Envejevimiento Celular- Telomerasas
3
CHAPTER 1 Cell Injury , Cell Deat h, and Adaptations 26 CELLULAR AGING Individuals age because their cells age. Although public attention on the aging process has traditionally focused on its cosmetic manifestations, aging has important health consequences, because age is one of the strongest indepen- dent risk factors for many chronic diseases, such as cancer, Alzheimer disease, and ischemic heart disease. Perhaps one of the most striking discoveries about cellular aging is that it is not simply a consequence of cells’ “running out of steam,” but in fact is regulated by a limited number of genes and signaling pathways that are evolutionarily con- served from yeast to mammals. Cellular aging is the result of a progressive decline in the life span and functional capacity of cells. Several mechanisms are thought to be responsible for cellular aging ( Fig. 1–29): • DNA damage. A variety of metabolic insults that accu- mulate over time may result in damage to nuclear and mitochondrial DNA. Although most DNA damage is repaired by DNA repair enzymes, some persists and accumulates as cells age. Some aging syndromes are associated with defects in DNA repair mechanisms, and the life span of experimental animals in some models can be increased if responses to DNA damage are enhanced or proteins that stabilize DNA are introduced. A role of free radicals in DNA damage leading to aging has been postulated but remains controversial. • Decreased cellular replication. All normal cells have a limited capacity for replication, and after a fixed number of divisions cells become arrested in a terminally nondi- viding state, known as replicative senescence. Aging is associated with progressive replicative senescence of cells. Cells from children have the capacity to undergo more rounds of replication than do cells from older people. In contrast, cells from patients with Werner syn- drome, a rare disease characterized by premature aging, have a markedly reduced in vitro life span. In human cells, the mechanism of replicative senescence involves progressive shortening of telomeres, which ultimately results in cell cycle arrest. Telomeres are short repeated sequences of DNA present at the ends of linear chromo- somes that are important for ensuring the complete rep- lication of chromosome ends and for protecting the ends from fusion and degradation. When somatic cells repli- cate, a small section of the telomere is not duplicated, cells that have lost their ability to regulate intracellular calcium. After initiation in either location, propagation of crystal formation occurs. This is dependent on the concen- tration of Ca 2+ and PO 4 − , the presence of mineral inhibitors, and the degree of collagenization, which enhances the rate of crystal growth. Metastatic Calcification Metastatic calcification can occur in normal tissues when- ever there is hypercalcemia. The major causes of hypercal- cemia are (1) increased secretion of parathyroid hormone, due to either primary parathyroid tumors or production of parathyroid hormone–related protein by other malignant tumors; (2) destruction of bone due to the effects of acceler- ated turnover (e.g., Paget disease), immobilization, or tumors (increased bone catabolism associated with multiple myeloma, leukemia, or diffuse skeletal metastases); (3) vitamin D–related disorders including vitamin D intoxication and sarcoidosis (in which macrophages activate a vitamin D precursor); and (4) renal failure, in which phosphate reten- tion leads to secondary hyperparathyroidism. MORPHOLOGY Regardless of the site, calcium salts are seen on gross exami- nation as fine white granules or clumps, often felt as gritty deposits. Dystrophic calcification is common in areas of caseous necrosis in tuberculosis. Sometimes a tuberculous lymph node is essentially converted to radiopaque stone. On histologic examination, calcification appears as intracellular and/or extracellular basophilic deposits. Over time, hetero- topic bone may be formed in the focus of calcification. Metastatic calcification can occur widely throughout the body but principally affects the interstitial tissues of the vas- culature, kidneys, lungs, and gastric mucosa. The calcium deposits morphologically resemble those described in dys- trophic calcification. Although they generally do not cause clinical dysfunction, extensive calcifications in the lungs may be evident on radiographs and may produce respiratory defi- cits, and massive deposits in the kidney (nephrocalcinosis) can lead to renal damage. SUMMARY Abnormal Intracellular Depositions and Calcifications Abnormal deposits of materials in cells and tissues are the result of excessive intake or defective transport or catabolism. • Depositions