Genu Varum en niños: Tratamiento y Diagnóstico

of 10
Transcript of Genu Varum en niños: Tratamiento y Diagnóstico
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
1/10
Genu Varum in Children: Diagnosis and Treatment
Werner C. Brooks, MD, and Richar d H. Gross, MD
Abstract
Genu varum is a relatively common finding in children. Physiologic bowing,which is seen most often, has a well-documented favorable natural history. Idio-
pathic tibia vara is the most common of the pathologic conditions that are associ-ated with bowed legs; treatment strategies vary with the patients age and the stageof disease and deformity. Genu varum may also accompany systemic conditions,such as achondroplasia, vitamin Dresistant rickets, renal osteodystrophy, andosteogenesis imperfectaall of which can result in short stature. Indications forintervention are not always well defined. A rare disorder, focal fibrocartilaginousdysplasia, usually requires no treatment. Standing radiographs of the entire lower
limbs are necessary for surgical planning, as the deformity can sometimes affectthe distal femur rather than the proximal tibia. Restoration of the mechanical axisof the limb is the principal goal of treatment; the particular type of internal fixa-tion is of secondary importance.
J Am Acad Orthop Surg 1995;3:326-335
Genu varum, known colloquially asbowlegs, is relatively common inchildren and is a frequent cause ofparental concern. In the vast major-ity of cases, genu varum will correct
with growth. A small number ofchildren have pathologic conditionsthat may result in functional andcosmetic problems if left untreated.In this article, we will review perti-nent factors in the assessment ofgenu varum, associated conditions,and treatment options.
Assessment
History
A thorough history will often dis-tinguish the relatively infrequentpathologic genu varum from themuch more common physiologic va-riety. A family history of shortstature or similar varus alignmentshould be sought; the grandparents
may be a good source for this infor-mation. The ages at attainment ofvarious developmental milestones,such as sitting independently,pulling to stand, and walking,
should be determined. It is useful toestablish whether the parents con-sider the deformity to be progres-sive. The positional sleeping andsitting habits of the child are also ofinterest.
Physical ExaminationAfter routine documentation of
the height and weight and determi-nation of their percentiles for age,the patients pelvis, knees, and feetshould be examined carefully.
Shortening of the limbs relative tothe trunk, especially rhizomelicshortening, suggests a dwarfingcondition. In ambulatory children,the appearance while standing andduring gait provides the most infor-mation. Both limbs should be ex-
amined in the frontal and sagittalplanes for asymmetry and align-ment. It should then be determinedwhether the deformity is a gradual
bowing or an abrupt angulation. Ifthe deformity is angular, its loca-tion is identified in the distal femur,the knee, or the proximal tibia.Obliquity of the popliteal crease, if
present, is a useful sign; distalfemoral varus will produce obliq-uity of the popliteal crease, whiledeformity more distal in the ex-tremity will not.
Passive rotation of the hips andmotion of the knee are noted. Liga-mentous stability of the knee is as-sessed, with particular attention tothe lateral ligamentous complex. Adynamic component of the defor-mity or lateral thrust at the knee dur-ing the stance phase of gait indicates
laxity of the lateral ligamentouscomplex. Torsion of the tibia shouldalso be routinely assessed; determi-nation of the thigh-foot angle andevaluation of the bimalleolar axis, asdescribed by Staheli et al,1 are useful
Dr. Brooks is a Resident in the Department of Or-thopaedic Surgery, Medical University of SouthCarolina, Charleston. Dr. Gross is Professor ofOrthopaedic Surgery and Pediatrics, MedicalUniversity of South Carolina.
Reprint requests: Dr. Gross, Department of Or-thopaedic Surgery, Medical University of SouthCarolina, 171 Ashley Avenue, Charleston, SC29425.
Copyright 1995 by the American Academy of Or-thopaedic Surgeons.
Journal of the American Academy of Orthopaedic Surgeons326
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
2/10
in torsional assessment. Serial pho-tographs of the standing child at theinitial and follow-up evaluationsserve as an inexpensive method ofdocumenting any progression of thedeformity.
RadiographsWe believe radiographs are un-
necessary in a young child of normalstature with physical findings com-patible with physiologic bowing.When there is a localized deformityor the child is short, full-lengthstanding radiographs (hip to ankle)should be obtained with the kneespointing straight forward. When in-ternal tibial torsion is present, the
technician often attempts to exter-nally rotate the leg (and the knee) topoint the foot straight forward;however, rotation affects thetibiofemoral and metaphyseal-dia-physeal angles and tends to minimizethe degree of deformity.2 In additionto the angular deformity present, thephyses of the femur and tibia shouldbe carefully assessed.
