Inmunoterapia en tratamiento de segunda línea y sucesivas en … · 2017-06-21 · Inmunoterapia...
42
Título de la dispositiva Inmunoterapia en tratamiento de segunda línea y sucesivas en cáncer renal avanzado José Luis Pérez Gracia Departamento de Oncología Clínica Universidad de Navarra
Transcript of Inmunoterapia en tratamiento de segunda línea y sucesivas en … · 2017-06-21 · Inmunoterapia...

Título de la dispositiva
Inmunoterapia en tratamiento de segunda línea
y sucesivas en cáncer renal avanzado
José Luis Pérez Gracia
Departamento de OncologíaClínica Universidadde Navarra

Inmunoterapia en tratamiento de segunda líneay sucesivas en cáncer renal avanzado
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones

Topalian, NEJM 2012

Motzer, JCO 2014

Motzer, JCO 2014

Motzer, JCO 2014

Motzer, JCO 2014

0.3 mg/kg 18.2 months
2 mg/kg 25.5 months
10 mg/kg 24.7 m
Motzer, JCO 2014
0.3 mg/kg 18.2 months
2 mg/kg 25.5 months
10 mg/kg 24.7 m

McDermott, JCO 2016
ORR: 15%IC0 (34%): 9%IC 1/2/3 (53%): 18%
Furhman 4 y sarcomatoide: 22%

Mediana spv. global: 28.9 m
McDermott, JCO 2016

McDermott, JCO 2016

Inmunoterapia en tratamiento de segunda líneay sucesivas en cáncer renal avanzado
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones

Advanced RCC withclear-cell
component
One or two prioranti-angiogenic
therapies
Progression within6 months
Advanced RCC withclear-cell
component
One or two prioranti-angiogenic
therapies
Progression within6 months
Nivolumab3 mg/kg intravenously
every 2 weeks
Nivolumab3 mg/kg intravenously
every 2 weeks
Ran
dom
ize
1:1
• Primaryendpoint: OS
• Key secondaryendpoint: ORR
• Primaryendpoint: OS
• Key secondaryendpoint: ORR
Advanced RCC withclear-cell
component
One or two prioranti-angiogenic
therapies
Progression within6 months
Advanced RCC withclear-cell
component
One or two prioranti-angiogenic
therapies
Progression within6 months
Everolimus10 mg orallyonce daily
Everolimus10 mg orallyonce daily
Ran
dom
ize
1:1
• Primaryendpoint: OS
• Key secondaryendpoint: ORR
• Primaryendpoint: OS
• Key secondaryendpoint: ORR
• 821 patients randomized from October 2012 through March 2014• Study halted July 2015 at preplanned interim analysis of OS
Motzer, NEJM 2015

Motzer, NEJM 2015

Motzer, NEJM 2015

Response characteristics
ORR, %
Nivolumab 25
Everolimus 5Odds ratio (95% CI),
5.98 (3.68–9.72)P < 0.0001
Indi
vidu
al re
spon
ders
Ongoing responseFirst responseOff treatment
NivolumabEverolimus On treatment
Odds ratio (95% CI),5.98 (3.68–9.72)
P < 0.0001
0 16 32 6448 80Time (Weeks)
96 112 128
Indi
vidu
al re
spon
ders

Motzer, NEJM 2015

¿Porqué sale positiva OS y no PFS?– Fenómeno habitual en inmunoterapia:
• Sipuleucel (Kantoff, NEJM 2010)• Nivolumab vs txt en CNMP no escamoso (Borghaei, NEJM 2015)• Pembrolizumab en CNMP (Herbst, Lancet 2016)
– Descrito con TKI: Intorsect (sorafenib vs temsirolimus: =SLP,mejor SPV para sorafenib) (Hutson JCO 2014)
– PFS es una variable subjetiva (respuesta)– Pseudoprogresión …
– ¿Diferencias biológicas de inmunoterapia?... PFS es “surrogate” de OS, no al revés
– Fenómeno habitual en inmunoterapia:• Sipuleucel (Kantoff, NEJM 2010)• Nivolumab vs txt en CNMP no escamoso (Borghaei, NEJM 2015)• Pembrolizumab en CNMP (Herbst, Lancet 2016)
– Descrito con TKI: Intorsect (sorafenib vs temsirolimus: =SLP,mejor SPV para sorafenib) (Hutson JCO 2014)
– PFS es una variable subjetiva (respuesta)– Pseudoprogresión …
– ¿Diferencias biológicas de inmunoterapia?... PFS es “surrogate” de OS, no al revés