of lipids Fatty change: accumulation of free triglycerides in cells, resulting from excessive intake or defective transport (often because of defects in synthesis of transport pro- teins); manifestation of reversible cell injury Cholesterol deposition: result of defective catabolism and excessive intake; in macrophages and smooth muscle cells of vessel walls in atherosclerosis • Deposition of proteins: reabsorbed proteins in kidney tubules; immunoglobulins in plasma cells • Deposition of glycogen: in macrophages of patients with defects in lysosomal enzymes that break down glycogen (glycogen storage diseases) • Deposition of pigments: typically indigestible pigments, such as carbon, lipofuscin (breakdown product of lipid peroxidation), or iron (usually due to overload, as in hemosiderosis) • Pathologic calcifications Dystrophic calcification: deposition of calcium at sites of cell injury and necrosis Metastatic calcification: deposition of calcium in normal tissues, caused by hypercalcemia (usually a consequence of parathyroid hormone excess)
-
Upload
prometeo01 -
Category
Documents
-
view
222 -
download
0
Transcript of Envejevimiento Celular- Telomerasas

7/27/2019 Envejevimiento Celular- Telomerasas
http://slidepdf.com/reader/full/envejevimiento-celular-telomerasas 1/3
CHA P T E R 1 Cell Injury, Cell Death, and Adaptations26
CELLULAR AGING
Individuals age because their cells age. Although publicattention on the aging process has traditionally focused onits cosmetic manifestations, aging has important healthconsequences, because age is one of the strongest indepen-dent risk factors for many chronic diseases, such as cancer,Alzheimer disease, and ischemic heart disease. Perhapsone of the most striking discoveries about cellular aging isthat it is not simply a consequence of cells’ “running out ofsteam,” but in fact is regulated by a limited number ofgenes and signaling pathways that are evolutionarily con-served from yeast to mammals.
Cellular aging is the result of a progressive decline in the lifespan and functional capacity of cells. Several mechanisms arethought to be responsible for cellular aging (Fig. 1–29):
• DNA damage. A variety of metabolic insults that accu-mulate over time may result in damage to nuclear andmitochondrial DNA. Although most DNA damage isrepaired by DNA repair enzymes, some persists and
accumulates as cells age. Some aging syndromes areassociated with defects in DNA repair mechanisms, andthe life span of experimental animals in some modelscan be increased if responses to DNA damage areenhanced or proteins that stabilize DNA are introduced.A role of free radicals in DNA damage leading to aginghas been postulated but remains controversial.
• Decreased cellular replication. All normal cells have alimited capacity for replication, and after a xed numberof divisions cells become arrested in a terminally nondi-viding state, known as replicative senescence. Aging isassociated with progressive replicative senescence ofcells. Cells from children have the capacity to undergomore rounds of replication than do cells from older
people. In contrast, cells from patients with Werner syn-drome, a rare disease characterized by premature aging,have a markedly reduced in vitro life span. In humancells, the mechanism of replicative senescence involvesprogressive shortening of telomeres, which ultimatelyresults in cell cycle arrest. Telomeres are short repeatedsequences of DNA present at the ends of linear chromo-somes that are important for ensuring the complete rep-lication of chromosome ends and for protecting the endsfrom fusion and degradation. When somatic cells repli-cate, a small section of the telomere is not duplicated,
cells that have lost their ability to regulate intracellularcalcium. After initiation in either location, propagation ofcrystal formation occurs. This is dependent on the concen-tration of Ca2+ and PO4
−, the presence of mineral inhibitors,and the degree of collagenization, which enhances the rateof crystal growth.
Metastatic Calcifcation
Metastatic calcication can occur in normal tissues when-
ever there is hypercalcemia. The major causes of hypercal-cemia are (1) increased secretion of parathyroid hormone, dueto either primary parathyroid tumors or production ofparathyroid hormone–related protein by other malignanttumors; (2) destruction of bone due to the effects of acceler-ated turnover (e.g., Paget disease), immobilization, or tumors(increased bone catabolism associated with multiplemyeloma, leukemia, or diffuse skeletal metastases); (3)vitamin D–related disorders including vitamin D intoxicationand sarcoidosis (in which macrophages activate a vitamin Dprecursor); and (4) renal failure, in which phosphate reten-tion leads to secondary hyperparathyroidism.
