INSUFICIENCIA RENAL EN EL TRASPLANTE CARDIACOsctransplant.org/sct2011/doc/presCurso/Manito.pdf ·...
23
INSUFICIENCIA RENAL EN EL TRASPLANTE CARDIACO Dr. Nicol Dr. Nicol á á s Manito s Manito Unidad de Insuficiencia Cardiaca y Trasplante Unidad de Insuficiencia Cardiaca y Trasplante Cardiaco Cardiaco Hospital Universitario de Bellvitge Hospital Universitario de Bellvitge SOCIETAT CATALANA DE TRASPLANTAMENT 2011
Transcript of INSUFICIENCIA RENAL EN EL TRASPLANTE CARDIACOsctransplant.org/sct2011/doc/presCurso/Manito.pdf ·...

INSUFICIENCIA RENAL EN EL TRASPLANTE CARDIACO
Dr. NicolDr. Nicoláás Manitos ManitoUnidad de Insuficiencia Cardiaca y Trasplante Unidad de Insuficiencia Cardiaca y Trasplante
CardiacoCardiacoHospital Universitario de BellvitgeHospital Universitario de Bellvitge
SOCIETAT CATALANA DE
TRASPLANTAMENT 2011

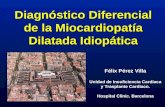
ADULT HEART TRANSPLANTATION Kaplan-Meier Survival by Era
(Transplants: 1/1982 – 6/2008)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
1982-1991 (N=18,236)
1992-2001 (N=34,422)
2002-6/2008 (N=18,661)
All comparisons are significant at p < 0.0001
Surv
ival
(%
)
2010ISHLT
J Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141
HALF-LIFE 1982-1991: 8.3 years; 1992-2001: 10.4 years; 2002-6/2008: NA

>> FunciFuncióón renal pre n renal pre -- TCTC
>> SituaciSituacióón hemodinn hemodináámica pre mica pre -- TCTC
>> CirculaciCirculacióón extracorpn extracorpóórea rea -- Isquemia del Isquemia del injerto en trasplante cardinjerto en trasplante cardííacoaco
>> Uso de fUso de fáármacos nefrotrmacos nefrotóóxicosxicos
>> Protocolos de inmunosupresiProtocolos de inmunosupresióón : n : Nefrotoxicidad por ICN aguda y crNefrotoxicidad por ICN aguda y cróónicanica
INSUFICIENCIA RENAL Y TRASPLANTE CARDIACO (TC)

Caso clínico : Insuficiencia renal+ Polineuropatía en trasplante cardíaco
• Hombre de 67 años
• Trasplante Cardíaco (TC) el 16/12 /2003 por miocardiopatía isquémica.
• Diabetes Mellitus ID. Vasculopatía periférica.
• Bypass Ao-bifemoral post-TC. Amputación 1º dedo pie I.
• Retinopatía diabética.
• Febrero-04 : Coronariografía : Normal . FE: 65 %
• Ingreso Agosto-05 para estudio funcion renal:
• Filtrado Glomerular (FG) isotópico: 50 ml/min/1,73 m2
• Flujo Plasmático Renal (FPR): 292 ml/min/1,73 m2
• Orina 24h: No Proteinuria
• Ecografía Abdominal : Normal
*

6-7-05 29-08-05 08-09-05 15-09-05
Creatinina 166 148 127 128
Urea 16 16 8 11.7
Filtrado Glomerular
39 44 53 53
Trigliceridos
Colesterol 3.9
Glucosa 5.2 5.4 5.5 4.3
Hb 11.5 11 10.8 10.4
Hto 36.5 33 32.2 31.2
Leucos 6450 5560 4950 4940
Plaquetas 238000 220000 221000 240000
Pre- Everolimus Post- Everolimus (23/8/05)
EVOLUCIÓN LABORATORIO TRAS CONVERSIÓN A ISP