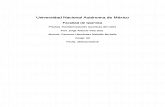
Landmark Overall Survival Analysis in PatientsTreated and Not Treated Beyond Progression
Ove
rall
Surv
ival
(Pro
babi
lity)
1.0
0.9
Median OS, months (95% CI)Treated beyond progression 28.1 (23.2–NE)Not treated beyond progression 15.0 (12.1–18.2)
HR (95% CI), 0.41 (0.29–0.57)Overall survival with nivolumab
Months
Ove
rall
Surv
ival
(Pro
babi
lity)
0.00 3 6 9 12 15 18 21 24 27 30 33
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Not treated beyond progression
Treated beyond progression
Escudier, ASCO 2016.

Tumor Burden Change Post-Progression• A total of 142 of 153 patients treated with nivolumab beyond progression had tumor measurements pre- and post-
progression– Of these 142 patients, approximately half had a reduction in tumor burden post-progression and 14%
(n = 20) had a ≥30% reduction in tumor burden post-progression
Best reduction in target lesions with nivolumab
*
50
25
Best
Red
uctio
n fro
m F
irst P
rogr
essi
on in
Targ
et L
esio
n (%
)
*
**
*
Reported as of June 2016.Asterisks represent responders before first progression. Square symbols represent % change truncated to 100%.nivo = nivolumab; q2w = every 2 weeks.Escudier B et al. Poster presentation at ASCO 2016. 4509.
Patients
* * *
* * *
* * *
*
****
0
-25
-50
-75
-100
Best
Red
uctio
n fro
m F
irst P
rogr
essi
on in
Targ
et L
esio
n (%
) * **
* ** * ****
□□□□
Escudier, ASCO 2016.

Tumor Burden Change Based on Best Overall Response
Complete/Partial Response
(n = 31)Stable Disease
(n = 51)Progressive Disease
(n = 70)
Cha
nge
From
Bas
elin
e (%
)
25
50
75
100
* *
*
25
50
75
100
25
50
75
100
Time Since Randomization (Weeks)Before Progression Patients Still on Treatment
**C
hang
e Fr
om B
asel
ine
(%)
-1000 12 24 36 48 60 72 84 96 108120
-75
-50
-25
0* *
*
-1000 12 24 36 48 60 72 84 96 108120
-75
-50
-25
0
-1000 12 24 36 48 60 72 84 96 108
-75
-50
-25
0
After Progression
Escudier, ASCO 2016.

Changes in serum interleukin-8 (IL-8) levels reflect andpredict response to anti-PD-1 treatment in melanoma
and non-small cell lung cancer patients
Sanmamed, Ann Oncol 2017

Changes in serum interleukin-8 (IL-8) levels reflect andpredict response to anti-PD-1 treatment in melanoma
and non-small cell lung cancer patients
Sanmamed, Ann Oncol 2017