MORPHOLOGY
Regardless o the site, calcium salts are seen on gross exami-nation as fne white granules or clumps, oten elt as grittydeposits. Dystrophic calcifcation is common in areas o caseous necrosis in tuberculosis. Sometimes a tuberculouslymph node is essentially converted to radiopaque stone. Onhistologic examination, calcifcation appears as intracellular and/or extracellular basophilic deposits. Over time, hetero-topic bone may be ormed in the ocus o calcifcation.
Metastatic calcifcation can occur widely throughout thebody but principally aects the interstitial tissues o the vas-culature, kidneys, lungs, and gastric mucosa. The calciumdeposits morphologically resemble those described in dys-
trophic calcifcation. Although they generally do not causeclinical dysunction, extensive calcifcations in the lungs maybe evident on radiographs and may produce respiratory def-cits, and massive deposits in the kidney (nephrocalcinosis) can lead to renal damage.
SUMMARY
Abnormal Intracellular Depositions and Calcications
Abnormal deposits o materials in cells and tissues are theresult o excessive intake or deective transport or catabolism.
• Depositions of lipids Fatty change: accumulation of free triglycerides in cells,
resulting from excessive intake or defective transport(often because of defects in synthesis of transport pro-teins); manifestation of reversible cell injury
Cholesterol deposition: result of defective catabolism andexcessive intake; in macrophages and smooth musclecells of vessel walls in atherosclerosis
• Deposition of proteins: reabsorbed proteins in kidneytubules; immunoglobulins in plasma cells
• Deposition of glycogen: in macrophages of patients withdefects in lysosomal enzymes that break down glycogen(glycogen storage diseases)
• Deposition of pigments: typically indigestible pigments,such as carbon, lipofuscin (breakdown product of lipidperoxidation), or iron (usually due to overload, as inhemosiderosis)
• Pathologic calcications
Dystrophic calcication: deposition of calcium at sites of cell injury and necrosis
Metastatic calcication: deposition of calcium in normaltissues, caused by hypercalcemia (usually a consequenceof parathyroid hormone excess)

7/27/2019 Envejevimiento Celular- Telomerasas
http://slidepdf.com/reader/full/envejevimiento-celular-telomerasas 2/3
Cellular Aging
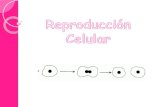
telomere length is stabilized, allowing the cells toproliferate indenitely. This is discussed more fully inChapter 5. Telomere shortening may also decreasethe regenerative capacity of stem cells, further contrib-uting to cellular aging. Despite such alluring observa-tions, however, the relationship of telomerase activityand telomere length to aging has yet to be fullyestablished.
• Defective protein homeostasis. Over time, cells are unableto maintain normal protein homeostasis, because ofincreased turnover and decreased synthesis caused byreduced translation of proteins and defective activity ofchaperones (which promote normal protein folding),proteasomes (which destroy misfolded proteins) andrepair enzymes. Abnormal protein homeostasis canhave many effects on cell survival, replication, andfunctions. In addition, it may lead to accumulation of
misfolded proteins, which can trigger pathways ofapoptosis.
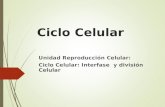
There has been great interest in dening signaling path-ways that counteract the aging process, not only becauseof their obvious therapeutic potential (the search for the“elixir of youth”) but also because elucidating these path-ways might tell us about the mechanisms that cause aging.It is now thought that certain environmental stresses, such ascalorie restriction, alter signaling pathways that inuence aging(Fig. 1–29). Among the biochemical alterations that havebeen described as playing a role in counteracting the agingprocess are reduced signaling by insulin-like growth factorreceptors, reduced activation of kinases (notably the “targetof rapamycin,” [TOR], and the AKT kinase), and altered
transcriptional activity. Ultimately these changes lead toimproved DNA repair and protein homeostasis andenhanced immunity, all of which inhibit aging. Environ-mental stresses may also activate proteins of the Sirtuinfamily, such as Sir2, which function as protein deacety-lases. These proteins may deacetylate and thereby activateDNA repair enzymes, thus stabilizing the DNA; in theabsence of these proteins, DNA is more prone to damage.Although the role of sirtuins has received a great deal ofattention recently, their importance in the aging process isnot yet established.
