Emergencia Cefalea
11
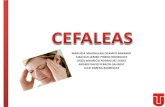
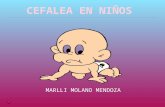
CEFALEA EMERGENCIA SALUDESA MOTIVO DE CONSULTA Cefalea / “Migraña” / Mareo / Rigidez cuello / Dolor facial Problemas de Senos / Trauma cráneo encefálico ANAMNESIS Cefalea de inicio: súbito / gradual / incierto que inicia a las…….horas del dia….. hoy / ayer __________ minutos / horas / dias / semanas / meses antes de llegar Se localiza en: difusa / cara / frontal / occipital / cuello / temporal / ojo (derecho / izquierdo) La cefalea de irradia al: cuello / espalda / cara Evolucióna de forma: constante / intermitente Actualmente el dolor esta: igual / peor / mejor / resuelto (hora:________ ) Síntomas ocurrieron durante: descanso / sexo / esfuerzo / trauma Esta precedido de pródromos: escotomas / nausea / vómito/ninguno Contexto: problema nuevo / recurrente / crónico Ultimo episodio similar fue hace: Frecuencia de episodio: raro /ocasional / frecuente ____epis. por mes/año Comparado con cefalea previa?: igual / no tan mal / peor / diferente Trauma reciénte?: no / si:_____________________________ Expuesto a medicamento o tóxico?: warfarina/ ASA / CO / Etanol La característica de la cefalea: no puede describir urente / presión / como martillo / como “cuchillo” / opresivo “la peor cefalea en toda mi vida” Gravedad: no puede describir En el peor momento (0-10): __________ leve / moderado / severo Actualmente (0-10): __________ nada / leve / moderado / severo Síntomas Asociados: ninguno Fiebre / debilidad / escalofríos / anorexia / sudor / mareo / fotofobia fonofobia / visión doble / visión borrosa / congestión nasal / gripe dolor garganta / dolor de cuello / rigidez cuello / nausea / vómito / diarrea Informante: paciente / familiar / amigo Anamnesis limitado por: estado mental alterado / gravedad / intoxicación / demencia / edad Referido por: / primer nivel / familiar/ SSC/ auto referencia S.V.: T: ______PA: ______ / ______ P: ______ FR: _____ Sat
-
Upload
carlos-troya-altamirano -
Category
Documents
-
view
20 -
download
0
description
Ficha de autollenado para atender en sala de emergencias
Transcript of Emergencia Cefalea

CEFALEA EMERGENCIA SALUDESA
MOTIVO DE CONSULTACefalea / “Migraña” / Mareo / Rigidez cuello / Dolor facialProblemas de Senos / Trauma cráneo encefálico
ANAMNESISCefalea de inicio: súbito / gradual / incierto que inicia a las…….horas del dia….. hoy / ayer __________ minutos / horas / dias / semanas / meses antes de llegar
Se localiza en: difusa / cara / frontal / occipital / cuello / temporal / ojo (derecho / izquierdo) La cefalea de irradia al: cuello / espalda / cara Evolucióna de forma: constante / intermitente Actualmente el dolor esta: igual / peor / mejor / resuelto (hora:________ ) Síntomas ocurrieron durante: descanso / sexo / esfuerzo / traumaEsta precedido de pródromos: escotomas / nausea / vómito/ninguno Contexto: problema nuevo / recurrente / crónico Ultimo episodio similar fue hace:Frecuencia de episodio: raro /ocasional / frecuente ____epis. por mes/añoComparado con cefalea previa?: igual / no tan mal / peor / diferente Trauma reciénte?: no / si:_____________________________Expuesto a medicamento o tóxico?: warfarina/ ASA / CO / Etanol La característica de la cefalea: no puede describir urente / presión / como martillo / como “cuchillo” / opresivo “la peor cefalea en toda mi vida” Gravedad: no puede describir En el peor momento (0-10): __________ leve / moderado / severo Actualmente (0-10): __________ nada / leve / moderado / severo Síntomas Asociados: ninguno Fiebre / debilidad / escalofríos / anorexia / sudor / mareo / fotofobiafonofobia / visión doble / visión borrosa / congestión nasal / gripe dolor garganta / dolor de cuello / rigidez cuello / nausea / vómito / diarreatos / hemoptisis / palpitaciones / dolor precordial / sincope / convulsión confusión / agitación / obnubilación / ansiedad / estrés / depresiónSe alivia: con nada Acostado / quieto / uso medicamentos_______________________________Se agrava por: nada Cambio de posición: acostado / sentado / parado /movimiento /
Informante: paciente / familiar / amigoAnamnesis limitado por:estado mental alterado / gravedad / intoxicación / demencia / edad Referido por: / primer nivel / familiar/ SSC/ auto referenciaLlegó por: caminando / silla ruedas / policia / vehiculo
