Lógica DIfusa Salud Enfermedad y Malestar

of 34
Transcript of Lógica DIfusa Salud Enfermedad y Malestar
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
1/34
Journal of Medicine and Philosophy 0360-5310/00/2505-0605$15.002000, Vol. 25, No. 5, pp. 605–638 © Swets & Zeitlinger
Fuzzy Health, Illness, and Disease
Kazem Sadegh-ZadehUniversity of Münster, Germany
ABSTRACT
The notions of health, illness, and disease are fuzzy-theoretically analyzed. They presentthemselves as non-Aristotelian concepts violating basic principles of classical logic. Arecursive scheme for defining the controversial notion of disease is proposed that alsosupports a concept of fuzzy disease. A sketch is given of the prototype resemblance theoryof disease.
Key words: prototype resemblance theory of disease, deontic constructs, disease, fuzzydisease, fuzzy health, fuzzy illness, health, illness, logic of medicine, Meinongian objects,nosology, patienthood
All humans are likely to find good reasons for holding angina or sarcomato be disease states, because they cause pain and circumscription of ourgoals, whether or not they have a positive or negative bearing on thesurvival of our species (Engelhardt, 1976, pp. 265f).
I. INTRODUCTION
In the last quarter of the 20th century we have been witnessing an intense
discussion on the nature of health, illness, and disease and on the meaningof these three basic notions of medicine.1 The discussion seems to haveended up in a blind alley, however. The harvest we have received thus farmay be summarized by a few labels: normativism, descriptivism, naïvenormalism, fictionalism, metaphorism, and philistinism.
Normativism says that the classification of certain groups of phenomenaas illnesses or diseases is based on value judgments (Engelhardt, 1975;1976; Margolis, 1969;1976). The concept of disease is not merely descrip-tive, but normative. It says what ought not to be (Engelhardt, 1975, p.127).
Correspondence: Kazem Sadegh-Zadeh, University of Münster Medical Institutions, In-stitute for Theory and History of Medicine, Waldeyer St. 27, 48149 Münster, Germany.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
2/34
KAZEM SADEGH-ZADEH606
Descriptivism or naturalism holds the opposite view. Disease is statisti-cally species-subnormal biological body function, and health is the ab-
sence of disease. The classification of human states as healthy or diseasedis an objective matter, to be read off the biological facts of nature withoutneed of value judgments (Boorse, 1997, p. 4).
According to naïve normalism, prevailing in medical schools and text-books, health is normality and diseases are abnormalities. What normalityis remains unclear.
The fictionalism of Franco-German origin says that “Disease is a genu-ine fiction” (Koch, 1920, pp. 130-131), for “there are no diseases, there areonly sick people” (Armand Trousseau, 1801-1867).
Thomas Szasz’ metaphorism, confined to psychiatry only, regards con-cepts of mental illness as mere myths and metaphors (1960; 1970). Mentalillness does not exist.
Philistinism, proudly argued and represented by Germund Hesslow(“GH, a philistine,” 1993, p. 2), holds that the three notions of health,illness and disease are superfluous in medicine and irrelevant to cliniciansand medical scientists (p. 3). For “there is no biomedical theory in whichdisease appears as a theoretical entity and there are no laws or generaliza-
tions linking disease to other important variables” (p. 5).Something omitted in the controversial debate above is the logical anal-ysis of the three notions mentioned. It is this omission that has led thediscourse to a dead end. In the present paper, a logical analysis of thesethree notions is undertaken that reveals a misconception underlying al-most all past philosophy on health, illness, and disease. The misconcep-tion may be described as follows. First, it is commonly assumed that theconcepts of health, illness, and disease are amenable to classical, bivalentmodes of reasoning of the Aristotelian type, based on the principles of
excluded middle and non-contradiction. According to this assumption:• an individual is healthy or she is not healthy, but not both at the same
time;• an individual is ill or she is not ill, but not both at the same time;• an individual has a disease or she does not have it, but not both at the
same time.
According to a second, also widespread assumption:• health and disease are opposites in that they are dual and mutually
exclusive attributes. It is said that health is the absence of disease andvice versa.
In this paper, I will demonstrate that the assumptions above are not true.First, the concepts of health, illness, and disease are not amenable to
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
3/34
FUZZY HEALTH, ILLNESS, AND DISEASE 607
classical logic. It may well be that a person is healthy and not healthy atthe same time; that she is ill and not ill at the same time, and that she has a
disease and does not have it at the same time. And second, health anddisease are not dual and mutually exclusive. It may well be that a person ishealthy and has a disease nonetheless, or that she is not healthy withouthaving any disease.
