Inmunoterapia en Carcinoma Urotelial Respuesta duradera · Linfoma no Hodkin Páncreas Hígado...
45
Inmunoterapia en Carcinoma Urotelial Respuesta duradera Dr. Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre. Prof. Asociado Univ. Complutense Madrid I + 12 Research Institute
Transcript of Inmunoterapia en Carcinoma Urotelial Respuesta duradera · Linfoma no Hodkin Páncreas Hígado...

Inmunoterapia en Carcinoma UrotelialRespuesta duradera
Dr. Daniel CastellanoOncología Médica. Unidad de Tumores Genito-UrinariosHospital Universitario 12 de Octubre.Prof. Asociado Univ. Complutense MadridI + 12 Research Institute

Incidencia estimada de cáncer de vejiga en España1
1. Galceran J et al. Clin Transl Oncol. 2017;19:799-825
Incidencia estimada de los tumores más frecuentes en España en el año 2015 (ambos sexos)
Estimación de nuevos casos (miles)
0 10000 20000 30000 40000 50000
Colorrecto
Próstata
Pulmón
Mama
Vejiga
Estómago
Linfoma no Hodkin
Páncreas
Hígado
Riñon
21,093
17,439 3,654

Mortalidad estimada en España para cáncer de vejiga1
1. Instituto de Salud Carlos III. Área de Epidemiología ambiental y Cáncer. Centro Nacional de Epidemiología. 2014.
Mortalidad estimada por tipo de tumor (10 tumores más frecuentes) en España para el año 2014
Estimación de nuevos casos (miles)
0 10000 20000 30000
pulmón
Colorrectal
Páncreas
Mama
Próstata
Estómago
Hígado
Vejiga
Leucemia
Riñón
4,795

Bellmunt et al. Ann Oncol 2014;25 Suppl 3:iii40–8
Patients with poor comorbid status or impaired renal
function ‘unfit’
Management of
metastatic disease
PS ≤2 plus
poor renal function
Carboplatin-based regimens or single-
agents: taxane, gemcitabine
Cisplatin-based
combination chemotherapy
(e.g. MVAC, GC, HDMVAC, PCG)
Clinical trial
Best supportive care
Progression <12 months
Second-line chemotherapy
1.Vinflunine
2.Taxane-based
3.Clinical trial
Progression >12 months
1. Platinum-based rechallenge
First line
• FIT → CISPLATIN-based combination
• UNFIT → CARBOPLATIN-based regimen
Subsequent lines
• Vinflunine
• Taxane-based
• Platinum rechallenge

Immunotherapy: Why Bladder
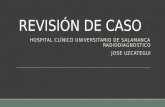
Figure: Somatic mutation frequencies observed in exomes from 3,083 tumor-normal pairs
Nature 499, 214–218 (11 July 2013)
Bladder tumors along with other malignancies such as lung and melanoma display a high number of somatic mutations rendering these tumors more immunogenic

Mutational Burden (13,8 mut./Mb)
So
ma
tic m
uta
tio
n b
urd
en
(mu
t/M
b)
1
5
10
50
100
200
300
500G
erm
cell
tum
our
Soft-t
issue s
arc
om
a
Pro
sta
te c
ancer
Thyro
id c
ancer
Bili
ary
ca
nce
r
Ovarian c
ancer
Re
nal cell
ca
rcin
om
a
Pancre
atic c
ancer
Bre
ast
carc
inom
a
Head a
nd n
eck
carc
inom
a
Glio
ma
Esophagogastr
ic
carc
inom
a
Endom
etr
ial cancer
No
n-s
mall-
cell
lung c
ancer
Co
lore
cta
l ca
nce
r
Mela
nom
a
Bla
dder
cancer
Alta carga mutacional en el cáncer de vejiga