S.V.: T: ______PA: ______ / ______ P: ______ FR: _____ Sat O2 (%): ________

Alergia: ninguna / latex / PCN / sulfa / contraste Rayos X
Medicamentos: ningunoOtro:
Antecedentes Patológicos: ningunoCluster / Migraña / Tensión / sinusitis /gripeSíndrome Articulación Temporo-MandibularGlaucoma / HTA / trauma cefálica / contusión cefálica / concusión / cirugía cefálica hemorragia subaracnoideSe realizo TAC o RM hace…..con el siguiente resultado
Antecedentes Familiares: desconocidosHemorragia subaracnoide / HTA / ECVOtro:
Antecedentes Sociales: desconocidos Alcohol: positivo, negativo Ocupación: desempleado estudiante jubilado empleado: _________________________ Vivienda: casa /departamento / rancho Vive con: solo / compañero / hijos / padres esposo(a)Violencia Doméstica: no si
REVISIÓN DE SISTEMAS__ Constitucional: fiebre / escalofríos / mareos / baja de peso__ Ojos: problemas visuales / visión borrosa / ojo rojo / escleras ictéricas__ ORL: dolor cuello / dolor garganta / dolor oído/ congestión__ CV: dolor toráxico / palpitaciones / ortopnea / disnea paroxística nocturna / edemas pre tibiales__ Respiratorio: disnea / sibilancias / hemoptisis / tos __ GI: dolor abdominal / nausea / vomito/ diarrea / sangre heces__ GU: disuria / urgencia / poliuria / hematuria / __ Musculoesqueletico: mialgias / artralgias / áreas dolorosas__ Piel: rash / problemas de piel __ Neurológico: cefalea / convulsiones/ sincope / déficit neurológico__ Psiquiátrico: stress / ansiedad / depresión / insomnio / alucinaciones__ Hemato/Linfatico: heridas / sangrado / nódulos linfáticos__ Endocrino: poliuria /polidipsia /problema tiroideos/problema adrenal__ Inmunológico: Uso inmunodepresores / HIV / cáncerTodos negativos

EXAMEN FÍSICO
Ortostatismo SV: O-- : PA= ________ P= _________ : PA= ________ P= _________
Examen limitado por: condición crítica del paciente / pcte no colaboraEstado general: alerta / letárgico / confundido / obnubiladoOrientado: en persona / tiempo espacioPresenta ansiedad: leve / moderada / severaDistres: leve / moderado / severoEstado nutricional: Normal / caquéctico / obesoHidratación: conservada / deshidratadoPiel: ___ tibia y seca___ no ronchas, no eritema ___ no ronchas, no eritema Linfático: ___ no adenopatía cervical, axilar, inguinal Ojos:___ parpados, esclera NL, Pupilas I,R,R., MEO íntegras ___ fondo NL ORL, Cuello: ___ fosas nasales permeables, no secreción___ Tímpanos NL, no abombados ___ faringe no eritema, no pus___ cuello suave, no soplos o masas Cardiovascular: ___ FC y ritmo normales ___ R1&R2 normales, no soplo ___ pulsos iguales y simétricos bilaterales. Respiratorio: ___ no distres respiratorio___ Campos claros bilateralmente ___ pared torácica no sensible Gastrointestinal / Abdomen / Espalda ___ inspección y ruidos intestinales NL ___ suave, no sensible, no masas ___ Flancos y espalda no sensibles Musculo esquelético: no deformidad, no sensibilidad___ fuerza muscular conservada
Neurológico: ___ Pares craneales 2-12 respuesta normal___ fuerza motriz conservada y simétrica ___ sensibilidad superficial intacta ___ reflejos iguales y simétricos Psiquiátrico: ___ personalidad normal ___ no ideación suicida u homicida
TRATAMIENTO
Monitoreo no invasivo
O2 __________ L/minuto / con bigotera / mascarilla para mantener % sat > 94%
Solución Salina I.V. …..ml .en bolo y luego Infusión continua _______ ml/hora
EXAMENES ___ EMO ___ Biometría Hematica___ Química Sanguínea ___ Punción Lumbar___ TAC Cabeza (transferencia)
DIAGNOSTICO:DIAGNOSTICO DIFERENCIALGlaucoma S. T.M. Tensión/Estrés Absceso Cerebral Migraña Sinusitis Cluster Meningitis CO toxicidadContusión Cerebral Concusión EncefalitisHematoma: subdural / epidural Hemorragia subaracnoidea

Tempra / Ibuprofeno / Diclofenaco ______mg VO / IM / IV/ I.R. Sosegon / Tramal / Sistalgina ________mg VO / IM / IV
Metoclopramide 10mg IV
Considerar TAC si hay: inicio súbito déficit neurológico dolor que le despierta en la noche vomito persistente
”peor cefalea de mi vida”
Disposición: Alta Ingreso Observación Transferencia
Medico:___________________________________________
SLMC SLSS WAMH
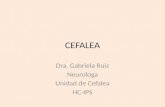