That means that health, illness, and disease are non-classical attributesviolating both bivalence and non-contradiction and, as such, they call for aconceptual framework that takes account of this non-Aristotelian circum-stance. In what follows, a fuzzy-theoretic approach is taken to provide aconceptual framework of just that virtue. In the next section, some prelim-inaries are presented to prepare the intended fuzzy-theoretic approach. Anovel theory of health, illness, and disease will then follow. It cannot, andwill not, be anticipated here. The core idea it rests upon is the view thathealth is a matter of degree, illness is a matter of degree, and disease is amatter of degree. They can, therefore, not be dealt with appropriately byAristotelian YES or NO principles. They are subject to the principle of graduality to which I now proceed.
II. FUZZY-THEORETIC TERMINOLOGY2
I will prefer the extensional mode of inquiry to the intensional one. Thatmeans that instead of considering an attribute itself I will consider the set of objects which bear that attribute. For example, I will talk about ‘the setof healthy people’ instead of talking about ‘health’. Whatever else health,illness, and disease may be, it is common belief that their bearers form setswith clear-cut boundaries (see, e.g., Feinstein, 1976, pp. 156-209). I will
abandon this received paradigm and will reconstruct them as fuzzy setsinstead.3
A fuzzy set is a collection of objects with grades of membership (Zadeh,1965a; 1965b). It does not have sharp boundaries between members andnon-members. For example, given two individuals, one of them may be young to some degree, whereas the other may be young to a lesser degreethan the former. Thus, these two individuals are to different degrees mem-bers of the same set of young people. The membership degrees of the setsmoothly decrease in the direction of zero; i.e., non-membership. The set
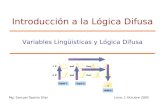
of young people is thus fuzzy. There is no dividing line between this setand the set of non-young people. Each of the following terms also denotesa fuzzy set: beautiful woman, tree, bush, big orange, much larger than 5,healthy, ill, diseased (see Figure 1). An individual who is young to a
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
4/34
KAZEM SADEGH-ZADEH608
particular extent, is not young to another particular extent, though thelatter may amount to zero. The same applies to individuals who are mem-bers of the sets of healthy, ill, or diseased people. For instance, a personwho is healthy to a particular extent, is not healthy to another particularextent. To elaborate this intuitive idea, let us arrange some terminology.
Considering a set A as a fuzzy set means that an object x is to somedegree a member of that set. Let us express this membership degree byµ(x, A), to be read as ‘the degree of membership of object x in set A’,conveniently abbreviated to µA(x). The symbol µA is referred to as themembership function of set A which assigns to an object x its membershipdegree µA(x). The membership degree µA(x) of object x in set A is sup-posed to be a real number in the unit interval [0, 1].4 Thus, the expression‘µyoung(Alf) = 0.7’ says that Alf is to the extent 0.7 a member of the set of
young people, or equivalently, that he is young to the extent 0.7.A function f is an assignment rule that assigns to a member of a set X aunique member of a set Y, also called a map from X to Y and simplyillustrated by f: X → Y. We will use this illustration to indicate that ‘f is amap from X to Y’. Let Ω be any set of objects. A fuzzy set A is obtainedby a membership function µA that maps members of Ω to the unit interval[0, 1] according to the following definitions:
Definition 1. If Ω is any set, A is a fuzzy subset of Ω if there is a function
µA such that1. µA: Ω → [0, 1],2. A = {(x, µA(x)) | x ∈ Ω}, that is, A is the set of all pairs (x, µA(x)) such
that x is a member of Ω and µA(x) is the degree of its membership in A.
Fig. 1. Gray, fog, and cloud as symbols of a fuzzy set. The more a member of the set is inthe gray area the lesser is the degree of its membership in the set.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
5/34
FUZZY HEALTH, ILLNESS, AND DISEASE 609
Definition 2. A is a fuzzy set , also called a fuzzy set in or over Ω, if A is afuzzy subset of Ω. The set Ω is referred to as the base set.
For example, given the base set {a, b, c, d} of four male doctors and afunction µproficient-doctor that assigns to any x ∈ {a, b, c, d} the degree of hisproficiency, then the following set is a fuzzy subset of our base set {a, b, c,d}, and thus a fuzzy set:
Proficient doctor = {(a, 0), (b, 0.4), (c, 0.8), (d, 1)}. (1)
Since the interval [0, 1] is uncountably infinite, a base set Ω may bemapped to [0, 1] in innumerably different ways. There are thus uncounta-bly infinite fuzzy subsets A, B, C, ... of a base set Ω. Given any such fuzzyset A in Ω, the negation of A, called its complement and denoted by Ac orNot A, is a fuzzy set that is defined by the following membership functionµAc:
µAc(x) = 1 – µA(x).
