crowther CA, Han S. Hospitalisation and bed rest for multiple pregnancy. Cochrane Database Syst Rev 2010;(7): CD000110.
Hospitaliza profiláctica NO
En pacientes de alto riesgo (cervicometria
muy alterada) reposo si..
Hospitalizada??

+Progesterona

+Progesterona pp
Fonseca et al. Progesterone and the risk of preterm birth among women with a short cervix. NEnglJ
Med 2007;357:462–9.
Combs C et al. 17-OH-progesterone caproate for twin pregnancy. Am
J Obstet Gynecol 2011;204:221–8.
Cetingoz E et al. Progesterone effects on preterm birth in
high-risk pregnancies. Arch Gynecol Obstet
2011;283:423–9.
Rouse DJ et al. A trial of 17 alpha-
hydroxyprogesterone caproate to prevent
prematurity in twins. N Engl J Med
2007;357:454–61.
Rode L et al. Prevention of preterm delivery in
twin gestations (PREDICT). Ultrasound
Obstet Gynecol 2011;38: 272–80.
Lim AC et al. 17alpha-OH progesterone caproate for the
prevention of adverse neonatal outcome in
multiple pregnancies.Obstet
Gynecol 2011;118:513–20.
Briery et al. Progesterone does not prevent preterm births in women with twins.
SouthMedJ 2009;102:900–4.
Aboulghar et al. The use of vaginal natural
progesterone for prevention of preterm
birth in IVF/ICSI pregnancies. Reprod
Biomed Online 2012;25:133–8.
Serra V et al. Increased doses of vaginal
progesterone for the prevention of preterm
birth in twin pregnancies. BJOG
2013;120:50–7.
Norman JE et al. Progesterone for the prevention of preterm birth in twin pregnancy (STOPPIT). Lancet
2009;373:2034–40.
Wood S et al. Vaginal progesterone to
prevent preterm birth in multiple pregnancy.
J Perinat Med 2012
Brizot. Vaginal progesterone in twin
pregnancies. Am J Obstet Gynecol 2015.
Con LC
Sin LC

+Progesterona
n 12 Estudios Ramdomizados n 8 Embarazo gemelar no seleccionado n 4 consideran Longitud cervical
n Ninguno ha podido demostrar reducción parto prematuro.

+Progesterona
n De los Tres estudios que consideran LC considerados en meta-análisis Romero et al
• 24 Gemelares <15 mm. OR 0,49 [0,09- 2,53]
Fonseca et al. 2007
• 72 Gemelares Alto Riesgo • 47 LC < 30 mm
• Sin diferencia estadística en prevención PP
Rode, Klein, et al. 2011
• 52 mujeres LC < P25: 36 mm (24%) • 55,8% pp < 35 sem v/s 36,9% p.0.02
• Sin diferencia estadística en prevención PP
Rouse, Durnwald et al. 2010
200 mg Prog micronizada
250 mg of 17OH Pg cap
200 mg Prog micronizada