and telomeres become progressively shortened. As thetelomeres become shorter, the ends of chromosomescannot be protected and are seen as broken DNA, whichsignals cell cycle arrest. Telomere length is maintainedby nucleotide addition mediated by an enzyme calledtelomerase. Telomerase is a specialized RNA-proteincomplex that uses its own RNA as a template for addingnucleotides to the ends of chromosomes. Telomeraseactivity is expressed in germ cells and is present atlow levels in stem cells, but it is absent in most somatictissues (Fig. 1–30). Therefore, as most somatic cellsage their telomeres become shorter and they exit thecell cycle, resulting in an inability to generate newcells to replace damaged ones. Conversely, in immortal-ized cancer cells, telomerase is usually reactivated and
Figure 1–29 Mechanisms that cause and counteract cellular aging. DNA damage, replicative senescence, and decreased and misolded proteins areamong the best described mechanisms o cellular aging. Some environmental stresses, such as calorie restriction, counteract aging by activating varioussignaling pathways and transcription actors. IGF, insulin-like growth actor; TOR, target o rapamycin.
DNAdamage
Cellularreplication
MUTATIONS CELL LOSS
Alteredtranscription
Telomereshortening
Proteins,damaged
proteins
Insulin/IGF signaling
DNA repair
Protein homeostasis
TOR
Altered sirtuins
DECREASEDCELL FUNCTIONS
Abnormalprotein homeostasis
Environmentalstress
Environmental andmetabolic insults
COUNTERACTS AGING
ROS?
DefectiveDNA repair
CELLULAR AGING
Figure 1–30 The role o telomeres and telomerase in replicative senes-cence o cells. Telomere length is plotted against the number o celldivisions. In most normal somatic cells there is no telomerase activity, andtelomeres progressively shorten with increasing cell divisions until growtharrest, or senescence, occurs. Germ cells and stem cells both containactive telomerase, but only the germ cells have sufcient levels o theenzyme to stabilize telomere length completely. In cancer cells, telomer-ase is oten reactivated.(Data from Macmillan Publishers Ltd, from Holt SE, et al: Rening the telomer-telomerasehypothesis of aging and cancer. Nat Biotechnol 14:836, 1996.)
T e l o m e r e l e n g t h
Cell divisions
Cancer
cells
Germ cells
S o m a t i c c e l l s
S t e m c e l l s
Growth arrest

7/27/2019 Envejevimiento Celular- Telomerasas
http://slidepdf.com/reader/full/envejevimiento-celular-telomerasas 3/3
CHA P T E R 1 Cell Injury, Cell Death, and Adaptations28
It should be apparent that the various forms of cellularderangements and adaptations described in this chaptercover a wide spectrum, ranging from adaptations in cellsize, growth, and function, to the reversible and irrevers-ible forms of acute cell injury, to the regulated type of celldeath represented by apoptosis. Reference is made to thesemany different alterations throughout this book, becauseall instances of organ injury and ultimately all cases ofclinical disease arise from derangements in cell structureand function.
BIBLIOGRAPHY
Auten RL, Davis JM: Oxygen toxicity and reactive oxygen species: thedevil is in the details. Pediatr Res 66:121, 2009. [A review of the pro-duction and degradation of reactive oxygen species, and their roles in cellinjury.]
Balaban RS, Nemoto S, Finkel T: Mitochondria, oxidants, and aging.
Cell 120:483, 2005. [A good review of the role of free radicals in aging.]Calado RT, Young NS: Telomere diseases. N Engl J Med 361:2353,2009. [An excellent review of the basic biology of telomeres, and how their abnormalities may contribute to cancer, aging, and other diseases.]
Chipuk JE, Moldoveanu T, Llambl F, et al: The BCL-2 family reunion.Mol Cell 37:299, 2010. [A review of the biochemistry and biology of theBCL-2 family of apoptosis-regulating proteins.]
de Groot H, Rauen U: Ischemia-reperfusion injury: processes in patho-genetic networks: a review. Transplant Proc 39:481, 2007. [A reviewof the roles of intrinsic cell injury and the inammatory response inischemia-reperfusion injury.]
