ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
10
ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS Dra. Isabel Lastra R1 Medicina Interna
-
Upload
macrisgabela -
Category
Documents
-
view
218 -
download
0
Transcript of ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 1/10
ENFERMEDAD ARTERIAL
CORONARIA EN PACIENTESDIABÉTICOS
Dra. Isabel Lastra
R1 Medicina Interna

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 2/10
Prevalencia
� Alta prevalencia de enfermedad arterialcoronaria
�
Mayor extensión de isquemia miocárdica� Infarto al miocardio
� Isquemia al miocardio silente.

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 3/10
Diabetes como equivalente de CHD
� Análisis de 698.782 personas
� Riesgo de enfermerdad arterial coronaria de 2·00(95% CI 1·832·19)
� Mujeres > Hombres (4059 años)� Mortalidad 11 vs 10% por enfermedades
vasculares.
�
2 veces más riesgo de enfermedades vascularesindependientemente de otros factoresconvencionales.
Emerging Risk Factors Collaboration, Diabetes mellitus, fasting blood glucose concentration, and risk of vascular
disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010 Jun 26;375(9733):2215-22

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 4/10
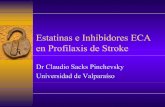
Figure 1.
Hazard ratios (HRs) for vascular outcomes in people with versus those without diabetes atbaselineAnalyses were based on 530 083 participants. HRs were adjusted for age, smoking status, bodymassindex, and systolic blood pressure, and, where appropriate, stratified by sex and trial arm.208 coronary heart disease outcomes that contributed to the grand total could not contribute tothe subtotals of coronary death or non-fatal myocardial infarction because there were fewer
than 11 cases of these coronary disease subtypes in some studies. *Includes both fatal and nonfatalevents.

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 5/10
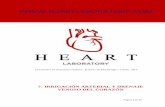
Hazard ratios (HRs) for coronary heart disease and ischaemic stroke in people with versus those without diabetes at baseline,by individual characteristicsHRs were adjusted as described in figure 1. BMI=body-mass index. *Bottom third=<23·8 kg/m2 (mean 21·7 kg/m2); middlethird=23·8<27 kg/m2 (mean 25·3 kg/m2); and top third=27 kg/m2 (mean 30·7 kg/m2). Bottom third=<123 mmHg (mean
113 mmHg); middle third=123<141 mmHg (mean 132 mmHg); and top third=141 mmHg (mean 157 mmHg

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 6/10
Extensión de enfermedad coronaria
TIDetection of coronary artery disease in asymptomatic patients with type 2 diabetes mellitus.AUScognamiglioR, Negut C, Ramondo A, Tiengo A, Avogaro ASOJ Am Coll Cardiol. 2006;47(1):65-71.
In type 2 diabetes mellitus (DM2) patients, coronary artery disease (CAD) generally is detected in an advanced stage, whereas anasymptomatic stage is commonly missed. Abnormal myocardial perfusion during stress myocardial contrast echocardiography
(MCE) and significant CAD were similar, irrespective of risk factor (RF) profile in our patients, but coronary anatomy differed. An"aggressive" diagnostic approach, requiring coronary angiography in asymptomatic DM2 patients with<or = 1 associated RF forCAD and abnormal MCE, identified silent CAD, characterized by a more favorable angiographic anatomy. The criterion of>or = 2RFs did not help to identify patients with a higher prevalence of CAD and is only related to a more severe coronaryatherosclerosis with unfavorable anatomy.OBJECTIVES: We sought to verify the effectiveness of current American DiabetesAssociation screening guidelines in identifying asymptomatic patients with coronary artery disease (CAD) in type 2 diabetesmellitus (DM2). BACKGROUND: In DM2 patients, CAD generally is detected in an advanced stage with an extensiveatherosclerosis and poor outcome, whereas CAD in an asymptomatic stage is commonly missed. METHODS: This study included1,899 asymptomatic DM2 patients (age<or = 60 years). Of these, 1,121 had>or = 2 associated risk factors (RFs), group A, and theremaining 778 had<or = 1 RF, group B, for CAD. All patients underwent dipyridamole myocardial contrast echocardiography(MCE), and in those with myocardial perfusion defects, the anatomy of coronary vessels was analyzed by selective coronary
angiography. RESULTS: In the two study groups, the prevalence of abnormal MCE (59.4% vs. 60%, p = 0.96) and of a significantCAD (64.6% vs. 65.5%, p = 0.92) was similar, irrespective of RF profile. But coronary anatomy differed: group B had a lowerprevalence of three-vessel disease (7.6% vs. 33.3%, p<0.001), of diffuse disease (18.0% vs. 54.9%, p<0.001), and of vesselocclusion (3.8% vs. 31.2%, p<0.001), whereas one-vessel disease was more frequent (70.6% vs. 46.3%, p<0.001). Coronaryanatomy did not allow any revascularization procedure in 45% of group A patients. CONCLUSIONS: An "aggressive" diagnosticapproach, requiring coronary angiography in asymptomatic DM2 patients with<or =1 associated RF for CAD and abnormal MCE,identified patients with a subclinical CAD characterized by a more favorable angiographic anatomy. The criterion of>or =2 RFs didnot help to identify asymptomatic patients with a higher prevalence of CAD and is only related to a more severe CAD withunfavorable coronary anatomy.