+ Progesterona. (2) Revisión sistemática y Metaanalisis
n 5 Estudios Controlados Ramdomizados mujeres LC < 25 mm que recibieron progesterona vaginal v/s placebo o no tto. n 775 Mujeres
n 52 Gemelares (6,7%)
n Sin reducción significativa de parto prematuro < 37, 35, 28 sem.
n Reducción morbilidad neonatal compuesta n OR 0,52 [0,29- 0,93]
singleton gestation and at least 1 previousspontaneous preterm birth !37 weeks ofgestation (RR, 0.41; 95% CI, 0.17–0.98), andin women with a twin gestation and no pre-vious preterm birth (RR, 0.52; 95% CI,0.29–0.93).
Subgroup and sensitivity analysesSubgroup analyses of the effect of vaginalprogesterone on primary outcomes arepresented in Table 5. There was no evi-dence that women in any one of the pre-specified subgroups benefit more or lessfrom the use of vaginal progesteronethan those in any other subgroup (all Pfor interaction " .30). However, the useof vaginal progesterone was associatedwith a statistically significant reductionin the risk of preterm birth !33 weeksand composite neonatal morbidity and
mortality in both women with no previ-ous spontaneous preterm birth andwomen with at least 1 previous sponta-neous preterm birth !37 weeks of gesta-tion, women with a sonographic cervicallength between 10-20 mm, women aged20-34 years, and Caucasian women.
No significant differences were notedfor preterm birth !33 weeks of gestationand composite neonatal morbidity andmortality between subgroups based onthe daily dose of progesterone. A signifi-cant decrease in the risk of preterm birth!33 weeks of gestation and compositeneonatal morbidity and mortality wasfound in women who received either 90-100 or 200 mg/d of vaginal progesterone.
The effect of vaginal progesterone onthe risk of preterm birth !33 weeks of
gestation and composite neonatal mor-bidity/mortality did not change whensensitivity analysis was limited to the 2trials131,133 in which the primary aim wasto evaluate the effect of vaginal proges-terone in women with a short cervix(pooled RR, 0.57; 95% CI, 0.40 – 0.80 forpreterm birth !33 weeks and pooled RR,0.54; 95% CI, 0.35– 0.82 for compositeneonatal morbidity/mortality). In addi-tion, the results of the metaanalyses didnot change significantly when randomeffects models were used for pretermbirth !33 weeks (RR, 0.59; 95% CI,0.43– 0.81) or for composite neonatalmorbidity/mortality (RR, 0.59; 95% CI,0.41– 0.83). Sensitivity analyses based ontrial quality were not performed becauseall trials were considered at low risk for
TABLE 3Effect of vaginal progesterone on preterm birth and perinatal outcomes in singleton and twin gestations
Outcome
Singleton pregnancy Twin pregnancy
InteractionP value
No. oftrials
No. of events/total No.
Pooled RR(95% CI)
No. oftrials
No. of events/total No.
Pooled RR(95% CI)
Vaginalprogesterone Placebo
Vaginalprogesterone Placebo
Primary outcome.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !33 wk 4 41/365 72/358 0.56 (0.40–0.80) 3 7/23 13/29 0.70 (0.34–1.44) .55................................................................................................................................................................................................................................................................................................................................................................................
Secondary outcomes.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !37 wk 4 127/365 141/358 0.91 (0.75–1.10) 3 17/23 24/29 0.91 (0.68–1.23) .88.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !35 wk 4 67/365 100/358 0.67 (0.51–0.87) 3 12/23 18/29 0.91 (0.57–1.46) .24.......................................................................................................................................................................................................................................................................................................................................................................
Preterm birth !28 wk 4 20/365 39/358 0.51 (0.31–0.85) 3 1/23 4/29 0.44 (0.11–1.85) .83.......................................................................................................................................................................................................................................................................................................................................................................
Respiratory distress syndrome 4 17/365 37/358 0.47 (0.27–0.81) 3 8/46 15/58 0.48 (0.21–1.09) .68.......................................................................................................................................................................................................................................................................................................................................................................
Necrotizing enterocolitis 4 5/365 6/358 0.88 (0.29–2.62) 3 0/46 0/58 Not estimable NA.......................................................................................................................................................................................................................................................................................................................................................................
Intraventricular hemorrhage 4 5/365 7/358 0.68 (0.22–2.13) 3 1/46 2/58 1.00 (0.10–10.11) .74.......................................................................................................................................................................................................................................................................................................................................................................
Proven neonatal sepsis 4 11/365 14/358 0.80 (0.37–1.74) 3 1/46 6/58 0.33 (0.06–1.67) .30.......................................................................................................................................................................................................................................................................................................................................................................
Retinopathy of prematurity 4 5/365 3/358 1.51 (0.40–5.69) 3 1/46 0/58 1.42 (0.05–42.22) .91.......................................................................................................................................................................................................................................................................................................................................................................
Fetal death 4 6/365 7/358 0.82 (0.28–2.40) 3 0/46 0/58 Not estimable NA.......................................................................................................................................................................................................................................................................................................................................................................
Neonatal death 4 6/365 11/358 0.53 (0.20–1.39) 3 2/46 4/58 0.68 (0.23–2.02) .69.......................................................................................................................................................................................................................................................................................................................................................................
Perinatal death 4 12/365 18/358 0.64 (0.31–1.31) 3 2/46 4/58 0.68 (0.23–2.02) .90.......................................................................................................................................................................................................................................................................................................................................................................
Composite neonatal morbidity/mortalitya
4 29/365 49/358 0.59 (0.38–0.91) 3 11/46 23/58 0.52(0.29–0.93) .69
.......................................................................................................................................................................................................................................................................................................................................................................
Apgar score !7 at 5 min 4 11/362 23/354 0.48 (0.24–0.95) 3 4/46 4/58 1.03 (0.38–2.81) .20.......................................................................................................................................................................................................................................................................................................................................................................
Birthweight !1500 g 4 28/364 53/355 0.52 (0.34–0.81) 3 8/46 15/58 0.69 (0.34–1.39) .47.......................................................................................................................................................................................................................................................................................................................................................................
Birthweight !2500 g 4 102/364 117/355 0.86 (0.69–1.07) 3 38/46 45/58 1.11 (0.92–1.35) .11.......................................................................................................................................................................................................................................................................................................................................................................
Admission to NICU 4 59/365 87/358 0.67 (0.50–0.91) 3 26/46 34/58 0.98 (0.70–1.35) .12.......................................................................................................................................................................................................................................................................................................................................................................
Mechanical ventilation 4 28/365 43/358 0.65 (0.41–1.01) 3 7/46 8/58 0.68 (0.30–1.56) .88................................................................................................................................................................................................................................................................................................................................................................................CI, confidence interval; NA, not applicable; NICU, neonatal intensive care unit; RR, relative risk.a Occurrence of any of the following events: respiratory distress syndrome, intraventricular hemorrhage, necrotizing enterocolitis, proven neonatal sepsis, or neonatal death.
Romero. Vaginal progesterone to prevent preterm birth in women with a short cervix: an IPD metaanalysis. Am J Obstet Gynecol 2012.
www.AJOG.org Reports of Major Impact
FEBRUARY 2012 American Journal of Obstetrics & Gynecology 124.e10