Check ( )for normals, circle positives , slash negatives, for test ordered or task performed Date: ________________ Time Seen: __________ Age: _________ PMD: ________________Temp: ____________ BP: ________ / _________P: ________ RR: ______ POX (%): ________ Chief Complaint: headache / “migraine HA” / neck stiffness / dizziness lightheadedness / facial pain / sinus problems / head trauma / _________________________
Historian: patient / family / friend / EMS / interpreter /Hx & ROS limited by: altered mental status / acuity / intoxication / dementia / ageReferred by. Self / clinic / PMD / family / EMS /Arrived by: EMS / walk-in / wheelchair / police / car driven by: self / friend / family /Advanced Directive: none / DNR / “full code” / comfort care /
Onset: sudden / crescendo-onset HA / gradual / unsure Began: _____________________ time ____________________ date today / yesterday _______________________ minutes / hrs / days / weeks / months prior to arrival Location: diffuse / frontal / occipital / face / neck(right / left ) temporal / eye /Radiation: neck / back / face /Course / Timing / Duration: constant / intermittent Course: same / fluctuating / worse / improved / resolved (time:______________________ ) Duration, frequency of HA’s: ______________________________________________________ ______________________________________________________________________________Symptoms occurred: rest / exertion / during sex / “woke up with HA” / traumaProdrome: none / scintillating scotoma / fortification spectrum / nausea / vomiting______________________________________________________________________________ Context: new problem / recurrent / chronic If recurrent HA, last HA of similar quality: ___________________________________________ HA frequency: rare / occasional / frequent ________________ HA’s per month / year HA history: migraine /cluster / tension / _____________________________________________ HA workup: none / CT scan _________ / MRI _______________ / neurology consult Compared to other HA’s: same / not as bad / worse / worst ever / different type Recent trauma or head injury? ____ no yes: _________________________________________ Medication or Toxin Exposure: coumadin / plavix / aspirin / ETOH / cocaine / CO Character / Quality: can’t describe aching / dull / “ pain” / pounding / pressure / sharp / squeezing / stabbing
Headache # 05
HPI: L1-3: 1-3 elements; L4-5: 4+ elements

tearing / “thunderclap” HA / throbbing / “worst HA of my life” / _______________________________________________________________________________ Severity: can’s describe At max (0 to 10): __________ mild / moderate / sever Now (0 to 10): __________ none / mild / moderate / sever Associated Sx: ___ none fever / weakness / dizziness / chills / malaise / blurred vision / double visionphotophobia / phonophobia / nasal congestion / URI Sx / flu Sx / facial pain sore throat / neck pain / neck stiffness / cough / nausea / vomiting / diarrhea syncope / seizure / confusion / obtunded / agitation / behaviour change / stress anxiety / depression / _____________________________________________________________
Alleviated / Relieved by: ___ nothing Lying still / medications: _________________________________________________________Aggravated / Exacerbated by: ____ nothing Change in position / head movement / stting up / standing / ____________________________________________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________
Allergy: __ NKDA see ED record / latex / PCN / sulfa / contrast medium /_________________________________________________________________Medications: ___ none see ED record aspirin / digoxin / coumadin_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________PMH / Surgical Hx: ___ none unsure / see ED recordmigraine HA / cluster HA / “tension” HA / sinusitis / URI / glaucomaHTN / hypercholesterolemia / NIDDM / IDDM / CAD / MI afib / CHF / COPD / DVT / PE / PUD / GI bleedUTI / TIA / CVA / hypothyroidism / LBP / cancerhead trauma / concussion / brain surgery / ventricular-peritoneal shuntappendectomy / cholecystectomy / CABGpacemaker / AICD / cardiac cath _____________ / stress test ______________________________________________________________________________________________________________ / Tetanus immunization current: yes / noSocial Hx: unknown Tobacco use: _____ no yes: _____ cigarettes / packs per day / weekETOH: _____ no yes: ______ drinks per day / week Last ETOH: _________Drug use: _____ no yes: cocaine / marijuana / ________________________Occupation: unemployed / student / retired / employed: __________________________________________________________________________________Lives: house / apartment / homeless / homeless shelter / group home /assisted living / nursing home / ______________________________________Living situation: alone / significant other / children / parents /Domestic Violence: ____ no yes:_____________________________________Family HX: noncontributory / unknown / HTN / subarachnoid hemorrhageCVA /
Past Medical, Family, Social hx:L1-4: 1 area; L5: 2 of 3 areas
ROS: L1-3: 1 system; L4: 2-9 systems; L5: 10+systems

All 14 systems reviewed: __ neg __ neg except as per HPI and/or circle below
__ Constitutional: fever / chills / malaise / weight loss__ Eyes / Mouth: visual problems / photophobia / redness / dental pain__ ENT: sore throat / congestion / ear pain / TMJ problems __ CV: chest discomfort / palpitations / orthopnea / PND / ankle swelling__ Respiratory: SOB / DOE / wheezing / hemoptysis / cough__ GI: abdominal discomfort / nausea / vomiting / diarrhea / tarry stools / rectal bleeding / constipation __ GU: dysuria / urgency / frequency / hesitation / hematuria / kidney problems) LMP: _________________: ___ WNL abnormal __ Musculoskeletal: myalgias / painful areas:__ Skin: rash / skin problems__ Neurologic: weakness / blackouts / numbness / tingling / seizures / Confusion / neck stiffness__ Psychiatric: stress / anxiety / depression / insomnia / hallucinations__ Hematology / Lymphatic: bruising / bleeding / swollen lymph nodes__ Endocrine: polyuria / polydipsia / thyroid problems __ Immunology / Allergy: HIV / Immunosuppressant therapy / cancer
Saludesa SLMC SLSS WAMH Headache # 05
Physical Exam: L2-3: 2-4 organ/areas; L4: 5-7 organ/areas; L5: 8+ organ/areas
VS Reviewed Exam limited by: urgency of condition / patient uncooperative
General: alert / lethargic / confused / obtunded Oriented: person / place / timeAnxious: mild / moderate / severe Distress: mild / moderate / severeNutritional status:___ WNL cachetic / obese Hydration: ___ WNL dehydrated
Orthostatic VS: O- : BP= _______ P= ________ : BP= ________ P= _________
Eyes: Musculoskeletal:___ lids, sclera WNL, PERRL bil , EOM intact ___ no deformity, no tenderness___ funduscopic exam WNL bil. ___ muscle strength grossly intac ENT, Neck: Skin: ___ nares patent, no discharge ___ warm and dry___ TM not injected, no bulging ___ no rash, no erythema ___ pharynx not injected, no exudates ___ no peripheral edema ___ neck supple, no bruits or masses Neurologic: Cardiovascular: ___ CN II-XII grossly intac ___ regular rate and rhythm ___ motor strength equal and symmetric ___ normal S1&S2, no murmur ___ light touch sensation intac ___ pulses equal and symmetric bilaterally ___ reflexes equal and symmetric Respiratory: ___ no nuchal rigidity, no neck stiffness ___ no respiratory distress Psychiatric: ___ lungs CTA bilaterally ___ affect and mood normal ___ chest wall non-tender ___ no suicidal or homicidal ideation Gastrointestinal / Abdomen / Back Lymphatic: ___ inspection and bowel sounds normal ___ no cervical lymphadenopathy ___ soft, non-distended, no masses ___ no axillary lymphadenopathy ___ no flank or back tenderness ___ no inguinal lymphadenopathy ___ rectal exam normal, heme neg. stool Genitourinary, FemaleGenitourinary, Male ___ external genitalia without lesions

___ external genitalia normal, no discharge ___ no cervical motion tenderness ___ testicles normal, no masses, no hernia ___ no cervical discharge ___ prostate not enlarged, no masses ___ uterus, adnexa non-terder, no mass Comments:
subarachnoid hemorrhage glaucoma TMJ syndromemeningitis / brain abscess migraine HA cerebral sinus thrombosistumor cluster HA pseudotumor cerebrisubdural / epidural hematoma tension HA hypertensive headacheintracerebral bleed sinusitis dehydrationcarbon monoxide poisoning trigeminal neuralgia temporal arteritis shingles
bronchitis anxiety / pani