SUMMARY
Cellular Aging
• Results from combination of accumulating cellular damage(e.g., by free radicals), reduced capacity to divide (replica-tive senescence), and reduced ability to repair damagedDNA
• Accumulation of DNA damage: defective DNA repair mech-
anisms; conversely DNA repair may be activated by calorierestriction, which is known to prolong aging in modelorganisms
• Replicative senescence: reduced capacity of cells to dividesecondary to progressive shortening of chromosomalends (telomeres)
• Other factors: progressive accumulation of metabolicdamage; possible roles of growth factors that promoteaging in simple model organisms
Dong Z, Saikumar P, Weinberg JM, Venkatachalam MA: Calcium incell injury and death. Annu Rev Pathol 1:405, 2006. [A review of thelinks between calcium and cell injury.]
Elliott MR, Ravichandran KS: Clearance of apoptotic cells: implica-tions in health and disease. J Cell Biol 189:1059, 2010. [An excellentreview of the mechanisms by which apoptotic cells are cleared, and howabnormalities in these clearance pathways may result in disease.]
Frey N, Olson EN: Cardiac hypertrophy: the good, the bad, and theugly. Annu Rev Physiol 65:45, 2003. [Excellent discussion of the mecha-nisms of muscle hypertrophy, using the heart as the paradigm.]
Galluzzi L, Aaronson SA, Abrams J, et al: Guidelines for the use and
interpretation of assays for monitoring cell death in higher eukary-otes. Cell Death Differ 16:1093, 2009. [A practical summary of themorphologic and other techniques for detecting and quantifying dead cells.]
Haigis MC, Yankner BA: The aging stress response. Mol Cell 40:333,2010. [A review of the role of cellular stresses in controlling the aging
process.]Hotchkiss RS, Strasser A, McDunn JE, Swanson PE: Cell death. N Engl
J Med 361:1570, 2009. [Excellent review of the major pathways of celldeath (necrosis, apoptosis, and autophagy-associated death), and their clinical implications and therapeutic targeting.]
Kenyon CJ: The genetics of ageing. Nature 464:504, 2010. [An excellentreview of the genes that inuence aging, based on human genetic syn-dromes and studies with mutant model organisms.]
Kroemer G, Marino G, Levine B: Autophagy and the integrated stressresponse. Mol Cell 40:280, 2010. [An excellent discussion of the biology,biochemical pathways, and physiologic roles of autophagy.]
Kundu M, Thompson CB: Autophagy: basic principles and relevance
to disease. Annu Rev Pathol 3:427, 2008. [A discussion of thebiology of autophagy and its potential contribution to a variety of diseasestates.]
Lin JH, Walter P, Yen TSB: Endoplasmic reticulum stress in diseasepathogenesis. Annu Rev Pathol 3:399, 2008. [A review of the biologyand disease relevance of the unfolded protein response and ER stressinduced by unfolded proteins.]
Lombard DB, Chua KF, Mostoslavsky R, et al: DNA repair, genomestability, and aging. Cell 120:497, 2005. [The role of DNA damage incellular aging.]
McKinnell IW, Rudnicki MA: Molecular mechanisms of muscleatrophy. Cell 119:907, 2004. [Discussion of the mechanisms of cellular atrophy.]
Newmeyer DD, Ferguson-Miller S: Mitochondria: releasing power forlife and unleashing the machineries of death. Cell 112:481, 2003.[Excellent review of the many functions of mitochondria, with an emphasison their role in cell death.]
Sahin E, DePinho RA: Linking functional decline of telomeres, mito-chondria and stem cells during ageing. Nature 464:520, 2010. [Anexcellent review of stem cell abnormalities that contribute to aging.]
Tosh D, Slack JM: How cells change their phenotype. Nat Rev MolCell Biol 3:187, 2002. [Review of metaplasia and the roles of stem cellsand genetic reprogramming.]
Valko M, Leibfritz D, Moncol J, et al: Free radicals and antioxidantsin normal physiological functions and human disease. Int J BiochemCell Biol 39:44, 2007. [An interesting discussion of the biochemistry of reactive oxygen and nitrogen-derived free radicals, their roles in cellinjury, and their physiologic functions as signaling molecules.]