+ Progesterona. (2) Revisión sistemática y Metaanalisis
n 13 Estudios Controlados progesterona vaginal o 17-OHCP v/s placebo. n 3768 Gemelares
n 116 Gemelares LC < 25 mm pg vaginal
n Sin reducción significativa de parto prematuro < 37, 35, 28 sem.
n Reducción morbilidad neonatal compuesta n RR 0.57 [0,47- 0,7]
Schuit et al. BMC Pregnancy and Childbirth 2012, 12:13

+Arch Gynecol Obstet (2016) 293:61–67
n ECR, Egipto.
n 250 embarazos gemelares bicoriales asintomatico con LC 20-25 mm a las 20-24 sem EG
n Ramdomización n 125: Progesterona vaginal 400 mg/dia iniciado 20-24 sem
n 125: no tratamiento
n Sin diferencias demográficas, ni ant. PP.
n Outcome primario: PP <34 sem
n Outcome secundario: SDR y Mortalidad neonatal precoz.

+Arch Gynecol Obstet (2016) 293:61–67

Conclusión…
Progesterona en Gemelar con cuello
corto reduciría riesgo de PP.
Faltan estudio que confirmen hallazgos


+
Vedel et al. Ultrasound Obstet Gynecol. 2016 Apr 22.
Long-term effects of prenatal progesterone exposure: Neurophysiological development and hospital admissions in twins up to 8 years of age.
n Seguimiento 8 años niños PREDICT
n 492 niños expuestos a progesterona y 497 a placebo.
n Sin diferencia en numero hospitalizaciones
n Se observo un mayor numero de dg relacionado con patologia cardiaca en grupo Pg, NO Significativo OR 1,66 IC [0,8.3,37]
n Promedio de Score de test neurodesarrollo fueron levemente más alto en grupo expuesto (p 0,03)
n El riesgo de presentar un score <p10 disminuyó en grupo Pg (OR 0,34 [0,14.0,86]

+Cerclage Cervical

+Cerclage
n Tipos de Cerclaje
n Electivo/ Por Historia (primario) n Historia clásica Insuficiencia cervical (>3
perdidas fetales) n Terapéutico/ Por US (secundario) n Pacientes con antecedente PP espontáneo
<34sem + cuello acortado < 15mm à Cerclaje idealmente antes de 23 sem.
n Emergencia/ Por examen físico (Terciario)