Motzer, NEJM 2015

Motzer, NEJM 2015
25% 75%



Long-term Overall Survival (OS) WithNivolumab in Previously Treated Patients
With Advanced Renal Cell Carcinoma(aRCC) From Phase I and Phase II Studies
David F. McDermott,1 Robert J. Motzer,2 Michael B. Atkins,3 Elizabeth R. Plimack,4Mario Sznol,5 Saby George,6 Charles G. Drake,7 Brian Rini,8 Toni K. Choueiri,9 Timothy Kuzel,10
JeffreyA. Sosman,11 David C. Smith,12 Ulka Vaishampayan,13 John D. Powderly,14
Suzanne L. Topalian,7 Huanyu Zhao,15 Ian M. Waxman,15 Hans J. Hammers7
4507
David F. McDermott,1 Robert J. Motzer,2 Michael B. Atkins,3 Elizabeth R. Plimack,4Mario Sznol,5 Saby George,6 Charles G. Drake,7 Brian Rini,8 Toni K. Choueiri,9 Timothy Kuzel,10
JeffreyA. Sosman,11 David C. Smith,12 Ulka Vaishampayan,13 John D. Powderly,14
Suzanne L. Topalian,7 Huanyu Zhao,15 Ian M. Waxman,15 Hans J. Hammers7
1Beth Israel Deaconess Medical Center, Dana-Farber/Harvard Cancer Center, Boston, MA, USA; 2Memorial Sloan Kettering Cancer Center, NewYork, NY, USA; 3Georgetown-Lombardi Comprehensive Cancer Center, Washington, DC, USA; 4Fox Chase Cancer Center, Philadelphia, PA,USA; 5Yale University School of Medicine and Smilow Cancer Center, Yale–New Haven Hospital, New Haven, CT, USA; 6Roswell Park CancerInstitute, Buffalo, NY, USA; 7Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, MD, USA; 8Cleveland Clinic Taussig
Cancer Institute, Cleveland, OH, USA; 9Dana-Farber Cancer Institute/Brigham and Women’s Hospital, Boston, MA, USA; 10NorthwesternUniversity Feinberg School of Medicine, Chicago, IL, USA; 11Vanderbilt University Medical Center, Nashville, TN, USA; 12University of Michigan
Comprehensive Cancer Center, Ann Arbor, MI, USA; 13Karmanos Cancer Institute, Wayne State University, Detroit, MI, USA; 14CarolinaBioOncology Institute, Huntersville, NC, USA; 15Bristol-Myers Squibb, Princeton, NJ, USA
ASCO 2016- 1506ES16NP04829-01

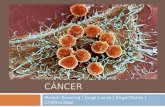
Overall Survival in Phase I and II StudiesStudy
Median OS, months(95% CI)
Phase IPhase II
22.4 (12.5–NE)23.4 (17.7–26.9)
1.00.90.80.70.60.50.40.30.20.10.0O
vera
llSu
rviv
al (P
roba
bilit
y)
38%
29%
34%
1.00.90.80.70.60.50.40.30.20.10.0
0
No. of patients at risk
6 12 18 24 30 36 42Months
48 54 60 66 72 78 84
Ove
rall
Surv
ival
(Pro
babi
lity)
• In phase I and II studies, minimum follow-up was 50.5 months and 49.2 months, respectively
NE, not estimable.
ASCO 2016
Phase I 34 28 24 18 14 13 12 12 11 8 6 6 2 1 0Phase II 167 142 113 93 80 65 58 51 47 2 0 0 0 0 0
ASCO 2016- 1506ES16NP04829-01
– Approximately one-third of patients are alive at 4 years (phase I and II)and 5 years (phase I)
– Long-term survival is achievable regardless of risk group,performance status, or best overall response (phase II)
McDermott, ASCO 2016

45
40
35
30
25
20
15
10
5
0
Emergence of Select Treatment-related AEs(Any Grade) Over Time in Phase II Study
Even
ts/p
atie
nts
at ri
sk(%
)45
40
35
30
25
20
15
10
5
0
Even
ts/p
atie
nts
at ri
sk(%
)
Overall ≤6 >6–≤12 >12–≤18 >18–≤24
Months
>24–≤30 >30–≤36 >36
No. of patients at risk 167 167 88 62 44 36 25 21
• Select treatment-relatedAEs included endocrine, gastrointestinal, hepatic, pulmonary, renal, and skin
ASCO 2016
ASCO 2016- 1506ES16NP04829-01 McDermott, ASCO 2016