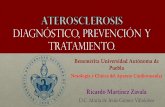
Physiologic Genu VarumPhysiologic genu varum is by far themost common cause of bowlegs in atoddler. The natural history of thechanging angular relationship be-tween the femur and the tibia in chil-dren is required knowledge for anyorthopaedist with a pediatric prac-tice. Development of the tibio-femoral angle follows a predictablesequential pattern. Infantile genuvarum progresses to excessive genuvalgum, followed a gradual correc-tion to adult physiologic valgusalignment (Fig. 1). Genu varum isgreatest at 6 months of age. Correc-tion to neutral alignment is oftencomplete by 18 months of age.Heath and Staheli3 report that per-sistence of genu varum beyond 2years of age is abnormal, and Sale-nius and Vankka4 state that neutral
alignment may not be reached until22 to 24 months of age. Even pro-nounced physiologic genu varumgreater than 30 degrees can correctwith continuing growth.3 Overcor-rection to excessive genu valgum ismaximal at 4 years of age; the valgusangulation averages 8 degrees. Cor-rection to physiologic valgus is usu-ally complete by 5 or 6 years of age.4
Early walking has been docu-mented in black children,5 and thismay be a factor in a tendency towardincreased physiologic bowing. In-ternal tibial torsion is frequentlyfound in association with physio-logic genu varum; if physiologic, itcorrects concomitantly with thegenu varum.
Radiographically, physiologicgenu varum is characterized bybowing of the entire limb. On thestanding anteroposterior radio-graph, both the distal femur and theproximal tibia will have some varus
bowing without an acute angularcomponent. The physis will appeanormal without medial physeachanges. There may be equabeaking of both the distal femoraand the proximal tibial metaphyses
The treatment of physiologicgenu varum is periodic observationand examination, together with education and reassurance of the par-ents. Occasionally, spontaneouscorrection of the physiologic genuvarum will be delayed. We believethis happens more often in childrenwho habitually sleep or sit with theirlegs rotated beneath them, as thisseems to counteract the normal unwinding effect of weight-bearing incorrecting tibial torsion and genuvarum.
Reassurance of anxious parentsor other relatives of a child withphysiologic bowing is not alwayseasy to achieve. We find that givinga copy of a graph depicting the nor-
Vol 3, No 6, November/December 1995 327
Werner C. Brooks, MD, and Richar d H. Gross, MD
+20
+15
+10
+5
-5
0
-10
-15
1 2 3 4 5 6 7 8 9 10 11
Age, yr
Valgus
Varus
12 13
Fig. 1 Graph illustrating the development of the tibiofemoral angle in children duringgrowth, based on measurements from 1,480 examinations of 979 children. Of the lighter linesthe middle one represents the mean value at a given point in time, and the other two represent the deviation from the mean. The darker line represents the general trend. (Adaptedwith permission from Salenius P, Vankka E: The development of the tibiofemoral angle inchildren. J Bone Joint Surg Am 1975;57:259-261.)
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
3/10
mal progression of genu varum togenu valgum in early childhood,along with the orthopaedists expla-nation of the graph, is extremelyhelpful. The parents can then showthe graph to other concerned rela-tives. In addition, the American
Academy of Orthopaedic Surgeonshas produced a video on commonlower-limb problems in children(Growing Out of It: Torsional De-formities in Children [No. 29-074]),which can be viewed independently
by the family.
Tibia Vara
HistoryTibia vara, often referred to as
Blounts disease, is characterized byan abrupt varus deformity of theproximal tibia. It is the most fre-quent cause of pathologic genuvarum. Unlike physiologic genuvarum, Blounts disease is progres-sive and rarely corrects sponta-neously. There are two predominanttypes of tibia varainfantile andlate-onset, or adolescentwhich aredistinguished by the age at onsetand the distinctive clinical presenta-tion. While the two types are simi-
lar in the histologic appearance ofthe proximal tibial physes, the exactetiologies remain somewhat un-clear.
Tibia vara is classified as infantilewhen the onset occurs before 5 yearsof age. Idiopathic infantile tibia varais more often seen in black, female,and obese children and in childrenwho begin to walk earlier thanusual. Involvement is bilateral in80% of patients and is associatedwith a greater degree of internal tib-ial torsion than in the adolescentform. There may be difficulty in dis-tinguishing early infantile tibia varafrom physiologic genu varum.
Children in whom significanttibia vara develops after 6 years ofage are thought to have the late-onset
form, which is less common than theinfantile type. Late-onset tibia varais more often unilateral and has agreater prevalence in black, male,and obese children and teenagers. Inhis study of the natural history oftibia vara in Finnish children, Lan-
genskild6
reported more rapid pro-gression of the varus deformity inthe infantile type than in the late-onsettype. The prevalence of morbid obe-sity in adolescents has increased inthe United States,7 and there appearsto be an associated increase in the in-cidence of late-onset tibia vara.
Children in whom pathologictibia vara later develops are bornwith normal alignment of the femurand tibia; the deformity results froma subsequent growth disturbance of
the proximal tibia. Tibia vara doesnot occur in children who do notwalk. While the exact etiology of in-fantile tibia vara remains unclear, anassociation between tibia vara andwalking at an early age and obesityin infancy suggests that mechanicalforces are at least partially causative.Early weight-bearing and obesity re-sult in greater compressive forcesacross the medial tibial physis thanin infants who are not obese andwho begin walking at about 1 year of
age. The compressed posteromedialphysis responds with slower growthin this region, producing a progres-sive varus deformity of the proximaltibia.