That is, Ac
= {(x, µAc(x)) | x ∈ Ω and µAc(x) = 1 – µA(x)}. For instance, thecomplement of the fuzzy set ‘proficient doctor’ mentioned in (1) above isthe fuzzy set:
Not proficient doctor = {(a, 1), (b, 0.6), (c, 0.2), (d, 0)} (2)
Of two numbers m and n the smaller one is called min(m, n), and the largerone is called max(m, n). These two functions, min and max , are defined asfollows:
min(m, n) = m, if n ≥ m= n, otherwise.
max(m, n) = m, if m ≥ n= n, otherwise.
For example, min(5, 3) = 3 and max(5, 3) = 5. Two fuzzy sets A and B ina base set Ω may have any relationships with one another. For example,their intersection, denoted by A ∩ B, is a fuzzy set defined by the minimaof their joint membership degrees; i.e., by the following membership func-tion µA∩B:
µA∩B(x) = min(µA(x), µB(x)).
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
6/34
KAZEM SADEGH-ZADEH610
That is, A ∩ B = {(x, µA ∩ B(x)) | x ∈ Ω and µA ∩ B(x) = min(µA(x),µB(x))}. And their union, denoted by A ∪ B, is a fuzzy set defined by themaxima of their joint membership degrees; i.e., by the following member-ship function µA∪B:
µA∪B(x) = max(µA(x), µB(x)).
That is, A ∪ B = {(x, µA ∪ B(x)) | x ∈ Ω and µA ∪ B(x) = max(µA(x),µB(x))}. A few examples will illustrate this terminology:
Ω = {a, b, c, d},Proficient doctor = {(a, 0), (b, 0.4), (c, 0.8), (d, 1)},Young doctor = {(a, 0.9), (b, 0.5), (c, 0.3), (d, 0.7)},Proficient doctor ∩ Young doctor = {(a, 0), (b, 0.4), (c, 0.3), (d, 0.7)},Proficient doctor ∪ Young doctor = {(a, 0.9), (b, 0.5), (c, 0.8), (d, 1)}.
The intersection A ∩ B represents a fuzzy conjunction (‘A and B’). Theunion A ∪ B represents a fuzzy disjunction (‘A or B’).
A base set Ω itself is the fuzzy set {(x, µΩ(x) = 1) | x ∈ Ω} all of whose
members have the membership degree 1. On the other hand, the emptyfuzzy set, written ∅, is {(x, µ∅(x) = 0) | x ∈ Ω} all of whose members havethe membership degree 0. Regarding the base set Ω = {a, b, c, d} of ourfour male doctors above, for instance, we have:
Ω = {a, b, c, d},Male = {(a, 1), (b, 1), (c, 1), (d, 1)} = Ω,Female = {(a, 0), (b, 0), (c, 0), (d, 0)} = ∅.
The fuzzy theory is a non-Aristotelian system because it does not accordwith the laws of excluded middle and contradiction. This is easily seenfrom the evidence that the union of a fuzzy set A and its complement A c
need not necessarily be the base set, and their intersection need not neces-sarily be empty:
A ∪ Ac ≠ Ω violation of the law of excluded middle (3)A ∩ Ac ≠ ∅ violation of the law of contradiction. (4)
(The symbol ‘≠’ negates equality and reads ‘does not equal’.) For in-stance, regarding the two example fuzzy sets mentioned in (1) and (2)above, we have:
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
7/34
FUZZY HEALTH, ILLNESS, AND DISEASE 611
Proficient doctor ∪ Not proficient doctor= {(a, 1), (b, 0.6), (c, 0.8), (d, 1)} ≠ Ω (5)
Proficient doctor ∩ Not proficient doctor= {(a, 0), (b, 0.4), (c, 0.2), (d, 0)} ≠ ∅ (6)
The union in (5) falls short of the base set, ‘the middle is not excluded’;and the intersection in (6) exceeds emptiness, ‘A does not contradict notA’. (For details, see Kosko, 1997; Sadegh-Zadeh, 2000a; forthcoming a).