Evolución de la terapia sistémica para cáncer urotelial
BLA, Biologics License Applicationhttp://www.accessdata.fda.gaov/scripts/cder/drugsatfda/index.cfm; http://www.ema.europa.eu/ema/1. Sternberg et al. Cancer 1989;64:2448–58; 2. McCaffrey et al. J Clin Oncol 1997;15:1853–73. von der Maase et al. J Clin Oncol 2005;23:4602–8; 4. Sternberg et al. J Clin Oncol 2001;19:2638–465. Vaughn et al. J Clin Oncol 2002;20:937–40; 6. Bellmunt et al. J Clin Oncol 2009;27:4454–617. Rosenberg et al. Lancet 2016;387:1909–20; 8. Balar et al. Lancet 2017;389:67–769. Sharma et al. Lancet Oncol 2017; doi: 10.1016/S1470-2045(17)30065-710. Bellmunt et al. N Engl J Med 2017; doi: 10.1056/NEJMoa161368311. Balar et al. J Clin Oncol 2017;35(suppl 6S):Abstract 284

FDA-Approved Checkpoint Inhibitors for UC
1. Atezolizumab [package insert]. July 2018. 2. Avelumab [package insert]. October 2017. 3. Durvalumab [package insert]. February 2018. 4. Nivolumab [package insert]. July 2018. 5. Pembrolizumab [package insert]. June 2018.
Agent Target Schedule FDA Approval Type by Setting
Post-Platinum Frontline Cisplatin Ineligible
Atezolizumab[1] PD-L1 Q3W Level 1 Accelerated
Avelumab[2] PD-L1 Q2W Accelerated --
Durvalumab[3] PD-L1 Q2W Accelerated --
Nivolumab[4] PD-1 Q4W Accelerated --
Pembrolizumab[5] PD-1 Q3W Level 1 Accelerated

IO therapy in Post-Platinum Urothelial Carcinoma

Atezolizumab. Evidencia estudio IMvigor210 Cohorte 2: Diseño del estudio1
1. Rosenberg et al. Lancet 2016;387:1909-20
Cohorte 2 (N=310)
tratados con platino
Atezolizumab
hasta pérdida de
beneficio clínico
UC localmente avanzado o
metastásico
Cohorte 1 (N=119)
1L no elegibles a
platino
Atezolizumab
hasta progresión
RECIST v1.1
OBJETIVOS CO-PRIMARIOS TRG (confirmada) por RECIST v1.1 por revisor central
TRG por RECIST modificado-immune por investigador

Atezolizumab. Con casi dos años de seguimiento la SG fue de 7,9 meses y el 37% de los pacientes estaban vivos al año1
1. Loriot et al. ESMO 2016
IMvigor210 Cohorte 2 (mediana de seguimiento de: 21,0 meses)
IC0/1
(n=210)
IC2/3
(n=100)
Todos los
pacientes
(N=310)
Mediana SG, meses
(IC 95%)
6.7
(5.4–8.0)
11.9
(9.0–NE)
7.9
(6.7–9.3)
Tasa SG 12-meses, %
(IC 95%)
31
(24–37)
50
(40–60)
37
(31–42)
Mediana SG = 7,9 meses
12 15 18 21963 240
100
SG
(%
)
80
60
40
20
0
Tiempo (meses)

Atezolizumab. Con casi dos años de seguimiento, la TRG fue del 16% y el 65% de los pacientes respondedores seguían en respuesta1
*Sin PE o fallecimiento. †Paciente fallecido (Patient is deceased (tiempo no incluido)
1. Loriot et al. ESMO 2016
IMvigor210 Cohorte 2 (mediana de seguimiento: 21,0 meses)
Todos
(N=310)
TRG
IC 95%
16%
(12, 20)
Tasa RC
IC 95%
6%
(4, 9)
Tiempo (meses)
RCRP
Primera RP/RCRespuesta mantenida*
Última dosisPE
Pacie
nte
sco
n R
C o
RP
co
mo
mejo
r
resp
uesta
12 14 18 22864 260 2 10 16 2420
††
††
††
La mediana de DoR aún no se había
alcanzado en todos los pacientes
El mantenimiento de la respuesta se
observó en 32 (65%) de 49 respondedores