In the late-onset type, there isusually a mild preexisting varus de-formity, which is thought to be afactor in the development of a pro-gressive varus deformity. Whenmild genu varum persists into ado-lescence, increased body weight and
physical activity repetitively trau-matize the posteromedial physis,causing medial growth suppres-sion.8
Cook et al9 performed a two-di-mensional finite-element analysis ofthe effect of varus angulation and in-creased body weight on resultant
forces on the medial proximal tibialphysis and found that in older chil-dren, lesser degrees of varus werenecessary to produce medial phy-seal growth retardation. In a 2-year-old, 20 degrees of varus couldproduce medial tibial physeal
growth inhibition; in a 5-year-old ofnormal weight, as little as 10 degreesof varus angulation could result ingrowth inhibition.
AssessmentExamination of the child with
tibia vara is notable for an angularvarus deformity discernible just be-low the knee. In morbidly obesechildren, the acute angulation of thetibia may be hidden by their exces-sive soft tissue. In contrast, the
young child with physiologic genuvarum will have a more gentle cur-vature of the entire extremity. An in-wardly directed thigh-foot angledue to internal tibial torsion may ac-company either of these conditions,
but is more severe in infantile tibiavara. A lateral thrust, indicating lax-ity of the lateral ligamentous com-plex, may be seen in children overthe age of 3 with tibia vara. This lax-ity is thought to exacerbate the dy-namic forces across the physis
during gait and is not seen in physi-ologic bowing.
PathologyThe histopathologic findings in the
physes are the same whether the childhas infantile or late-onset tibia vara.8,10
The physeal disruption is similar tothat found in slipped capital femoralepiphysis, which may suggest a com-mon etiology. Disorganized physealcartilage is present, with disruption of
the normal columnar architecture ofthe physis, which is most evident inthe resting zone. Islands of denselypacked, unusually hypertrophic carti-lage cells are seen. Both fibrovascularand cartilaginous reparative tissuecan be found at the physeal-metaphy-seal junction.
Journal of the American Academy of Orthopaedic Surgeons328
Genu Varum in Childr en
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
4/10
RadiographsThe characteristic radiographic
appearance of tibia vara is not usu-ally present until the age of 2 years.The radiographic classification de-veloped by Langenskild6 is most of-ten used to stage the infantile forms
of the disease (Fig. 2). The potentialfor recovering growth after treat-ment is thought to be directly relatedto the stage of the disease, althoughthis staging may be more pertinentin a retrospective review thanprospectively.
Medial fragmentation of theproximal tibial metaphysis is theearliest abnormal radiographic find-ing. Later, medial physeal depres-sion and varus angulation of themetaphysis develop, with beaking
of the proximal tibial metaphysis. Invery late stages of Blounts disease,the medial physis develops an os-seous bridge between the epiphysisand the metaphysis.
As with the use of many classifi-cation systems, there is considerableinterobserver variation, and thestaging is not precise. However, the
system does provide the user withsome notion of the natural history ofprogression of the condition.Whether a given tibia demonstratesstage III or stage IV changes is lessimportant than is the recognitionthat tibia vara is well established and
the treatment that might be appro-priate for stage I or II is no longerappropriate.
In late-onset tibia vara, the radi-ographic changes are less dramatic.The growth plate shows less irregu-larity and rarely forms the physeal
bone bridge that may be seen in theinfantile form. The epiphysis is lessdeformed, producing less articularincongruity. Overgrowth of the lat-eral femoral condyle is common,and distal femoral varus may be pre-
dominant.11Levine and Drennan12 have popu-
larized measurement of the metaph-yseal-diaphyseal angle of theproximal tibia for the early differen-tiation of infantile tibia vara fromphysiologic genu varum. This angleis formed by a line drawn perpen-dicular to the tibial diaphysis and a
line drawn between the medial andlateral aspects of the tibial metaph-ysis (Fig. 3). A metaphyseal-diaphy-seal angle greater than 11 degrees isstrongly associated with subsequentdevelopment of tibia vara. In theirstudy, Levine and Drennan found
that 29 of 30 affected limbs with ametaphyseal-diaphyseal angle over11 degrees developed advancedradiographic changes consistentwith the diagnosis of tibia vara, witha false-positive rate of only 3%. Incontrast, tibia vara developed inonly 3 of 59 limbs with metaphyseal-diaphyseal angles of less than 11 de-grees.
Feldman and Schoenecker2
found the metaphyseal-diaphysealangle to be somewhat less reliable
in younger patients. On linear-regression analysis of the use of ametaphyseal-diaphyseal angle of 11degrees or more as a basis for de-ciding treatment, they found afalse-negative rate of 9% and afalse-positive rate of 33%.