06-07-05 25-08-05 29-08-05 8-09-05 15-09-05
Ciclosporina 110 79 38
MMF 1.7 1.7 1.2 2.5 2.6
Everolimus 4,1 5,4 5,5 6,6
Sandimmun 150 mg/24h 100 mg/24h 50 mg/24h
Cellcept 1000 mg/24h 200 mg/24h = =
Dacortin 2,5 mg/24 h 5 mg/24 h = =
Certican 1,5 mg /24 h 2,25 mg/24 h =
Post- Everolimus (23/8/05)Pre- Everolimus
EVOLUCIÓN NIVELES Y DOSIS DE FÁRMACOS INMUNOSUPRESORES TRAS CONVERSIÓN A ISP

CONVERSIÓN A EVEROLIMUS
ml/m
in/1
,73/
m2
EVOLUCIÓN FILTRADO GLOMERULAR DURANTE TODO EL SEGUIMIENTO POSTRASPLANTE

POST-HEART TRANSPLANT MORBIDITY FOR ADULTSCumulative Prevalence in Survivors at 1, 5 and 10 Years Post-Transplant (Follow-
ups: April 1994 - June 2009)
Outcome Within 1 Year
Total N with known
response
Within 5 Years
Total N with known
response
Within 10 Years
Total N with
known response
Hypertension 73.2% (N = 24,229) 93.1% (N = 10,485) 97.4% (N = 2,238)
Renal Dysfunction 26.8% (N = 25,254) 31.1% (N = 12,146) 36.8% (N = 3,681)
Abnormal Creatinine < 2.5 mg/dl 18.1% 21.0% 24.3% Creatinine > 2.5 mg/dl 7.0% 7.3% 6.2% Chronic Dialysis 1.5% 2.3% 4.8% Renal Transplant 0.3% 0.5% 1.5%
Hyperlipidemia 58.1% (N = 25,572) 87.8% (N = 11,800) 93.3% (N = 2,659)
Diabetes 27.4% (N = 25,292) 36.6% (N = 11,154) 38.5% (N = 2,401)
Cardiac Allograft Vasculopathy 7.8% (N = 22,853) 31.0% (N = 8,197) 51.8% (N = 1,830)
2010ISHLT
J Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141

LA INSUFICIENCIA RENAL EN EL TX NO-RENAL
Ojo et al . N Engl J Med 2003;10:931.
En 69.321pacientes receptores de un trasplante no-renal, la DRC se asoció a un
incremento de mortalidad por un factor >4 (RR 4.55; IC 4.38-4.74)

� De los pacientes con DRC , en el momento del diagnóstico:
- La Creatinina media fue de 2.2 (0.6) mg/dl
- El 83.5% presentaban toxicidad renal por ICN por diagnóstico
clínico analítico. En ningún caso por biopsia renal.
- Tiempo medio post Tx hasta Dx fue de 3 años 4 m.
� El 46,2% de los pacientes presentaban Disfunción Renal
Crónica (DRC) definida como: Creatinina sérica ≥ 2 mg/dl y/o
Aclaramiento de Creatinina ≤ 50 ml/min. Fw medio: 7 años
ESTUDIO ICEBERG EN TRASPLANTE CARDIACO
Arizón JM et al . ISHLT. Boston. 2008 .

Distribución de la función renal según niveles de MDRD y creatinina (mg/dl) en consulta
4,8%1,5%
42,6%
51,1%
>=60 30-59 15-29 <15
n = 399
CAPRI : ESTUDIO PARA EVALUAR PREVALENCIA DE INSUFICIENCIA
RENAL EN PACIENTES TRASPLANTADOS CARDÍACOS EN ESPAÑA
38%
62%
≥1,2 mg/dl<1,2 mg/dl
n = 416
Crespo-Leiro MG et al. Clin Transplant. 2010;24:88-93. Delgado JF et al. Clin Transplant. 2010 ;24:194-200