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 7/10

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 8/10
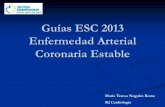
Infarto al miocardio
� 24� TI� Cardiovascular events in diabetic and nondiabetic adults with or without history of myocardial infarction.� AU� Lee CD, Folsom AR, PankowJS, Brancati FL, Atherosclerosis Risk in Communities (ARIC) Study Investigators� SO� Circulation. 2004;109(7):855-60.�
� BACKGROUND: Whether diabetic patients without a history of myocardial infarction (MI) have the same risk of coronary heart disease (CHD) eventsas nondiabetic patients with a history of MI remains controversial. We compared risks of CHD and stroke events and mortality from cardiovasculardisease (CVD) in diabetic and nondiabetic men and women with and without a history of MI. METHODS AND RESULTS: We followed a total of 13 790African American and white men and women ages 45 to 64 years who participated in the Atherosclerosis Risk in Communities study, beginning in1987 to 1989. There were 634 fatal CHD or nonfatal MI events, 312 fatal or nonfatal strokes, and 358 deaths from CVD during an average of 9 yearsof follow-up (125 998 person-years). After adjustment for age, sex, race, Atherosclerosis Risk in Communities field center, and multiple baseline riskfactors, patients who had a history of MI without diabetes at baseline had 1.9 times the risk of fatal CHD or nonfatal MI (95% CI, 1.35 to 2.56;P<0.001) compared with diabetic patients without a prior history of MI. The nondiabetic patients with MI also had 1.8 times the risk of CVD mortalitycompared with diabetic patients without MI (95% CI, 1.22 to 2.72; P=0.003). However, stroke risk was similar between diabetic patients without MIand nondiabeticpatients with MI (RR, 1.05; 95% CI, 0.61 to 1.79; P=0.87). We also observed that nondiabetic patients with MI had a carotid arterywall thickness similar to diabetic patients without MI (P=0.77). CONCLUSIONS: Diabetic patients without MI had lower risk of CHD events andmortality from CVD compared with nondiabetic patients with MI, but stroke risk was similar between these 2 groups.
� AD� Department of Sports and Exercise Sciences, West Texas A&M University, Canyon, Tex, USA.� PMID� 14757692� No diabetes and no MI 3.9 percent� Diabetes and no MI 10.8 percent� No diabetes and prior MI 18.9 percent� Diabetes and prior MI 32.2 percent

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 9/10
ISQUEMIA SILENTE E INFARTO
Desnervación autonómica delcorazón (regional)
Inestabilidad eléctrica miocárdica
Arritmias
Alteración en la percepción deangina

8/7/2019 ENFERMEDAD ARTERIAL CORONARIA EN PACIENTES DIABÉTICOS
http://slidepdf.com/reader/full/enfermedad-arterial-coronaria-en-pacientes-diabeticos 10/10
Enfermedad arterial coronariaasintomática
� Asociación con calcificación de arteriascoronarias
� Isquemia silente e infarto
Desnervación autonómica del corazón
inestabilidad eléctrica miocárdica