Conclusions second linetreatment of RCC
“Official”• Nivolumab, cabozantinib and
lenvatinib are standard 2nd lineoptions for RCC– They all improve survival– Nivolumab does not improve PFS– Nivolumab less toxic
Personal• Nivolumab will be widely used in
second line therapy in RCC– Toxicity profile– New mechanism of action– Long term survivors (?)
• Lenvatinib + everolimus andcabozantinib will likely replaceother TKI and everolimus in 2ndor 3rd line, very specially in youngand fit patients
• Nivolumab, cabozantinib andlenvatinib are standard 2nd lineoptions for RCC– They all improve survival– Nivolumab does not improve PFS– Nivolumab less toxic
• Nivolumab will be widely used insecond line therapy in RCC– Toxicity profile– New mechanism of action– Long term survivors (?)
• Lenvatinib + everolimus andcabozantinib will likely replaceother TKI and everolimus in 2ndor 3rd line, very specially in youngand fit patients

Inmunoterapia en tratamiento de segunda líneay sucesivas en cáncer renal avanzado
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones

Efficacy and safety of nivolumab in patients with metastatic renalcell carcinoma (mRCC) and brain metastases: Preliminary resultsfrom the GETUG-AFU 26 (Nivoren) study.
55 pacientes con metástasis cerebrales de 588 incluidos (35 (67%) ,6(12%) and 11 (21%) with 1, 2 o > 2 metástasis).
10 pts (23%) con PS 2 y 25 (58%) PS 1.
16 pacientes (29%) tratados con > 2 líneas
67% (n = 37) sin tratamiento previo para mts SNC ,
En 44 pacientes evaluables se observaron 10 respuestas (23%)
21 pacientes (48%) presentaron progresión de la enfermedad
55 pacientes con metástasis cerebrales de 588 incluidos (35 (67%) ,6(12%) and 11 (21%) with 1, 2 o > 2 metástasis).
10 pts (23%) con PS 2 y 25 (58%) PS 1.
16 pacientes (29%) tratados con > 2 líneas
67% (n = 37) sin tratamiento previo para mts SNC ,
En 44 pacientes evaluables se observaron 10 respuestas (23%)
21 pacientes (48%) presentaron progresión de la enfermedad
Escudier, ASCO 2017, abstract 4563

Safety and efficacy of nivolumab for metastatic renal cell carcinoma(mRCC): Real world data from an Italian expanded access program (EAP).
389 pts median age was 65 years (range, 34-85)
70 (18%) aged ≥ 75 yrs. Pts had a clear-cell RCC in 92% of cases, bonemetastases in 50% and brain metastases in 8%, and received more thanone previous line in 79% of cases.
Median number of doses received was 10 (1-31). 82 (21%) pts treated beyondprogression.
18 pts (5%) discontinued treatment due to AE.
Best overall response rate was 17% (1 CR, 66 PR). SD: 31%
6-month and 9-month survival rates were 83% and 77%, respectively.Response and survival rates were comparable regardless age,presence of brain or bone metastases and number of prior therapies.
Conclusions: This EAP represents the most extensive reported real-worldexperience with nivolumab in pre-treated RCC pts. These first data seemto confirm efficacy and safety data of the pivotal trial in a real worldsetting.
389 pts median age was 65 years (range, 34-85)
70 (18%) aged ≥ 75 yrs. Pts had a clear-cell RCC in 92% of cases, bonemetastases in 50% and brain metastases in 8%, and received more thanone previous line in 79% of cases.
Median number of doses received was 10 (1-31). 82 (21%) pts treated beyondprogression.
18 pts (5%) discontinued treatment due to AE.
Best overall response rate was 17% (1 CR, 66 PR). SD: 31%
6-month and 9-month survival rates were 83% and 77%, respectively.Response and survival rates were comparable regardless age,presence of brain or bone metastases and number of prior therapies.
Conclusions: This EAP represents the most extensive reported real-worldexperience with nivolumab in pre-treated RCC pts. These first data seemto confirm efficacy and safety data of the pivotal trial in a real worldsetting.
De Giorgi, ASCO 2017, abstract 4577

Inmunoterapia en tratamiento de segunda líneay sucesivas en cáncer renal avanzado
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones
• Bloqueo PD-1/PDL1
• Fases II
• Fase III
• Estudios poblacionales
• Combinaciones