Evidencia estudio IMvigor211; diseño del estudio1
ClinicalTrials.gov, NCT02302807. †Definido por el tiempo desde la quimioterapia previa <3 meses, ECOG PS >0 y hemoglobina <10 g/dL‡No se precisó confirmación de la respuesta para los objetivos secundarios de eficacia. Este análisis refiere respuestas exploratorias confirmadas
1. Powles et al. EACR-AACR-SIC Special Conference 2017
Factores de estratificación Objetivo primario Objetivos adicionales
Número de factores de riesgo† (0 vs 1/2/3) SG, valorada jerárquicamente en poblaciones
preespecificadas
RECIST v1.1 TRG, SLP y DoR‡, seguridad, PROs
(EORTC QLQ-C30)
Metástasis hepáticas (sí vs no)
Estado PD-L1 (0/1 vs 2/3)
Quimioterapia (vinflunina vs taxanos)
Chemotherapy(investigator’s choice)
▪ Vinflunine q3w
▪ Docetaxel q3w
▪ Paclitaxel q3w
Atezolizumab
1200 mg q3w
Criterios clave de eligibilidad*
CUm con progression durante o
después de quimioterapia
basada en platino
≤ 2 líineas previas de
tratamiento
Enfermedad medible por
RECIST v1.1
ECOG PS 0–1
Muestra evaluable para test de
PD-L1
Histología transicional como
componente primario
N=931
El protocolo no permite
cruzamientos
Progresión
por RECIST
v1.1
Pérdida de
beneficio
clínico
Seguimiento
de
supervivencia
R
1:1

NºPacientes en riesgo
20 4 8 10 12 14 16 18 20 22 246
Eventos/pacientes
Mediana SG(IC 95%)
Tasa SG a 12 m(IC 95%)
TECENTRIQ 72/116 11,1 m (8,6;15,5) 46% (37, 56)
Quimioterapia 88/118 10,6 m (8,4;12,2) 41% (32, 50)
HR= 0,87 (IC 95%: 0,63; 1,21)P=0,41
80
20
0
60
40
100
Superv
ivencia
glo
bal (%
)
Meses
TECENTRIQ®116 100 85 77 71 58 51 39 27 19 11 6 0
QUIMIOTERAPIA 118 100 91 82 71 61 47 32 24 15 9 5 1
ANÁLISIS SG: POBLACIÓN IC2/3
La población con CI 2/3 se analizó primero con una HR de la SG de 0,87 (IC 95%: 0,63; 1,21; mediana de SG de 11,1 meses vs. 10,6meses para atezoliumab y quimioterapia respectivamente). El valor p del test log-Rank estratificado fue de 0,41 y por lo tanto, los resultados se consideraron estadísticamente no significativos en esta población. 1.Ficha Técnica Tecentriq®
HR: Hazard Ratio; SG: Supervivencia global; IC: célula inmune1 Powles T et al. EAS 2017, IMvigor 211
Los resultados se consideraron estadísticamente no significativos en esta población. No se alcanzó el objetivo primario del estudio
IMvigor211: resultados1

Meses
Su
pe
rviv
en
cia
Glo
ba
l (
%)
80
20
0
20 4 8 10 12 14 16 18 20 22 246
60
40
100
HR= 0,85 (IC 95%: 0,73; 0,99)
P=0,038
IMvigor211: resultados población ITT1
*Los análisis primarios no alcanzaron el objetivo principal de SG en población IC 2/3 . En consecuencia los resultados de estos análisis se consideran
exploratoriosHR: Hazard Ratio; SG: Supervivencia global; IC: célula inmune; ITT: población por intención de tratar
1. Powles T et al. EAS 2017, IMvigor 211
Análisis SG: Población ITT
Eventos/
pacientes
Mediana SG
(IC 95%)
Tasa SG a 12 m
(IC 95%)
TECENTRIQ® 324/467 8,6 m (7,8;9,6) 39% (35, 44)
Quimioterapia 350/464 8,0 m (7,2;8,6) 32% (28, 37)
TECENTRIQ®467 405 327 280 245 201 177 138 90 59 34 13 1
Quimioterapia 464 397 330 268 219 175 140 99 60 42 17 7 1
Nº
Pacientes
en riesgo