+Cerclage Terapéutico
statistics from published data. Other advantages ofusing individual patient-level data include the abilityto perform survival analysis, a more effective oppor-tunity for subgroup analysis and possible hypothesisgeneration, and the ability to adjust for possibleconfounders and look for interactions among vari-ables.21–25 Meta-analysis using individual patient datahas been shown to be the least biased and mostreliable means of addressing questions unresolved byindividual clinical trials.25
The benefit of cerclage in high-risk singletonpopulations and the detriment in multiple gestationsfound in our meta-analysis are in general agreementwith individual trial results and with nonrandomizeddata. The only trial that showed benefit from cerclageincluded just singleton gestations with the highestincidence of prior preterm birth (Table 1).5 Given theresults of our meta-analysis, it is not surprising that atrial focusing mostly on this population would showpositive results. Three other randomized trials on
Table 2. Selected Outcomes
Population Outcome Cerclage (%)No Cerclage
(%) RR (95% CI)
Total PTB ! 37 wk 133/305 (43.6) 157/302 (52.0) 0.84 (0.71–0.99)PTB ! 35 wk 89/305 (29.2) 105/302 (34.8) 0.84 (0.67–1.06)PTB ! 34 wk 80/305 (26.2) 90/302 (29.8) 0.88 (0.68–1.14)PTB ! 32 wk 65/305 (21.3) 74/302 (24.5) 0.87 (0.65–1.16)PTB ! 28 wk 44/305 (14.4) 43/302 (14.2) 1.02 (0.69–1.49)PTB ! 24 wk 14/305 (4.6) 12/302 (4.0) 1.15 (0.53–2.49)GA at delivery 35.1 " 5.3 34.8 " 5.6 P #.51PPROM 48/305 (15.7) 50/302 (16.6) 0.95 (0.66–1.35)Perin mort 36/335 (10.7) 27/333 (8.1) 1.31 (0.82–2.10)
SingletonsAll PTB ! 35 wk 69/278 (24.8) 93/274 (33.9) 0.74 (0.57–0.96)
Perin mort 22/278 (7.9) 23/274 (8.4) 0.94 (0.54–1.64)No risks for PTB PTB ! 35 wk 31/121 (25.6) 38/114 (33.3) 0.76 (0.52–1.15)
Perin mort 10/121 (8.3) 8/114 (7.0) 1.18 (0.48–2.88)No prior PTB PTB ! 35 wk 44/171 (20.6) 54/173 (31.2) 0.84 (0.60–1.17)
Perin mort 13/171 (7.6) 14/173 (8.1) 0.94 (0.46–1.90)Prior PTB ! 37 wk PTB ! 37 wk 41/107 (38.3) 61/101 (60.4) 0.63 (0.48–0.85)
PTB ! 35 wk 25/107 (23.4) 39/101 (38.6) 0.61 (0.40–0.92)PTB ! 34 wk 23/107 (21.5) 32/101 (31.7) 0.68 (0.43–1.08)PTB ! 32 wk 17/107 (15.9) 28/101 (27.7) 0.58 (0.34–0.98)PTB ! 28 wk 12/107 (11.2) 17/101 (16.8) 0.66 (0.34–1.29)PTB ! 24 wk 4/107 (3.7) 7/101 (6.9) 0.54 (0.18–1.67)Perin mort 9/107 (8.4) 14/101 (13.8) 0.62 (0.29–1.30)
Prior STL 16—23 wk PTB ! 35 wk 15/68 (22.1) 20/51 (39.2) 0.57 (0.33–0.99)Perin mort 4/68 (5.9) 5/51 (9.8) 0.62 (0.19–2.06)
Cone biopsy PTB ! 35 wk 10/28 (35.7) 11/36 (30.6) 1.18 (0.57–2.45)Perin mort 3/28 (10.7) 2/36 (5.6) 1.46 (0.34–6.32)
$ 1 D&E PTB ! 35 wk 19/66 (28.8) 23/65 (35.4) 0.91 (0.57–1.47)Perin mort 5/66 (7.6) 9/65 (13.8) 0.61 (0.23–1.62)
GAshortCL ! 20 wk PTB ! 35 wk 16/54 (29.6) 21/52 (40.4) 0.68 (0.41–1.15)Perin mort 6/54 (11.1) 10/52 (19.2) 0.61 (0.23–1.60)