2-to-1 Format1 Flexible range of motion in Fabs1,2
CEA-TCB is the first T-cell bispecific antibody with a novel2-to-1 format, optimized for efficacy and safety
• Binds simultaneously with 1 arm to CD3 on T cells and with 2 arms to CEA on tumor cells• Flexible 2-to-1 format enables high-avidity binding and selective killing of high CEA-expressing tumor cells• Longer half-life compared with other TCB formats• Silent Fc results in reduced risk of FcγR-related cytokine release/IRRs
Fab, fragment antigen-binding region; IRR, infusion-related reaction. 1. Bacac M, et al. Clin Cancer Res. 2016;22:3286-3296; 2. Roche. Data on file.
35

Untargeted TCB CEA TCBIntravital two-photon imaging of anti-tumor activity
Combination Strategies – Enhancing Direct T cell Killing ofTumor Cells: T cell Bispecific Antibodies (TCBs)
Significantly higher number of T cells and high apoptotic tumor fractionalready 24 h after single CEA TCB treatment
LS174T-RFP (red)/hPBMCs co-grafting (5:1) for 4 days;T cells labeled with CFSE (green); imaging 1 day after therapyBacac, et al. ITOC 2014
T Cells:Tumor Cells:

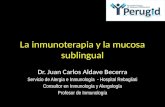
CEA-TCB + atezolizumab demonstrated promising clinical activityin 3L+ patients with MSS mCRC
Study 2: CEA-TCB + atezolizumab (n = 11, 80 and 160 mg of CEA-TCB)
Cha
nge
in ta
rget
lesi
ons
from
bas
elin
e, %
p
*p*
p
-50
0
50
100 *p
WithdrawalProgressionOngoingFirst new lesion
a
160 mg80 mg
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Data reported by investigators, cutoff: March 3, 2017. a Patient had the confirmatory CT scan on March 23, 2017.
38
Presented by: Dr. Josep Tabernero,Phase I Studies of CEA-TCB in mCRC. http://tago.ca/BfO
Weeks after treatment start
Cha
nge
in ta
rget
lesi
ons
from
bas
elin
e, %
p
*p*
p
-50
0
50
100 *p
WithdrawalProgressionOngoingFirst new lesion
a
160 mg80 mg
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24

Tumor targetanti-CEA or anti-FAP
Tumor-targeted immune cell growth factorEngineered Immunoglobulin-cytokine fusion
protein• CEA (Carcinoembryonic Antigen)
= adenocarcinoma cell antigen• FAP (Fibroblast Activation Protein α )
= cancer associated fibroblast/stroma cell antigen• High affinity binding for tumor targeting
pMAffinity
IL2vcytokine
• IL2v = IL-2 variant, IL-15 like cytokinePromoting immune effector cells (CD8 T & NKcells) over suppressor cells (Tregs &Macrophages)
Immunomodulator designed for combination with cytolysis-triggering moleculessuch as ADCC-mAbs, T-Cell bispecific mAbs and anti-PD1/PD-L1.
nM
Affinity
• Inert Fc-partImproved PK & Safety over aldesleukin

Obinutuzumab pre-treatmentTiming differs based on development of ADAs

CONCLUSIONES• La inmunoterapia es uno de los pilares del
tratamiento del cáncer renal– Nivolumab aprobado en cáncer renal avanzado
previamente tratado– Varios estudios en marcha en primera línea
• Desarrollo futuro– Biomarcadores– Nuevas combinaciones– Fases tempranas de la enfermedad
• La inmunoterapia es uno de los pilares deltratamiento del cáncer renal– Nivolumab aprobado en cáncer renal avanzado
previamente tratado– Varios estudios en marcha en primera línea
• Desarrollo futuro– Biomarcadores– Nuevas combinaciones– Fases tempranas de la enfermedad

Muchas gracias por vuestra atención
José Luis Pérez Gracia
Departamento de OncologíaClínica Universidad
de Navarra