With increasing age, the metaph-yseal-diaphyseal angle is more reli-
Vol 3, No 6, November/December 1995 329
Wern er C. Brooks, MD, and Richar d H . Gross, MD
Fig. 2 The six stages of tibia vara, as described by Langenskild.6 Stage I (seen in children up to age 3 years) is characterized by medial anddistal beaking of the metaphysis and irregularity of the entire metaphysis. Stage II (seen in children aged 212 to 4 years) is characterized by a
sharp lateromedial depression in the ossification line of the wedge-shaped medial metaphysis. Complete restoration is common in this stage.Stage III (seen from ages 4 to 6 years) is characterized by deepening of the metaphyseal beak, which gives the appearance of a step in the me-dial metaphysis. Stage IV (seen from ages 5 to 10 years) is characterized by enlargement of the epiphysis, which occupies the medial me-taphyseal depression. Restoration is still possible in this stage. Stage V (seen from ages 9 to 11) is characterized by a cleft in the epiphysis,which gives the appearance of a double epiphysis; the articular surface of the medial tibia is deformed, sloping distally and medially fromthe intercondylar region. Stage VI (seen from ages 10 to 13) is characterized by closure of the medial proximal tibial physis, with a normallateral physis. Langenskild described his findings on the basis of his observations of Finnish children; changes in African-American chil-dren tend to occur at a younger age.
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
5/10
able, since it tends to increase inmagnitude in patients who haveBlounts disease and decrease inmagnitude in patients with physio-logic genu varum. Rotation canhave a small but significant effect onthe radiographic measurement ofthe metaphyseal-diaphyseal angle.Henderson et al13 compared radio-graphs obtained with and withoutrotation and found a difference of 2.8 1.2 degrees in the metaphyseal-diaphyseal angles that were measured.When attempting to distinguishphysiologic genu varum from tibiavara in young patients, this amountof measuring error can be mislead-ing if one is relying on the metaphy-seal-diaphyseal angle alone for thediagnosis. If there is doubt regard-ing the radiographic findings, we be-lieve a further period of observationis indicated, rather than initiatingtreatment on the basis of blind ad-herence to arbitrary radiographicmeasurements.
TreatmentThere are still no generally ac-
cepted criteria for initiation of treat-ment in infantile tibia vara.
Although Levine and Drennan12 re-ported that a metaphyseal-diaphy-seal angle of 11 degrees could beused as a basis for treatment, othershave recommended observation ofchildren aged less than 24 monthswith metaphyseal-diaphyseal angles
of as much as 16 degrees.2
Persistentinternal tibial torsion, lateral thrustduring stance phase in gait, and pos-terolateral instability are additionalfindings that may influence a deci-sion to initiate early treatment.
There is certainly a place for ob-servation of the young child with ab-normal clinical and radiographicfindings before initiating brace orsurgical treatment. A child with ametaphyseal-diaphyseal angle ofless than 9 degrees is obviously at
minimal risk for tibia vara. If the an-gle is greater than 16 degrees, treat-ment probably should be initiated.Children with metaphyseal-diaphy-seal angles between 9 and 16 degreesare generally treated if there has
been no tendency toward correctionafter 24 months of age.
While early tibia vara will correctwithout bracing in some children(Fig. 4), bracing has often been rec-ommended as the initial treatment ofchildren with Langenskild stage I or
II tibia vara. The device usually pre-scribed is a knee-ankle-foot orthosiswith a single medial upright securedat the upper thigh and ankle. A kneehinge is not used, but this does notprevent the child from sitting. Theankle is left free. A strap at the kneeapplies a corrective valgus force. The
brace is worn nearly full-time, espe-cially during walking, to minimizethe valgus stress at the knee. The ef-fectiveness of the brace is thought to
be related to the relief of weight-bearing stresses on the medial phy-seal region of the proximal tibia.Brace treatment is reported to be suc-cessful in 50% to 80% of the patientstreated.14,15 The brace is worn untilthe deformity has been corrected andreconstitution of medial physeal
growth is present on radiographs,which usually takes about 1 year.Thus, bracing is usually not a viableoption for children over the age of3.16 Factors such as patient age, stageof the disease, family compliance,and brace fit can have an effect on the
success of bracing. Studies control-ling for all these variables have notyet been reported. However, itseems that bracing is a reasonablefirst treatment option when a deci-sion is made to start treatment ofearly tibia vara in a 2- or 3-year-oldchild.
Children who are too old for brac-ing and children in whom tibia varahas progressed despite bracing are
best treated with a proximal tibialvalgus osteotomy. The goal of the
osteotomy is to restore the mechani-cal axis of the lower extremity. Theosteotomy is performed below thetibial tubercle apophysis and is com-
bined with a fibular osteotomy.Ideally, the osteotomy is done be-
fore the child is 4 years old. Residualinternal tibial torsion can be cor-rected at the same time. If os-teotomies are first done in olderchildren, repeat osteotomies aremore often needed. Ferriter andShapiro17 retrospectively analyzed
factors affecting the outcome of 77proximal tibial osteotomies per-formed on 25 patients with tibia varaand found a 76% rate of deformityrecurrence in children operated onafter the age of 4.5 years. In youngerchildren, the rate of recurrence ofvarus deformity was 31%.