GAshortCL ! 20 wk PTB ! 35 wk 53/224 (23.7) 70/222 (31.5) 0.75 (0.55–1.02)Perin mort 16/224 (7.1) 16/222 (7.2) 0.95 (0.50–1.81)
CL ! 25 mm PTB ! 35 wk 69/274 (25.2) 93/273 (34.1) 0.75 (0.58–0.97)Perin mortal 22/274 (8.0) 21/273 (7.7) 0.96 (0.55–1.67)
CL " 15 mm PTB ! 35 wk 54/182 (29.7) 71/183 (38.8) 0.77 (0.58–1.02)Perin mortal 18/182 (9.9) 17/183 (9.3) 1.07 (0.59–1.97)
FUN/CL ! 25 mm PTB ! 35 wk 69/250 (27.6) 92/254 (36.2) 0.77 (0.60–1.00)Perin mortal 22/250 (8.8) 23/254 (9.1) 0.99 (0.57–1.72)
Twins PTB ! 35 wk 18/24 (75.0) 9/25 (36.0) 2.15 (1.15–4.01)Perin mort 11/48 (22.9) 3/50 (6.0) 2.66 (0.83–8.54)
RR, relative risk; CI, confidence interval; PTB, preterm birth; GA, gestational age; PPROM, preterm prematurerupture of membranes; Perin mortal, perinatal mortality; STL, second-trimester loss; D&E, dilatation andevacuation; GAshortCL ! 20 wk, gestational age at short cervical length less than 20 weeks; GAshortCL ! 20wk, gestational age at short cervical length 20 weeks or more; CL, cervical length; FUN/CL ! 25 mm,funneling ! 5 mm and cervical length ! 25 mm.
Data are expressed as n/n (%) or mean " standard deviation.
186 Berghella et al Cerclage for Short Cervix: A Meta-Analysis OBSTETRICS & GYNECOLOGY
statistics from published data. Other advantages ofusing individual patient-level data include the abilityto perform survival analysis, a more effective oppor-tunity for subgroup analysis and possible hypothesisgeneration, and the ability to adjust for possibleconfounders and look for interactions among vari-ables.21–25 Meta-analysis using individual patient datahas been shown to be the least biased and mostreliable means of addressing questions unresolved byindividual clinical trials.25
The benefit of cerclage in high-risk singletonpopulations and the detriment in multiple gestationsfound in our meta-analysis are in general agreementwith individual trial results and with nonrandomizeddata. The only trial that showed benefit from cerclageincluded just singleton gestations with the highestincidence of prior preterm birth (Table 1).5 Given theresults of our meta-analysis, it is not surprising that atrial focusing mostly on this population would showpositive results. Three other randomized trials on
Table 2. Selected Outcomes
Population Outcome Cerclage (%)No Cerclage
(%) RR (95% CI)
Total PTB ! 37 wk 133/305 (43.6) 157/302 (52.0) 0.84 (0.71–0.99)PTB ! 35 wk 89/305 (29.2) 105/302 (34.8) 0.84 (0.67–1.06)PTB ! 34 wk 80/305 (26.2) 90/302 (29.8) 0.88 (0.68–1.14)PTB ! 32 wk 65/305 (21.3) 74/302 (24.5) 0.87 (0.65–1.16)PTB ! 28 wk 44/305 (14.4) 43/302 (14.2) 1.02 (0.69–1.49)PTB ! 24 wk 14/305 (4.6) 12/302 (4.0) 1.15 (0.53–2.49)GA at delivery 35.1 " 5.3 34.8 " 5.6 P #.51PPROM 48/305 (15.7) 50/302 (16.6) 0.95 (0.66–1.35)Perin mort 36/335 (10.7) 27/333 (8.1) 1.31 (0.82–2.10)