FREEDOM FROM SEVERE RENAL DYSFUNCTION BY ERA*For Adult Heart Recipients (Transplants: April 1994-June 2008)
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10
Years
Freedom from Severe Renal Dysfunction 4/1994-2000 (N = 11,180)
Freedom from Severe Renal Dysfunction 2001-6/2008 (N = 12,421)
* Severe renal dysfunction = Creatinine > 2.5 mg/dl, dialysis or renal transplant
% F
reed
om
fro
m S
ever
e R
enal
Dys
fucn
tio
n
p < 0.0001
2010ISHLT
J Heart Lung Transplant. 2010 Oct; 29 (10): 1083-1141

REGÍMENES ALTERNATIVOS DE INMUNOSUPRESIÓN
1. Minimización de los ICN– Con bajas dosis de ICN incorporando MMF / MPS.
2. Retirada de los ICN– Sin ICN: MMF/MPS + Everolimus/Sirolimus
3. Pacientes de novo sin ICN
INSUFICIENCIA RENAL Y TRASPLANTE CARDIACO (TC)

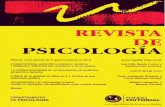
A B
NEFROTOXICIDAD CRÓNICA POR INHIBIDORES DE LA CALCINEURINA
Imagen A: Hialinosis medial en arteriolas aferentes renales –flechas-
(PAS, x400).
Imagen B: Fibrosis intersticial y atrofia tubular parcheada o en bandas – área entre flechas-
(Tricrómico de Masson, x100).

Resultados de la función renal
Autor GT (n) / GC (n)
Tiempo post-TC Criterio IR Inmunosupresión FW medio GT vs GC P
Angermann 109/52 > 6 meses CrS ≥ 1,7 mg/dlCambio de AZA a
MMF8 meses ↓ CrS 11% vs ↓CrS 4% 0,001
Baryalei 14/10 > 3 meses CrS ≥ 1,7 mg/dlCambio de AZA a
MMF177 días ↓ CrS 29% vs ↓ CrS 4% 0,02
Teodoriya 30/- > 17 meses CrS ≥ 1,7 mg/dlCambio de AZA a
MMF26 meses ↓ CrS 17,5% en GT 0,01
Arizon del
Prado31/- > 3 meses CrS ≥ 1,4 mg/dl
Cambio de AZA a
MMFND ↓ CrS 10,7% en GT 0,01
Aleksic 12/- > 111días CrS ≥ 2 mg/dlCambio de AZA a
MMF184 ↓ CrS 24% vs basal 0,004
Trosch 12/- > 4 años > 2'5 mg/ dlCambio de AZA a
SRL3 / 6 meses
3m: ↑ FG 34%
6 m: FG igual al basal
3 m:
0,003
Potter 16/- 142 meses ↓ FG ≥ 25% Cambio AZA/MMF a
SRL12 meses ↓ FG 11,3% vs basal 0,02
ESTUDIOS QUE APLICAN ESTRATEGIAS DE MINIMIZACIÓN
DE LOS ICN EN TC

ESTUDIO COLABORATIVO ESPAÑOL SOBRE LA
NEFROTOXICIDAD POR INHIBIDORES DE LA CALCINEURINA
CsA dosis bajas + MMF vs CsA + Aza
Rabago G et al. J Heart Lung Transplant 2001; 20: 193.

ESTUDIO COLABORATIVO ESPAÑOL SOBRE LA
NEFROTOXICIDAD POR INHIBIDORES DE LA CALCINEURINAACLARAMIENTO DE CREATININA (ml/min) - FORMULA DE COCKROFT-GAULT.
Rabago G et al. J Heart Lung Transplant 2001; 20: 193.