III. FUZZY HEALTH
In what follows, I will construct a framework that makes health, illness,and disease amenable to fuzzy theory (Sadegh-Zadeh, 1997). To this end,a few new terms will be introduced to enhance the clarity of the context,whereas some other, traditional terms and relationships will be abandoned.To begin with, I will not consider disease as an opposite of health. Theopposite of health is malady (German ‘ Leiden’) that is a much broader
class than disease, containing besides disease also injury, wound, lesion,defect, deformity, disorder, syndrome, disability, impairment, and the like(Sadegh-Zadeh, 1982). Although it is not difficult to achieve agreementabout how to define the non-disease parts of this class of maladies, arecalcitrant problem to medicine is generated by the question: “What isdisease?”
The persistent mistake made in treating this foundational question is atypical petitio principii in that to define the notion of disease, one seeksafter common characteristics of its individual referents, i.e., of phenomena
such as ‘hepatitits’, ‘multiple sclerosis’, etc., that in our textbooks areclassified as ‘diseases’. However, such entities will come into being quaindividual diseases after a notion of disease one is seeking for has alreadybeen defined, but not before. A concept of disease-in-general must, there-fore, precede the inclusion and exclusion of phenomena as individualdisease entities. That means that the question of “What is disease?” canonly be decided prescriptively, not descriptively; i.e., it must be tackledaxiomatically, not empirically. The attempt to define ‘disease’ descrip-tively is a philosophical sin because it is a conceptual Unsinn (Sadegh-
Zadeh, 1977).5In what follows, a method is outlined that may assist in resolving this
basic problem of medicine. To this end, a concept of disease will beintroduced extensionally-recursively. The notion of health will be treated
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
8/34
KAZEM SADEGH-ZADEH612
separately, independent of disease so defined. It will be based upon anovel concept of patienthood of which the notion of health will be the
additive inverse in the following sense. Health = 1 – patienthood.6Let Ω be the set of human beings at a particular time. Suppose there is a
fuzzy subset P of Ω whose members are to various extents characterizedby discomfort, pain, endogenously threatened life, loss of autonomy, lossof vitality, and loss of pleasure. The extent to which an individual is amember of this fuzzy set P is called the degree of her patienthood (Sa-degh-Zadeh, 1982). This degree of patienthood of an individual x ∈ Ω isindicated by the fuzzy set membership function µpatienthood such thatµ
patienthood(x) is a real number in the unit interval [0, 1]. That provides the
following map: µpatienthood: Ω → [0, 1], which yields the fuzzy set P an-nounced above: P = {(x, µpatienthood(x)) | x ∈ Ω}.
The complement of patienthood, Pc, is referred to as health (‘the set of healthy people’) and is written H instead of Pc. The degree of health of anindividual x ∈ Ω is indicated by the membership function µhealth. Theterminology is thus:
µpatienthood(x) = degree of patienthood of x,
µhealth(x) = degree of health of x,
where µhealth is defined as follows:
Definition 3. µhealth(x) = 1 – µpatienthood(x),
and yields the health fuzzy set:
H = {(x, µhealth(x)) | x ∈ Ω}.
For example, according to the arrangements above, an individual’s degreeof health is 0.6 if she has a patienthood of 0.4. Since that individual is tothe extent 0.6 a member of set H, and to the extent 0.4 a member of itscomplement set P, she is to the extent min(0.6, 0.4) = 0.4 a member of thefuzzy set intersection H ∩ P. Hence, the intersection of health and patient-hood , H ∩ P, is not empty. That means that health and patienthood arecomplementary in a fuzzy sense, but not disjoint and contradictory in abivalent, Aristotelian sense.
As I will argue, health and disease also are not dual and contradictory. Itis not true that an individual is either healthy or diseased, and never both atthe same time. It may be that someone, e.g., Anne, has a particular diseasesuch as calcinosis circumscripta of her thyroid gland, whereas she is abso-
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
9/34
FUZZY HEALTH, ILLNESS, AND DISEASE 613
lutely healthy because of her µhealth(Anne) = 1. A disease that does notraise patienthood is not detrimental to health. (See Section V.)
IV. FUZZY ILLNESS
Usually an individual is said to be either healthy or ill, but not both at thesame time. This dichotomous terminology is inadequate and misleading,however, for illness and health are not conceptual opposites. “Ill” healthand “well” health, i.e., illness and wellness, are particular fuzzy states of health besides many other ones. To uncover this rich fuzzy structure of health, I will reconstruct the syntax of the phrase ‘state of health’. To thisend some terminology may be in order. I will briefly explain the notions of linguistic variable and semantic operator and will then return to the theme.(For details of the theory, see Sadegh-Zadeh, 1997; 1998; forthcoming a.)