SingletonsAll PTB ! 35 wk 69/278 (24.8) 93/274 (33.9) 0.74 (0.57–0.96)
Perin mort 22/278 (7.9) 23/274 (8.4) 0.94 (0.54–1.64)No risks for PTB PTB ! 35 wk 31/121 (25.6) 38/114 (33.3) 0.76 (0.52–1.15)
Perin mort 10/121 (8.3) 8/114 (7.0) 1.18 (0.48–2.88)No prior PTB PTB ! 35 wk 44/171 (20.6) 54/173 (31.2) 0.84 (0.60–1.17)
Perin mort 13/171 (7.6) 14/173 (8.1) 0.94 (0.46–1.90)Prior PTB ! 37 wk PTB ! 37 wk 41/107 (38.3) 61/101 (60.4) 0.63 (0.48–0.85)
PTB ! 35 wk 25/107 (23.4) 39/101 (38.6) 0.61 (0.40–0.92)PTB ! 34 wk 23/107 (21.5) 32/101 (31.7) 0.68 (0.43–1.08)PTB ! 32 wk 17/107 (15.9) 28/101 (27.7) 0.58 (0.34–0.98)PTB ! 28 wk 12/107 (11.2) 17/101 (16.8) 0.66 (0.34–1.29)PTB ! 24 wk 4/107 (3.7) 7/101 (6.9) 0.54 (0.18–1.67)Perin mort 9/107 (8.4) 14/101 (13.8) 0.62 (0.29–1.30)
Prior STL 16—23 wk PTB ! 35 wk 15/68 (22.1) 20/51 (39.2) 0.57 (0.33–0.99)Perin mort 4/68 (5.9) 5/51 (9.8) 0.62 (0.19–2.06)
Cone biopsy PTB ! 35 wk 10/28 (35.7) 11/36 (30.6) 1.18 (0.57–2.45)Perin mort 3/28 (10.7) 2/36 (5.6) 1.46 (0.34–6.32)
$ 1 D&E PTB ! 35 wk 19/66 (28.8) 23/65 (35.4) 0.91 (0.57–1.47)Perin mort 5/66 (7.6) 9/65 (13.8) 0.61 (0.23–1.62)
GAshortCL ! 20 wk PTB ! 35 wk 16/54 (29.6) 21/52 (40.4) 0.68 (0.41–1.15)Perin mort 6/54 (11.1) 10/52 (19.2) 0.61 (0.23–1.60)
GAshortCL ! 20 wk PTB ! 35 wk 53/224 (23.7) 70/222 (31.5) 0.75 (0.55–1.02)Perin mort 16/224 (7.1) 16/222 (7.2) 0.95 (0.50–1.81)
CL ! 25 mm PTB ! 35 wk 69/274 (25.2) 93/273 (34.1) 0.75 (0.58–0.97)Perin mortal 22/274 (8.0) 21/273 (7.7) 0.96 (0.55–1.67)
CL " 15 mm PTB ! 35 wk 54/182 (29.7) 71/183 (38.8) 0.77 (0.58–1.02)Perin mortal 18/182 (9.9) 17/183 (9.3) 1.07 (0.59–1.97)
FUN/CL ! 25 mm PTB ! 35 wk 69/250 (27.6) 92/254 (36.2) 0.77 (0.60–1.00)Perin mortal 22/250 (8.8) 23/254 (9.1) 0.99 (0.57–1.72)
Twins PTB ! 35 wk 18/24 (75.0) 9/25 (36.0) 2.15 (1.15–4.01)Perin mort 11/48 (22.9) 3/50 (6.0) 2.66 (0.83–8.54)
RR, relative risk; CI, confidence interval; PTB, preterm birth; GA, gestational age; PPROM, preterm prematurerupture of membranes; Perin mortal, perinatal mortality; STL, second-trimester loss; D&E, dilatation andevacuation; GAshortCL ! 20 wk, gestational age at short cervical length less than 20 weeks; GAshortCL ! 20wk, gestational age at short cervical length 20 weeks or more; CL, cervical length; FUN/CL ! 25 mm,funneling ! 5 mm and cervical length ! 25 mm.
Data are expressed as n/n (%) or mean " standard deviation.
186 Berghella et al Cerclage for Short Cervix: A Meta-Analysis OBSTETRICS & GYNECOLOGY
Berghella V, Odibo AO, To MS, et al: Cerclage for short cervix on ultrasonography: Meta-analysis of trials using individual patient-level data. Obstet Gynecol 106:181-189, 2005
• Revisión Sistemática • 4 Estudios • 607 mujeres LC < 25mm Asintomática • 49 Gemelares (8%) • 24 cerclage • 25 no cerclage • 98 RN