Loder and Johnston14 reportedlower rates of recurrent deformityafter valgus tibial osteotomy. Prog-nostic factors associated with a
higher rate of recurrence in theirolder patients included morbid obe-sity and more severe disease (Lan-genskild stages IV, V, or VI).
Efforts to improve the results oftibial osteotomy as treatment of in-fantile tibia vara in children olderthan 4 years include physeal-bar re-
Journal of the American Academy of Orthopaedic Surgeons330
Genu Varum in Childr en
Fig. 3 Determination of the metaphyseal-diaphyseal (MD) and tibial-femoral (TF) an-gles.
CALLOUT NEEDED
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
6/10
section and lateral proximal tibialhemiepiphysiodesis (Fig. 5). Theseprocedures were developed with anunderstanding that recurrence of thedeformity is largely due to the lackof reconstitution of growth of themedial proximal tibial physis.
Physeal bridges are more com-mon in children with infantile tibia
vara who are older than 5 years. Thepresence of a physeal bridge may beimpossible to ascertain on routineradiographs. Computed tomogra-phy or magnetic resonance imaging,with thin sections obtained throughthe physis, can be helpful in detect-ing the presence and size of the os-seous bridge.
Physeal-bridge resection is a diffi-cult operative procedure due to thedeformity of the physis, and the poor-est results have been associated withinvolvement of more than 30% of thephysis.16 Fat, cartilage, Silastic, andmethylmethacrylate have all beenused as spacers to prevent bridge re-currence after surgical resection. Fa-
Vol 3, No 6, November/December 1995 331
Wern er C. Brooks, MD, and Richar d H . Gross, MD
Fig. 4 A, Clinical appearance of a healthyboy, aged 1 year 9 months, being evaluatedfor infantile tibia vara. B, Initial radiographshows medial tibial physeal beaking and me-taphyseal-diaphyseal angles of 17 degreeson the left and 12 degrees on the right. Ob-servation without bracing was elected at thattime. C, Radiograph obtained at age 2 years3 months shows persistent medial tibial
beaking and irregularity of the proximal tib-ial physes, greater on the left than the right.D, Normal tibial alignment was seen at age 4years 10 months. E, Clinical appearance atage 4 years 10 months.
A B C
D E
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
7/10
vorable outcomes in small series ofpatients have been reported.14,18 Ac-tual growth, however, is difficult todetermine from the published radio-graphs, and our personal experiencewith this procedure has been poor. Arim of viable physis surrounding theexcised portion is necessary if growth
is to recover after partial physeal re-section. It may not be possible to de-termine on gross examination at thetime of surgery whether the remain-ing physeal rim is biologically active.
The use of lateral hemiepiphys-iodesis of the proximal tibial physisis an attractive treatment alternativein the older child with tibia vara atrisk for redevelopment of varus de-formity after proximal tibial os-teotomy alone. A formal ablation ofthe lateral tibial physis or simple sta-pling can be done (Fig. 5). Whendone unilaterally, a limb-length dis-crepancy is predictable in youngerpatients; however, treatment of thisinequality may not be needed.15
In advanced forms of infantiletibia vara (Langenskild stage IV or
greater), resultant deformity of thetibial epiphysis, as well as the physis,produces articular incongruity.Restoration of normal articularanatomy by elevation of the de-pressed medial epiphysis and physishas been reported to reconstruct the
joint architecture, generally in com-
bination with a valgus tibial os-teotomy to restore the alignment ofthe lower limb.19 Medial elevationcombined with proximal tibial os-teotomy (and occasionally distalfemoral osteotomy) has been utilizedwith success by Schoenecker et al.15
For patients with late-onset tibiavara, the indication for treatment has
been defined arbitrarily as varusalignment greater than approxi-mately 10 degrees. The goal ofsurgery is correction of the mechani-cal axis to prevent the development ofmedial knee-compartment osteo-arthrosis. Young adults with tibiavara have a high incidence of acceler-ated symptomatic degenerativechanges of the knee, which is relatedto the degree of varus malalignment.20
Treatment of the adolescent withtibia vara often involves increasedtechnical problems due to morbidobesity. Complications are morecommon than in the treatment of in-fantile tibia vara. These complica-tions include difficulty in theexposure and performance of the os-
teotomy and failure of osteotomyfixation. For these reasons, Hender-son et al21 have proposed lateralproximal tibial hemiepiphysiodesisas a primary procedure, reservingosteotomy for those cases in whichmore conservative procedures havefailed. The importance of standingradiographs of the entire lowerlimbs has recently been empha-sized.11 We believe such radio-graphs are necessary for properpreoperative planning and postop-erative assessment. The literature isreplete with techniques for the per-formance of the tibial osteotomy inlate-onset tibia vara, including vari-ous types of internal and externalfixation. Regardless of the methodof fixation chosen, the goals of
Journal of the American Academy of Orthopaedic Surgeons332
Genu Varum in Childr en
A B C
Fig. 5 A, Radiograph of a 7-year-old girl with unilateral varus deformity and severe depression of the medial tibial physis. B, A correctiveclosing-wedge proximal tibial osteotomy was performed, with stapling of the lateral proximal tibial physis. C, On radiograph obtained at 2-year follow-up examination, alignment is normal, with minimal leg-length discrepancy.