*Los análisis primarios no alcanzaron el objetivo principal de SG en población IC 2/3 . En consecuencia los resultados de estos análisis se consideran exploratorios
DoR: duración de la respuesta; ITT: población por intención de tartar.
1. Powles T et al. EAS 2017, IMvigor 211
Respuesta poblacion ITT
Eventos/pacientes MDoR (IC 95%)
ATEZOLIZUMAB 23/62 21,7 m (13,0;21,7)
Quimioterapia 49/627,4 m
(6,1;10,3)
Pacientes
TECENTRIQ® 62 61 56 50 42 35 23 14 9 5 2 0
Quimioterapia 62 62 59 40 28 23 16 8 5 4 0 0
Re
sp
ue
sta
Ob
jeti
va
(%)
Meses
80
60
0
10 12 14 16 18 202 4 6 8 22
20
100
0
40
Atezolizumab ofrece respuestas duraderas en pacientes con TRO (RC, RP) alcanzando
una mediana de duración de la respuesta de 21,7 meses vs 7,4 con Quimioterapia
DoR en la población ITT
IMvigor211: Resultados población ITT1

KEYNOTE-045: Study Design
▪ International, randomized, open-label phase III study
▪ Primary endpoints: OS, PFS
▪ Secondary endpoints: ORR, DoR, safety
Bellmunt J, et al. N Engl J Med. 2017;376:1015-1026.
Adult patients with predominantly transitional cell UC of the renal pelvis, ureter, bladder, or urethra;
PD after 1-2 lines of platinum-based CT or recurrence < 12 mos
after perioperative platinum-based CT; ECOG PS 0-2
(N = 542)
Treatment continued for 2 yrs or until PD,
unacceptable toxicity, or withdrawal of
consent
Pembrolizumab 200 mg IV Q3W
(n = 270)
Paclitaxel 175 mg/m2 IV Q3W or Docetaxel 75 mg/m2 IV Q3W orVinflunine 320 mg/m2 IV Q3W
(n = 272)
Stratified by ECOG PS (0/1 vs 2), Hg (< 10 vs ≥ 10 g/dL), liver
mets (yes vs no), and time since last CT (< vs ≥ 3 mos)

Pembrolizumab
Chemotherapy
KEYNOTE-045: OS
270 194 147 116 98 67 23
272 171 109 73 58 35 13
44.4%30.3% 33.2%
19.7%
Median OS, Mos (95% CI)10.3 (8.0-12.3)
7.4 (6.3-8.3)
0 4 8 12 16 20 24 28 320
20
40
60
80O
S (%
)
Mos
100
Patients at Risk, n
de Wit R, et al. ESMO 2017. Abstract LBA37_PR.
Data cutoff: May 19, 2017
HR: 0.70 (0.57-0.86; P = .0003)

Pembrolizumab
Chemotherapy
Median PFS, Mos (95% CI)2.1 (2.0-2.2)3.3 (2.4-3.5)
KEYNOTE-045: PFS
270 86 61 44 39 24 6
272 93 39 19 12 7 2
PFS
(%
)
MosPatients at Risk, n
17.8%9.3% 15.3%
4.8%
0 4
60
80
8 12 16 20 24 280
20
40
100
de Wit R, et al. ESMO 2017. Abstract LBA37_PR.
Data cutoff: May 19, 2017
HR: 0.96 (0.79-1.16; P = .32)

KEYNOTE-045: ORR
de Wit R, et al. ESMO 2017. Abstract LBA37_PR.
21.1%
11.0%
PRCR
7.8%
13.3%
Pembrolizumab(n = 270)
Chemotherapy(n = 272)
2.9%
8.1%
OR
R (
%, 9
5%
CI)
All Patients
20.3%
6.7%
6.8%
13.5%
Pembrolizumab(n = 74)
Chemotherapy(n = 90)
2.2%
4.4%
OR
R (
%, 9
5%
CI)
PD-L1 Positive (CPS ≥ 10)
0
5
10
15
20
25
30
35
0
5
10
15
20
25
30
35