Nordic Federation of Societies of Obstetrics and Gynecology, Acta Obstetricia et Gynecologica Scandinavica 94 (2015) 352–358

Nordic Federation of Societies of Obstetrics and Gynecology, Acta Obstetricia et Gynecologica Scandinavica 94 (2015) 352–358

Nordic Federation of Societies of Obstetrics and Gynecology, Acta Obstetricia et Gynecologica Scandinavica 94 (2015) 352–358
Conclusión Revisión Sistemática Uso cerclaje
cervical en embarazo gemelar con LC >25 mm
asintomático: No Efecto

+Cerclage Terapéutico
Problema:
n Incluyen un bajo numero de paciente (n=49) y son solo 3 ECR
n Estudios clínicos no fueron diseñados para evaluar reducción de parto prematuro en embarazo múltiple
n Los Ensayos incluidos no estratificaban sus secuencias de asignación al azar para gemelos. n Los dos grupos diferían en incidencia de parto prematuro
previo y edad gestacional al momento de la aleatorización.

+
n Cohorte retrospectiva emb. Gemelar bicoriales o mono-bi con LC ≤ 25 mm en eco 16-24 sem.
n 1995 a 2012. 4 centros
n Outcome primario: PP <34 sem
n Outcome secundario: PP< 28, < 32 Y < 37 SEM n Planeado subgrupo con LC ≤ 15 mm.
n 140 MUJERES n 57 cerclage
n 83 no cerclage



+
Ultrasound Obstet Gynecol. 2016 Mar 16.
Cer vical cerclage for preterm birth prevention in twin gestations with short cervix: a retrospective cohort study. Houlihan C, Poon LC, Ciarlo M, Kim E, Guzman ER, Nicolaides KH.
n Londres y EEUU
n Cohorte retrospectiva emb. Gemelar dicorionico n 40 gemelares con cerclage por LC 1-24 mm entre 16-24
sem EG
n Casos fueron emparajedos con 40 controles sin cerclage, según LC y EG
n Outcome primario: PP <32 sem

Houlihan et al.Ultrasound Obstet Gynecol. 2016 Mar 16.

Houlihan et al.Ultrasound Obstet Gynecol. 2016 Mar 16.

+Cerclage Terapéutico (indicado por ultrasonografía)
n El cerclage en mujeres con embarazo gemelar y cuello corto (< 25 mm) podría reduce el parto prematuro, y aumentar el
tiempo de latencia al parto.
n Importante elección adecuada de pacientes.

+ Cerclaje de Emergencia
n Reportes de casos retrospectivos
Autor N EG AMCT
Atb (%)
Tocolisis
Latencia parto
PP <28s (%)
Pp <32 (%)
PP <34 (%)
RPM (%)
Sobre-vida neo
Levin 201229
14 20.1 ± 2,5
No 100 No 71.1 dias ±44.6
14 NA NA 14 16/20 (80%)
Rebarber 201330
12 14- 23+6
100 100 100 92 dias (26-145)
16 25 58 16 20/24 (83%)
Zanardini 201331
14 16-26 No 100 100 9.9 sem (0.3-17.9) sem
21 50 50 29 24/28 (86%)
Miller 201432
104
16- 23+6
No 54 57 69 dias (21-99)
34 52 NA 33,7 NE
Barnabeu 201533
7 19.6 ± 4
100 100 100 12,1 sem (4-16)
28 NE 43 14 14/14 (100%)
- Todos EG <24 sem - 50% con AMCT previa
- 100% uso ATB profilactico - Mayoria uso Indometacina
- Promedio latencia parto 69-92 dà 8 sem - Sobrevida promedio >80%.

+ Cerclaje de Emergencia
n Primer estudio cohorte retrospectivo n EEUU, Italia, Israel.
n Cerclaje emergencia vs manejo expectante
n 76 gemelares bicoriales, 16-24 sem EG. (38)
n Dilatación cervical ≥1 y ≤3 cm o membranas expuestas.
n 80% AMCT previa (negativa)
Roman et al. Cerclage in women with twin gestation and dilated cervix. Am J Obstet Gynecol 2016.