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
8/10
surgery are unchanged: correction ofthe mechanical axis and leveling ofthe knee joints.
Differential Diagnosis
Vitamin DResistant RicketsProgressive genu varum often de-
velops in children with untreatedhypophosphatemic rickets, a sex-linked inherited disorder due to vit-amin D resistance that results indefective bone mineralization. Chil-dren with this disorder typicallypresent with bilateral lower-limb an-gular deformities. The diagnosisshould be considered if the child isrelatively short, because height in af-fected children is usually in the
lower 10th percentile. The bowing isdue to a combination of varus of thedistal femur and varus of the proxi-mal tibia.
Medical treatment of this type ofrickets includes oral phosphates andsome form of vitamin D replacement.Surgical measures to correct the de-formity are often unsuccessful whenadequate medical control of the rick-ets has not been achieved beforesurgery. In that situation, it may be
best to wait until skeletal maturity torealign the mechanical axis.22 Whenonly partially treated, this conditionmay be difficult to distinguish fromphysiologic bowing, but childrenwith rickets typically are older. Mas-sive doses of a vitamin D preparationcan restore a normal radiographicappearance to the epiphysis; how-ever, normal growth will not berestored unless phosphate replace-ment is also adequate. Phosphate re-placement therapy has to be
administered at regular intervals,and patient compliance with thisstrict dosage schedule may be poor.
Renal Failure and RenalOsteodystrophy
Children who are in renal failureor who have renal osteodystrophy
have a high incidence of growth dis-turbance in both the proximal anddistal ends of the tibia. The physesin these children have been shown toexhibit many of the same pathologicchanges found in tibia vara andslipped capital femoral epiphysis,
particularly disorganized growthplates at the physeal-metaphyseal
junction.23 Deformity results wheneccentric forces occur across theweakened physis. Because renalfailure occurs more commonly inolder children who have alreadyachieved physiologic valgus align-ment, valgus deformity is encoun-tered most often at the knee.Younger children who have retainedphysiologic varus alignment mayundergo exaggeration of preexisting
genu varum. Deformities secondaryto renal disease are usually bilateral,with a gentle curve of the extremitydue to simultaneous involvement of
both the distal femoral and proximaltibial physes.
Rickets and renal osteodystrophymay be easily distinguished fromtibia vara on the basis of their radio-graphic appearance. In both, phy-seal cupping and widening occur at
both the distal femoral and proximaltibial physes. Marked osteopeniaand thinning of cortical bone are alsopresent.
Orthopaedic treatment of angularlower-limb deformities resultingfrom renal disease is wisely post-poned until the renal status has sta-
bilized in response to medicaltreatment or renal transplantation.Correction of genu varum or valgumwith osteotomy will be short-livedunless the abnormal bone metabo-lism resulting from the renal disease
has been reversed.
Metaphyseal ChondrodysplasiaMetaphyseal chondrodysplasia,
which results from abnormal chon-droblast function and chondroidproduction, is a very rare cause ofgenu varum. A number of metaph-
yseal dysplasias can lead to bowing,among them the Jansen and Schmidtypes. The more severe Jansen typehas an autosomal-dominant inheri-tance and is characterized by mentalretardation, short-limb dwarfism,exophthalmia, hypercalcemia, and
long-bone bowing. The more mildSchmid type, which is also transmit-ted by autosomal-dominant inheri-tance, is characterized by normalintellect and normal laboratory find-ings. As lower-extremity bowingdoes occur with this condition, itmay be difficult to distinguish fromrickets. Even though the physes arewidened and cupped in the Schmidtype, the epiphyses are normal, andthe presence of short stature should
be helpful in arriving at the correct
diagnosis.
AchondroplasiaGenu varum is a frequent finding
in achondroplasia, a rhizomelicdwarfing condition due to abnormalendochondral bone formation. At
birth, lower-limb alignment is rela-tively normal. However, withgrowth, the spontaneous correctionto genu valgum does not occur. In-stead, genu varum tends to increasethroughout childhood and adoles-cence, largely due to overgrowth ofthe fibula in relation to the tibia. Inaddition, the growth of the proximaltibial metaphysis may be asymmet-rical. Radiographically, the proxi-mal fibular physis is superior to theproximal tibial physis. Although thetibial metaphysis is enlarged, theepiphysis remains normal.
Children with achondroplasiararely have knee pain, and function-al indications for surgical correc-
tion of bowlegs are not well defined.Treatment options include proximalfibular epiphysiodesis and tibial os-teotomy. A fibular epiphysiodesismust be done early in childhood toprevent the development of progres-sive genu varum. For establishedgenu varum, proximal tibial valgus
Vol 3, No 6, November/December 1995 333
Wern er C. Brooks, MD, and Richar d H . Gross, MD
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
9/10
osteotomy is most often used. Anaccompanying distal tibial os-teotomy and concomitant tibiallengthening have also been advo-cated by some. The role of lengthen-ing of short limbs in this condition isstill unsettled. Bracing is ineffective,
in part because of the joint laxitycommonly present.