Post-Platinum Urothelial Carcinoma: ORR
CT: ~ 10%
1. Powles T, et al. Lancet. 2018;391:748-757. 2. Apolo AB, et al. J Clin Oncol. 2017;35:2117-2124. 3. Powles T, et al. JAMA Oncol. 2017;3:e172411. 4. Sharma P, et al. Lancet Oncol. 2017;18:312-322.5. Bellmunt J, et al. N Engl J Med. 2017;376:1015-1026.
Atezolizumab[1]
OR
R (
%, 9
5%
CI)
Data from separate studies. Not head-to-head comparisons.
13.4 18.2 17.8 19.6 21.10
10
20
30
40
50
60
70
Pembrolizumab[5]Nivolumab[4]Durvalumab[3]Avelumab[2]

Frontline Checkpoint Inhibition in Cisplatin Ineligible UC: Updates from Single-Arm Trials
Pembrolizumab (n = 370)KEYNOTE-52[1]
Atezolizumab (n = 119)IMvigor 210 Cohort 1[2]
Median follow up, mos 11.5 29
ORR, % 29 24
Median OS, mos 11.5 16.3
12 month OS, % 48 58
Pembrolizumab OS Atezolizumab OS100
80
60
40
20
00 4 8 12 16 20 24
MosPatients at Risk, n
370
28 32
283 223 173 147 86 38 11 11
OS
(%)
100
80
60
40
20
00 4 8 12 16 20 24
MosPatients at Risk, n
370
28 32
283 223 173 147 86 38 11 11O
S (%
)
36
1-yr OS: 58% (95% CI: 49-67)
2-yr OS: 41% (95% CI: 32-50)
Median OS: 16.3 mo (95% CI: 10.4-24.5)
1. Vuky J, et al. ASCO 2018. Abstract 4524. 2. Balar AV, et al. ASCO 2018. Abstract 4523.

IMvigor210 Cohort 1: study design
Primary endpoint
• Confirmed ORR: RECIST v1.1 (per central IRF)
Key secondary endpoints
• DOR, PFS, OS, safety
IRF, independent review facility. ClinicalTrials.gov ID: NCT02108652. aPD-L1 prospectively assessed by a central laboratory, with patients and investigators blindedbCockcroft-Gault formula
Balar et al. Lancet 2017;389:67–76
Cohort 2 (N=310):
Platinum-treated mUC
Atezolizumab 1,200mg IV q3w
until loss of clinical benefit
Cohort 1 (N=119):
1L cisplatin ineligible
Atezolizumab 1,200mg IV q3w
until RECIST v1.1 progression• Inoperable locally advanced or
metastatic urothelial carcinoma
• Predominantly UC histology
• Tumour tissue evaluable for
PD-L1 testinga

IMvigor210 Cohort 1: efficacyOverall survival (median and landmark 12-month OS)
Data cut-off: 4 July 2016
Balar et al. Lancet 2017;389:67–76
00
20
40
60
80
100
4 8 12
Time (months)
Overa
ll s
urv
ival (%
)
16 20 24
Subgroup Median OS (95% Cl) 12-month OS (95% Cl)
All (N=119) 15.9 months (10.4, NE) 57% (48–66)
IC0/1 (n=87) 19.1 months (9.8, NE) 59% (48–70)
IC2/3 (n=32) 12.3 months (6.0, NE) 52% (35–70)
Number at risk
All patients 310 265 203 176 146 126 110 99 91 79 70 23 2

Baseline 08/2014
PS 1
Back pain
PR 11/2014
PS 0PR 01/2015 CR 03/2015
Hospital 12 de Octubre: IMvigor 210 STUDY
MB: 62-year-old male with Stage IV TCC and extensive RP lymph node mts
after adjuvant GC, paclitaxel-carbo, vinflunine, gemcitabine alone and
anthracycline based-CT.
Atezolizumab 1.200mg q3w initiated on study on September 2014
(> 60 cycles)
Excellent tolerance
Adverse events: G1 flu-like syndrome, and G1-2 asthenia.