The State-of-Health Variable
Properties of an object that do not remain constant are called variables.Distinguish between two types of variables: numerical and linguistic. A
numerical variable, such as ‘height’, assumes numbers as values. Forexample, “the height of David is 175 cm.” A linguistic variable, on theother hand, assumes linguistic entities, such as words or sentences, asvalues (Zadeh, 1975a; 1975b; 1976). For instance, color in the statement“the color of blood is red” is a linguistic variable. Its possible values arecolor terms such as ‘red’, ‘yellow’, ‘green’, etc. The totality of the possi-ble values of a linguistic variable v is referred to as its term set andwritten T(v). In the present example we have T(color) = {red, yellow,green, ... }.7
‘State of health’ will be construed as a linguistic variable whose termset may be conceived of as something like {well, not well, very well, ill,not ill, ...}. To elaborate this idea consider a simple example. The age of people may be described by statements such as:
David is 19 years old, (7)Theresa is 99 years old,
on the one hand, and by statements such as:
David is young, (8)Theresa is quite old,
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
10/34
KAZEM SADEGH-ZADEH614
on the other. Relationships of this type may be conceptualized by intro-ducing two variables, a numerical variable age and a linguistic variable Age. The former assigns numerical age to an individual, as in (7):
age of David is 19 yearsage of Theresa is 99 years,
whereas the latter assigns a linguistic term, as in (8):
Age of David is young,Age of Theresa is quite old .
The range of the numerical variable age is a set of integers such as {0, 1, 2,..., 120, ...}. The term set of the linguistic variable Age is a set of linguisticage labels such as T(Age) = {very young, young, not young, adult, old,quite old, more or less old, ....}. One may try to understand the relationshipbetween these two variables in the following way. (See Figure 2.)
The linguistic variable Age operates upon the numerical variable ageand transforms subsets of its values {0, 1, 2, ..., 120, ...} into fuzzy sets
which are termed ‘young’, ‘old’, ‘quite old’, etc. That is, any term τi of theterm set T(Age) is the name of a fuzzy set over the set of numerical ages. Aname τi such as ‘young’ thus subsumes an entire set of different numericalages under a single fuzzy set label. It is, therefore, quite reasonable to askof any particular numerical age such as 19 to what extent it is a member of
Fig. 2. The values of the linguistic variable ‘Age’ are young, not young, old, etc. Each of the latter ones is a label for an entire fuzzy set of numerical ages. See text.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
11/34
FUZZY HEALTH, ILLNESS, AND DISEASE 615
that fuzzy set τI; e.g., of the fuzzy set young. How young is 19? How old is
it? (See Figure 3.)By analogy, ‘state of health’ may be construed as a linguistic variable,
symbolized by state-of-health, whose term set may be conceived of assomething like:
{well, not well, very well, very very well, extremely well, (9)ill, not ill, more or less ill, very ill, very very ill, extremelyill, not well and not ill, … etc. …}.
The variable operates over the fuzzy set health introduced in Section III. Itassigns to degrees of health, i.e., to µhealth values, elements of its term set(9). Each element τi of this term set is thus the name of a particular fuzzyset that is a fuzzy subset of health. It subsumes an entire set of different
Fig. 3. A tentative illustration of the fuzzy sets young and old over the base set of thenumerical ages. The x-coordinate axis represents the set of numerical ages Ω = {0,1, 2, ..., 100, ..}. The y-coordinate axis displays the degree of membership, µτi(x),of numerical ages in any of the fuzzy sets young and old . The curves visualizethese two fuzzy sets. For instance, a newborn is young to the extent 1. The same istrue of the numerical ages 10 and 20. However, a man of 35 years is young only to
the extent 0.4, and old to the extent 0.1. Thus the membership functions µyoung andµold, here represented by µτi, map the set of numerical ages {0, 1, 2, ...} = Ω to theclosed interval [0, 1] generating two fuzzy subsets of the base set Ω that we call
young and old , respectively. The statement that an individual of 35 years old is young to the extent 0.4 thus means µyoung(35) = 0.4. And analogously, µold(35) =0.1 says that she is old to the extent 0.1.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
12/34
KAZEM SADEGH-ZADEH616
Fig. 4. Analogous with Fig. 2, the values of the linguistic variable ‘state-of-health’ may bevery well, well, not well, ..., ill, not ill, ... , etc. Each of them is a label for an entirefuzzy set of degrees of health. See text.