+Cerclaje de Emergencia
Variable Cerclage N=38
Control N=38
aOR (IC 95%) Valor P PP <34 sem 20 (53,6%) 36 (94,7%) 0,06 (0,03-0,34) <.0001 PP <32 sem 17 (44,7%) 34 (89,4%) 0,08 (0,03.0,34) <.0001 PP <28 sem 12 (31.6%) 34 (89,4%) 0,05
(0,01-0,21) <.0001
PP<24 sem 5 (13,1%) 18 (47,3%) 0,17 (0,05-0,54)
.02 RPM <34 sem 8 (21%) 12 (31,5%) 0,5 (0,3.1,6) .58 Latencia dg al parto (sem)
10.4 ± 5,6 3,7 ± 3,2 6,76 (4,71- 8,81)
<.0001 Mortalidad perinatal
21/76 (27,6%) 45/76 (59%) 0,24 (0,11-0,5)
<.0001 Outcome neonatal compuesto
18/54 (33.9%) 38/42 (90,5%) 0,05 (0,01-0,21)
<.0001
Roman et al. Cerclage in women with twin gestation and dilated cervix. Am J Obstet Gynecol 2016.

+Cerclage de Rescate (Dilatación cervical- exposición memb)
n El cerclage de rescate en mujeres con embarazo gemelar y dilatación cervical
con o sin membranas expuestas, podría ser útil.

+Pesario Cervical

+Pesario Cervical
Pro-‐Twin. 2013 Liem et al
PECET-‐Twin. 2016 Goya et al.
Nicolaides et al. 2016

+Variable Pro-‐Twin. 2013
Liem et al PECET-‐Twin. 2016 Goya et al.
Nicolaides et al. 2016 Población Embarazo mul+ple Embarazo mul+ple con
LC ≤ 25 mm. Embarazo múl+ple
Número (P/C) 813 (401-‐407) 137 (68/66) 1177 (588/589) LC ≤ 25 mm 9 (1%) 137 (100%) (68/66) 215 (18%) (106/108) LC <p25 133 (16%) [LC=38 mm] NA NA Pérdida 0,7% 2.1% 0,3%
EG promedio ramdomización
17 s 22 s 22 s LC promedio 43 mm 19 mm 32 mm
PP<34 s (P/C) 10% / 12% RR 0.86 [0.65 -‐1.15]
NA 13.6%/ 12.9% RR 1.04 [0.78-‐1.41]
PP < 34 s en CC (P/C)
<32s: 29% /14% RR 0.49 [0.24-‐0-‐97]
16.2% / 39.4% RR 0.44 [0.22-‐0.76]
31.1%/ 25.9% RR 1.2 [0.78-‐1.84]
Morbilidad neonatal en CC
29%/ 12% RR 0,4 [0.19-‐0.83]
5.9%/ 9.1% RR 0.54 [0.27-‐1,50]
23.2%/ 19,5% RR1.18 [0.69-‐2.01]
Aumento Flujo vaginal
26%/ 0% 100/ 53% p.0001 42.1 / 20.4% p<.0001

+ Comparación
ProTwin Nicolaides
Estudio Ramdomizado Abierto multicentrico (paises bajos)
Idem Multicentrico
Reclutamiento
Sept 2009- marzo 2012 Ag 2008- Mayo 2011
N 813 1180
Perdida 0.7% 0.3%
EG ramdomi 16.9 sem 22 sem
EG insercion 18 sem 22 sem
EG LC 18. 5 22 sem
LC prom 43-44
LC <25 1% (n.9) 18% (215)
LC< P25 (38mm) 78/55 (16%)
PP <32s (C/P) 10/12% P25:10/8 LC<25: 21/25.4%

+Conclusiones
n Existe poca evidencia para uso cualquier método en prevención PP Embarazo Gemelar.
n Progesterona vaginal en embarazo gemelar con LC< 25 mm asintomático, podría mejorar outcome neonatal sin disminuir incidencia PP. Faltan estudios con mayor N.
n Cerclage en embarazo gemelar con LC< 25 mm asintomático podría ser útil en prolongar el periodo de latencia al parto.
n Cerclage de emergencia en embarazo gemelar permitiría prolongar la gestación hasta la viabilidad.
n Pesario resultados controvertidos: n Podría disminuir riesgo PP < 32 sem en casi 50% en mujeres con LC < p
25. Solo un estudio.
n Sin utilidad

+
Muchas Gracias