26 de Septiembre 2017

KEYNOTE-052



75-year-old male with upper tract UCC and bone, liver and LN mts after
nephroureterectomy + lymphadenectomy
Hospital 12 de Octubre: KEYNOTE-052
Pembrolizumab 200mg q3w initiated on study on September 2015
Baseline 09/2015
PS 2
Cis-inelegible
CR 09/2016
PS 0
24 cycles
Excellent
tolerance
Caso clínico 2


First-line Therapy for Metastatic UC: What We Know
▪ Chemotherapy is active in this space
▪ Cisplatin-eligible patients should get cisplatin-based chemotherapy
▪ FDA and EMA warn of decreased survival with first-line atezolizumab or pembrolizumab in cisplatin-ineligible patients with low PD-L1, as assessed by an appropriate companion diagnostic test
▪ FDA Alert about the PDL-1 low status had decreased survival compared to patients who received platinum-based chemotherapy. (5-18-2018)
‒ Access to such diagnostic tests is variable, limited at many institutions

Ensayos de Primera Línea en curso
IMvigor130 (NCT02807636)
• 1L cisplatin-ineligible, locally
advanced/metastatic• ECOG PS ≤2
N = 1200
Co-primary endpoints: PFS and OS
DANUBE (NCT02516241)
• 1L unresectable stage IV• Eligible / ineligible for
cisplatin-based chemotherapyN = 1004
Primary endpoint: OS
KEYNOTE-361 (NCT02853305)
• 1L unresectable or metastatic
• ECOG PS ≤2N = 990
Co-primary endpoints: PFS and OS
R
R
R
Atezolizumab
Platinum based chemo +
atezolizumab
Cisplatin + gemcitabine or
carboplatin + gemcitabine
Durvalumab + tremelimumab
Durvalumab
Cisplatin + gemcitabine orcarboplatin + gemcitabine
Pembrolizumab + cisplatin/gemcitabine or
Pembrolizumab + carboplatin/gemcitabine
Pembrolizumab
Cisplatin + gemcitabine orcarboplatin + gemcitabine

Ensayos de Primera Línea en curso
R
CHECKMATE 901 (NCT03036098)
• Metastatic urothelial cancer
• Unfit or fit patients
• No chemotherapy in metastatic setting
N = 897
• Metastatic urothelial cancer
• CR, PR, SD upon 4-6 platinum-based
chemotherapyN = 668
Primary endpoint: OS; secondary endpoints: PFS, ORR, DOR, Safety
R
Nivolumab
Nivolumab + chemotherapy
SOC Platinum-based chemotherapy
Avelumab
SOC: BSC
Primary endpoint: OS and PFS in unfit patients; secondary endpoints: OS in all patients, ORR, safety
JAVELIN (NCT002603432)
Estimated completion: 2020
SOC, standard of care

Cisplatin-Based Neoadjuvant CT
1. Dash A, et al. Cancer. 2008;113:2471-2477. 2. Tully CM, et al. ASCO GU 2014. Abstract 355. 3. Anari F, et al. Eur Urol Oncol. 2018;1:54-60. 4. Iyer G, et al. J Clin Oncol. 2018;36:1949-1956.5. Blick C, et al. Cancer. 2012;118:3920-3927. 6. Plimack ER, et al. J Clin Oncol. 2014;32:1895-1901.7. Choueiri TK, et al. J Clin Oncol. 2014;32:1889-1894.
CharacteristicGem/Cis[1]
(n = 42)Gem/Cis[2]
(n = 154)
DD Gem/Cis[3]
(n = 31)
DD Gem/Cis[4]
(n = 46)
AMVAC[5]
(n = 80)AMVAC[6]
(n = 40)DD MVAC[7]
(n = 39)
Study typeRetrospectiv
eRetrospectiv
eProspective Prospective
Retrospective
Prospective Prospective
Cycles, n 4 4 3 6 3-4 3 4
Wks, n 12 12 6 12 6-8 6 8
pCR (pT0), % 26 21 32 15 43 38 26
PR (< pT2), % 36 46 45 57 ~ 61 53 49
Median days from CT start to surgery
138 120 65 ~ 114+ 75 68 ~ 98
Grade 3/4 AEs, % NR NR 35 37 27 18 10
Progression free at 2 yrs, %
64 ~ 68 ~ 68 ~ 76 65 78 ~ 47
Alive at 2 yrs,* % 73 ~ 75 ~ 77 ~ 87 77 83 ≤ 80
*vs 58% with cystectomy alone.
40% to 60% have significant residual bladder cancer (≥ T2) after neoadjuvant CT