Monitor ECG: ready by ED MD and compared to ECG from _________________
Rhythm: NSR / ST / a-fib / paced Rate: ______ Intervals: ____ WNL QRS:____ WNL ST-T wave: ___ WNL: _____________________________________________________ Other: ECG unchanged / ___________________________________________________
Lab: Lab Results Reviewed U/A: ___ WNL ___ WNL except:
CBC: ___ WNL ___ WNL except: RBCs_______ WBCs ________
Chem: ___ WNL ___ WNL except Bacteria ________
CSF fluid analysis:
Opening Pressure: __________ RBCs: __________ (tube # 4) RBCs: __________ (tube # 1) Xanthochromia: ___ neg pos
Total Protein: _____________ __ Bands __ Segs ___ Lymphs __ Monos Anion Gap= Glucose: _________________ WBCs: __________________
Culture: Urine / Blood / CSF Segs _____ Lymphs _______
ESR: _____ WNL _________ Monos ____
INR: ____ WNL ___________ Gram Stain: ______________
CO level: ____ WNL _______
Radiology:
1- Head CT scan _____________________________________________________
____ WNL _______________________________________________________ 2- _________________________________________________________________
____ WNL ______________________________________________________ 1- Read by: ED MD / Radiology Report 2- Read by: ED MD / Radiology Report
Treatment / Management Options / Course: O2 at __________ L/minute / % FiO2 (NC, face mask, _____________________ )
IV cap / infusion (NS, _____); Bolus ______________ mL; Rate _______ mL/hr
Acetaminophen / Ibuprofen _________________ mg PO Vicodin / Percocet 1 / 2 PO
Zofran 2 / 4 ____ mg IV / PO Benadril 25 / 50 mg IV / PO
Compazine 5 / 10 mg IV / IM / PO Haldol / Droperidol 2.5 / 5 mg IV / IM
Benadryl 25 / 50 mg IV / IM / PO Toradol 15 / 30 / 60 mg IV / IM
Morphine sulphate _____ mg IV ; repeated x 1 2 3 4 ; total dose= ___________ mg
______________________________________________________________________________________________________________________________________________
Diagnostic Considerations: circle or write potential diagnoses
Medical Decision Making: L1: straightforward; L2-3: low/complex; L4: mod; L5:highMark box if test ordered or task done, check normals , circle and note abnormals

_____________________________________________________________________________________________________________________________________________________________________________________________________________________
Pain Level: ___ / 10 @ _________ ; ___ / 10 @ _________ ; ____ / 10 @ ___________Course: same / worse / improved / resolved Patient evaluated and examined by MD
Level: ___1 ____ 2 ____ 3 ___ 4 ___ 5 _____________________ _______________ physician # PA #Critical Care Time (excluding procedures) = _______________________ minutes ED Observation Admission ED Fast TrackConsultation / Other Data Reviewed:Consulted Dr(s): _______________________________________ @ ______________Suggests: admit / discharge / will see: _____________________________________Case discussed with: patient / family / Radiologist / PMD / ______________________Reviewed: Nursing Home / EMS / RN / Old Records from _______________________Clinical Impression (circle or write diagnoses):
headache hypertensionmigraine headache meningitistension headache subarachnoid bleednausea / vomiting cerebrovascular accidentdehydrationfever / sinusitis
Disposition: time: __________________ Discharge Admit: OBS beb / general / Tele / medical / surgical / ICU
Transfer ____________________________ to Dr._________________________
Follow up: PMD / ______________________ in / on _______ days / prn / as scheduledCondition: good / stable / serious / critical Isolation: none / droplet / contact / airborne Restrictions: off work / limited duty / gym / school for __________________________ Discharge Instructions given: verbal / written / via interpreter Discharge Rx: ibuprofen / vicodin / percocet / ____________________________________ MD / DO / PA Date ______________ ____________________________________ MD / DO / PA Date ______________ ____________________________________ MD / DO / PA Date ______________
Addendum: _______ template complete, dictation pending
See: template / dictation template complete, full / partial dictation complete
See RN Notes & ED Chart template complete, no dictation needed