A c la ra m ie n to d e c re a t in in a
(m l/m in )
5 0 ,84 8 ,6
4 6 ,5
4 2 ,6
4 5 ,9 4 6
3 6 ,9 3 7 ,3 3 6 ,3
2 2 ,4
2 6 ,9
2 2 ,8
3 94 0 ,4
3 7 ,9
1 0
1 5
2 0
2 5
3 0
3 5
4 0
4 5
5 0
5 5
B A S A L M E S 6 M E S 1 2
G ru p o 1 G ru p o 2G ru p o 3 G ru p o 4G lo b a l
Grupo 1: 0 > creatinina < 1,8 Grupo 2: 1,8 > creatinina < 2,0
Grupo 3: 2,0 > creatinina < 2,7 Grupo 4: creatinina > 2,7
USO DEL SIROLIMUS EN LA INSUFICIENCIA RENAL DEL TRASPLANTE CARDÍACO
Subanálisis del Registro Multicéntrico Español (Estudio RAPACOR)

Creatinine clearance (ml/min)
35,537,9
41,8
40,8
43,5 44,440,3
41,4
42,3
40,6
0,0
10,0
20,0
30,0
40,0
50,0
Baseline Month 1 Month 3 Month 6 Month 12
CNI withdrawal before month 3 CNI continuation at month 3
USO DEL SIROLIMUS EN LA INSUFICIENCIA RENAL DEL TRASPLANTE CARDÍACO
Subanálisis del Registro Multicéntrico Español (Estudio RAPACOR)
Delgado JF, et al. Transplant Proc. 2009 ;41:3835-7.

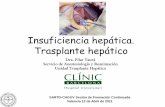
EVERODATA Renal function – subgroup with conversion due to nephrotoxicity
Mean serum creatinine levels
(mg/dl )
Mean glomerular filtration
rate (MDRD; ml/min/1,73/m2)
2.24
2.09
1.932 2.02 2.08
1.97 1.99 2.02 2.04
1.5
1.6
1.7
1.8
1.9
2
2.1
2.2
2.3
2.4
2.5
Pre-
conversion
Day 7Day 14 1 m 2 m 3 m 4 m 6 m 9 m 12 m
34.937.6
41.640.1 40.4 40.1 40.9 40.9 41.2 40.4
30
32
34
36
38
40
42
44
46
48
50
Pre-
conversion
Day 7Day 14 1 m 2 m 3 m 4 m 6 m 9 m 12 m
P<0.001 P=0.049
P < 0.001P < 0.001

Glomerular
filtration rate (ml/min/1,73/m2 )
Calcineurin Inhibitors
Total NO YES
baseline
≥≥≥≥ 50 4 (4,4%) 87 (95,6%) 91
40 - 49 3 (6,1%) 46 (93,9%) 49
30 - 39 1 (2,2%) 44 (97,8%) 45
≤≤≤≤ 29 4 (11,8%) 30 (88,2%) 34
month 12 (p<0,001)
≥≥≥≥ 50 17 (22,7%) 58 (77,3%) 75
40 - 49 12 (27,3%) 32 (72,7%) 44
30 - 39 12 (31,6%) 26 (68,4%) 38
≤≤≤≤ 29 20 (69,0%) 9 (31,0%) 29
GFR Analytical values in patients with o without CNISubgroup nephrotoxicity
EVERODATA

Gonzalez Vilchez F et al. J Heart Lung Transplant. 2008;27:1135-41.
USO DE ISP EN PACIENTES CON TRASPLANTE CARDIACO DE NOVO E INSUFICIENCIA RENAL
N = 20 ( 14 Sirolimus, 6 Everolimus) + MMF + Corticoides. Inducción en 9 p (45%) con Daclizumab/ Basiliximab
28±±±±17
67±±±±136 64±±±±2466±±±±36
• 55% Rechazo Agudo (76% disfunción vent)
• 4 Éxitus ( 2 RA)
• 50% de abandono del IPS:
- RA
- Derrame pleur/peric
- Herida Q
- Edemas EEII

CONCLUSIONES
• La nefrotoxicidad por ICN es una patología frecuente y precoz y se asocia a un mal pronóstico
• Existen diversas estrategias en el manejo de la inmunosupresión que conllevan la minimización o la retirada de los ICN.
• La evolución de la función renal según grupos de gravedad de la misma y del uso de los ICN, apoyan una introducción más precoz de los ISP y menos tiempo de uso concomitante con los ICN.