CharacteristicAtezolizumab
(n = 68)[2]
Eligibility criteria T2-T4a; N0 only
Cisplatin eligible, % 0
Received neoadjuvant CT, % 0
Duration of neoadjuvant checkpoint inhibition
2 cycles (6 wks)
Safe Yes
Pathological CR (pT0), % 29
Available biomarker data Yes
Neoadjuvant Checkpoint Inhibition in Bladder Cancer: Early Results of Phase II Trials-Atezo (ABACUS)
1. Necchi A, et al. ASCO 2018. Abstract 4507. 2. Powles T, et al. ASCO 2018. Abstract 4506.
Encouraging results; long-term outcomes needed before clinical use
pT0 Rates With CT:
Gem/Cis,15% to 32%
DD MVAC,26% to 43%

CharacteristicPembrolizumab
(n = 43)[1]
Eligibility criteria T2-T3b; N1 allowed
Cisplatin eligible, % 100
Received neoadjuvant CT, % 12
Duration of neoadjuvant checkpoint inhibition
3 cycles (9 wks)
Safe Yes
Pathological CR (pT0), % 40
Available biomarker data Yes
Neoadjuvant Checkpoint Inhibition in Bladder Cancer: Early Results of Phase II Trials-Pembro (PURE-01)
1. Necchi A, et al. ASCO 2018. Abstract 4507. 2. Powles T, et al. ASCO 2018. Abstract 4506.
Encouraging results; long-term outcomes needed before clinical use
pT0 Rates With CT:
Gem/Cis,15% to 32%
DD MVAC,26% to 43%

Summary: Urothelial Carcinoma▪ Options of treatment 2018
*Consider testing for PD-L1 using the appropriate companion diagnosticand limiting treatment to those who are PD-L1 positive
Neoadjuvant Preferred Alternate
Cisplatin eligibleGemcitabine/cisplatin or
DD MVACCheckpoint inhibitor on a clinical trial
Cisplatin ineligibleUpfront surgery,
then consider adjuvant trialCheckpoint inhibitor on a clinical trial
First-line Metastatic Preferred Alternate
Cisplatin eligibleGemcitabine/cisplatin
(standard dosing)DD MVAC
Cisplatin ineligible Gemcitabine/carboplatin Atezolizumab or pembrolizumab*

Algorithm for first line/second line treatment for metastatic UC from
July 2018 – why did it change
Atezolizumab
Pembrolizumab
Atezolizumab
Pembrolizumab
Clinical Trial(IO combinatios,fgfr inh, parp
inh, TKIs)
Modified, T. Powles, ESMO 2018

Bladder Cancer: Spectrum of Disease
Localized: ~ 95%
NMIBC: 70%CIS, Ta, T1
MIBC: 30%T2-T4
Urology
Metastatic: ~ 5%
RadiationOncology
MedicalOncology
The Future
-Pathologist
-Radiologist
-Biologist
-Palliative care Unit
- Pain Unit
- Internist

Backup

Multidisciplinary Collaborative Approach to Patients With Bladder Cancer
▪ Offers most balanced and objective understanding of available options
▪ Provides best chance for cure
▪ Catalyzes patient engagement
▪ Improves quality of care

Bladder Cancer: Spectrum of Disease
MedicalOncology
Localized: ~ 95% Metastatic: ~ 5%
NMIBC: 70%CIS, Ta, T1
MIBC: 30%T2-T4
Urology
The Past

Bladder Cancer: Spectrum of Disease
MedicalOncology
Localized: ~ 95%
NMIBC: 70%CIS, Ta, T1
MIBC: 30%T2-T4
Urology
Metastatic: ~ 5%
The Present

Bladder Cancer: Spectrum of Disease
Localized: ~ 95%
NMIBC: 70%CIS, Ta, T1
MIBC: 30%T2-T4
Urology
Metastatic: ~ 5%
RadiationOncology
MedicalOncology
The Present