Osteogenesis ImperfectaOsteogenesis imperfecta results
from a defect in type I collagen andproduces varying degrees of skeletalfragility. In the more severe forms,multiple fractures of the lower ex-tremities are common. The femur ismost frequently fractured, followed
by the tibia. Repeated fractures of-ten lead to bowing and torsional de-
formities of the lower extremity. Thedistal third of the femur is a commonlocation of these fractures, usuallyassociated with anterolateral angu-lation at the fracture site. Residualdeformity after fracture is common,and the varus angulation often in-creases as a result of repeated frac-tures. Radiographs demonstratediffuse osteopenia, occasionally ac-companied by evidence of fracturehealing at multiple locations.
In cases of mild deformity, bracing
can be used for support and prophy-laxis against repeat fractures. Occa-sionally in more severe cases,pronounced bowing is present from
birth, and ambulation will not be pos-sible unless correction is undertakenearly. There are a number of optionsfor the surgical management of varusdeformity secondary to osteogenesisimperfecta; selection is dependent onthe age of the patient and the natureof the anatomic deformity.
Focal FibrocartilaginousDysplasia
Focal fibrocartilaginous dyspla-sia is a rare cause of unilateral genuvarum.24,25 It affects the proximalmedial tibia, and the resultant de-
formity is more properly termedtibia vara. The deformity is usuallyapparent to the parents before thechild is 18 months of age. Radio-graphs show a characteristic corticallucency with surrounding sclerosisin the proximal medial tibial me-
taphysis and varus angulation. Thecondition usually corrects by age4 with growth. Surgical correctionof the deformity is usually notneeded.25
Less Common CausesAny disorder that can affect the
proximal tibial or distal femoralgrowth plate has the potential forcausing genu varum. For example,infantile osteomyelitis with abscessformation can generate uneven sub-
sequent growth, with resultant de-formity. Another such disorder isphyseal growth disturbance sec-ondary to trauma or sepsis. The dis-tal femur is a relatively common siteof growth disturbance followingphyseal fracture. Physeal fracturesof the proximal tibia are much lesscommon. Management of physealgrowth disturbances is complex andis beyond the scope of this article.
Principles of Evaluationand Treatment
The following are a few principlesthat will help the orthopaedist in theevaluation and treatment of thechild with genu varum:
(1) Genu varum is physiologicuntil the age of 18 to 24 months, andtreatment is unnecessary.
(2) In a child with normal statureand findings compatible with physi-
ologic bowing, radiographic docu-mentation is unnecessary. Ifdocumentation of the condition isdesired, photographs are less expen-sive and just as valuable.
(3) If radiographs are deemednecessary, full-length standing films
of the entire lower limbs are requiredfor the evaluation of the mechanicalaxis and the site of deformity.
(4) Shortness of stature shouldsignal the likelihood that a constitu-tional disorder is the cause of genuvarum.
(5) Idiopathic tibia vara is themost common pathologic cause ofbowlegs in the child. Bracing may beeffective in the early stages, but thishas not been established by prospec-tive controlled clinical trials.
(6) Surgical correction of tibiavara can be guided by the principlethat reestablishing a normal me-chanical axis in the early stages willallow normal growth to occur. Inolder children, resumption of nor-mal growth cannot be assumed, and
measures to slow later tibial physealgrowth may also be needed.
(7) There are various types of in-ternal and external fixation, all ofwhich are satisfactory. The particu-lar type of fixation used for surgicaltreatment of tibia vara is less impor-tant than reestablishment of the me-chanical axis.
(8) Treatment of genu varum sec-ondary to constitutional disordersmust be tailored on an individual
basis.
Conclusion
Although genu varum is fairly com-mon in children, considerablechanges in evaluation and treat-ment approaches have occurredover the past decade. Further re-finements can be expected in thecoming years, perhaps including aclearer concept of the etiology oftibia vara, a better grasp of the roleof bracing in infantile tibia vara,and a more complete understand-ing of the effects of treatment (bothpositive and negative) in consti-tutional disorders such as achon-droplasia.
Journal of the American Academy of Orthopaedic Surgeons334
Genu Varum in Childr en
-
7/25/2019 Genu Varum en nios: Tratamiento y Diagnstico
10/10
References1. Staheli LT, Corbett M, Wyss C, et al:
Lower-extremity rotational problems inchildren: Normal values to guide man-agement. J Bone Joint Surg Am 1985;67:39-47.
2. Feldman MD, Schoenecker PL: Use of
the metaphyseal-diaphyseal angle inthe evaluation of bowed legs. J Bone
Joint Surg Am 1993;75:1602-1609.3. Heath CH, Staheli LT: Normal limits of
knee angle in white children: Genuvarum and genu valgum. J Pediatr Or-thop 1993;13:259-262.
4. Salenius P, Vankka E: The developmentof the tibiofemoral angle in children. JBone Joint Surg Am 1975;57:259-261.
5. Illingworth RS (ed): The Development ofthe Infant and Young Child: Normal and
Abnormal, 9th ed. Edinburgh: ChurchillLivingstone, 1987.
6. Langenskild A: Tibia vara: Osteochon-
drosis deformans tibiaeBlounts dis-ease. Clin Orthop 1981;158:77-82.7. Henderson RC, Kemp GJ, Hayes PRL:
Prevalence of late-onset tibia vara. J Pe-diatr Orthop 1993;13:255-258.
8. Wenger DR, Mickelson M, Maynard JA:The evolution and histopathology ofadolescent tibia vara. J Pediatr Orthop1984;4:78-88.
9. Cook SD, Lavernia CJ, Burke SW, et al: Abiomechanical analysis of the etiology oftibia vara.J Pediatr Orthop1983;3:449-454.
10. Carter JR, Leeson MC, Thompson GH,et al: Late-onset tibia vara: A histo-pathologic analysisA comparativeevaluation with infantile tibia vara andslipped capital femoral epiphysis. JPediatr Orthop 1988;8:187-195.
11. Kline SC, Bostrum M, Griffin PP:Femoral varus: An important compo-nent in late-onset Blounts disease. J Pe-diatr Orthop 1992;12:197-206.
12. Levine AM, Drennan JC: Physiologicalbowing and tibia vara: The metaphy-seal-diaphyseal angle in the measure-ment of bowleg deformities. J Bone JointSurg Am 1982;64:1158-1163.
13. Henderson RC, Lechner CT, DeMasiRA, et al: Variability in radiographicmeasurement of bowleg deformity inchildren. J Pediatr Orthop 1990;10:491-494.
14. Loder RT, Johnston CE II: Infantile tibia
vara. J Pediatr Orthop 1987;7:639-646.15. Schoenecker PL, Meade WC, Pierron
RL, et al: Blounts disease: A retrospec-tive review and recommendations fortreatment. J Pediatr Orthop 1985;5:181-186.
16. Greene WB: Infantile tibia vara. J BoneJoint Surg Am 1993;75:130-143.
17. Ferriter P, Shapiro F: Infantile tibiavara: Factors affecting outcome followingproximal tibial osteotomy. J Pediatr Or-thop 1987;7:1-7.
18. Beck CL, Burke SW, Roberts JM, et al:Physeal bridge resection in infantileBlount disease. J Pediatr Orthop 1987;7:161-163.
19. Siffert RS: Intraepiphyseal osteotomyfor progressive tibia vara: Case report
and rationale of management. J PediatrOrthop 1982;2:81-85.
20. Hofmann A, Jones RE, Herring JA:Blounts disease after skeletal maturity.
J Bone Joint Surg Am 1982;64:1004-1009.21. Henderson RC, Kemp GJ Jr, Greene WB:
Adolescent tibia vara: Alternatives foroperative treatment. J Bone Joint SurgAm 1992;74:342-350.
22. Evans GA, Arulanantham K, Gage JR:Primary hypophosphatemic rickets: Ef-fect of oral phosphate and vitamin D ongrowth and surgical treatment. J Bone
Joint Surg Am 1980;62:1130-1138.23. Oppenheim WL, Shayestehfar S,
Salusky IB: Tibial physeal changes inrenal osteodystrophy: Lateral Blountsdisease. J Pediatr Orthop 1992;12:774-779.
24. Olney BW, Cole WG, Menelaus MB:Three additional cases of focal fibrocar-tilaginous dysplasia causing tibia vara.
J Pediatr Orthop 1990;10:405-407.25. Bradish CF, Davies SJM, Malone M:
Tibia vara due to focal fibrocartilagi-nous dysplasia: The natural history. JBone Joint Surg Br 1988;70:106-108.
Vol 3, No 6, November/December 1995 335
Wern er C. Brooks, MD, and Richar d H . Gross, MD
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8245052&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8245052&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8245052&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8245052&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8245052&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8245052&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1112851&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1112851&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1112851&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1112851&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1112851&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7273529&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7273529&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7273529&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7273529&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7273529&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459022&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459022&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459022&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459022&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459022&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6693572&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6693572&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6693572&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6693572&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6693572&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6630488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6630488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6630488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6630488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6630488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3429646&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3429646&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3429646&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3429646&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8419383&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8419383&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8419383&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8419383&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3793900&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3793900&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3793900&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3793900&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3793900&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3793900&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3558798&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3558798&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3558798&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3558798&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3558798&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3558798&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7076838&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7076838&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7076838&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7076838&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7076838&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7076838&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7118963&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7118963&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7118963&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7118963&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1548260&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1548260&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1548260&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1548260&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1548260&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2355089&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2355089&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2355089&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2355089&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2355089&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3339040&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3339040&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3339040&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3339040&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3339040&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3339040&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3339040&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2355089&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1452749&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6253500&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1548260&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7118963&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7076838&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3558798&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3793900&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8419383&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988919&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3429646&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2358488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7130229&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1552023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3350954&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6630488&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6693572&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459022&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7273529&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1112851&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459023&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8245052&Dopt=rhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3968103&Dopt=r