Fig. 5. A tentative illustration of the fuzzy set well and of its complement not well =unwell. The x-coordinate axis represents the fuzzy set health with its membershipfunction µhealth. The y-axis demonstrates the compatibility degrees of values of
µhealth with the fuzzy sets well and unwell, both represented by the membershipfunction µτi where τi is a place-holder for the terms ‘well’ and ‘unwell’. Accordingto this tentative demonstration, we have µwell(0.3) = µwell(µhealth(Pope)) = 0.1, andthus µunwell(0.3) = µunwell(µhealth(Pope)) = 0.9. Note that complementation is amirror image at point 0.5 of the y-axis.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
13/34
FUZZY HEALTH, ILLNESS, AND DISEASE 617
health values of the type µhealth(x) under a single fuzzy label τi such as‘well’, ‘ill’, etc. (See Figure 4). For instance, let the term ‘well’ designate
one of those fuzzy sets. One can ask how compatible with this set well thehealth value of a particular individual, such as µhealth(Pope) = 0.3, may be.If the membership function of the fuzzy set well is denoted by µwell, thequestion then reads: What is the value of µwell(0.3), i.e., of µwell(µhealth(Pope))? (Plots of two examples are displayed in Figure 5.)
The State-of-Health Operations
The term set T(state-of-health), as it has been partly displayed in (9) above,is a large set of linguistic terms that is based upon only a few primitivessuch as ‘well’ which we may call the primary terms of the variable. Theremaining elements of T(state-of-health) are composite terms such as ‘verywell’, ‘not well’, ‘not well and not ill’, etc. They are composed of primaryterms to which semantic operators such as very and not have been appliedto modify their meaning (Sadegh-Zadeh, 1998). A subset of T(state-of-health), e.g., the minimum term set {well, borderline}, may be used as aset of primary terms from which the remainder of T(state-of-health) maybe obtained by definition.
Semantic operators comprise:
1. complementation: ‘not’,2. connectives: ‘or’ and ‘and’,3. quantifiers: ‘all’, ‘almost all’, ‘most’, ‘about half’, ‘a few’, etc.4. linguistic hedges: ‘very’, ‘more or less’, ‘quite’, ‘fairly’, ‘extremely’,
etc. (Zadeh, 1972; Lakoff, 1973).
Categories 1 and 2 have already been dealt with earlier. Category 3 will
not be used here. A linguistic hedge such as ‘very’, when applied to anoperand like ‘well’, concentrates the meaning of the latter, whereas alinguistic hedge such as ‘more or less’ dilates the meaning of its operand:
concentration of a µA(x) is [µA(x)]2
dilation of a µA(x) is [µA(x)]1/2 = √ µA(x)
That means that if A is a fuzzy set,
very A is a fuzzy set with µvery(A)(x) = [µA(x)]2 ≡ concentrationmore or less A is a fuzzy set with µmore-or-less(A)(x) = [µA(x)]
1/2 ≡ dilation.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
14/34
KAZEM SADEGH-ZADEH618
For instance, regarding the previous example fuzzy sets:
Proficient doctor = {(a, 0), (b, 0.4), (c, 0.8), (d, 1)},Young doctor = {(a, 0.9), (b, 0.5), (c, 0.3), (d, 0.7)},
one obtains by concentration (‘very’) and dilation (‘more or less’):
Very proficient doctor = {(a, 0), (b, 0.16), (c, 0.64), (d, 1)},More or less young doctor = {(a, 0.94), (b, 0.7), (c, 0.54), (d, 0.84)}.
According to these standard approximations, one obtains from the primary
term set {well, borderline} a wide range of derived terms for T(state-of-health), such as the following:
very well = well2,more or less well = well1/2,ill = very(more or less ill) = very very unwell = unwell4 etc.,
by
µvery-well(x) = (µwell(x))2,µmore-or-less-well(x) = (µwell(x))
1/2,µill(x) = ((µill(x))
1/2)2 = (very(µunwell(x)))2 = (µunwell(x))
4.
(See Figure 6.) Thus, illness may be construed as a particular fuzzy setover health; i.e., as the following state of health:
very(very(not(well))) = unwell4,
which is a concentration of concentration of the complement of the fuzzyset well. It has become clear what it means to say that illness is not theconceptual opposite of health.
Due to the additive-inverse relationship between health and patient-hood, according to Definition 3 in Section III above, the state-of-healthfuzzy sets as illustrated in Figure 6 may also be based upon patienthood asthe base variable. They will in this case reverse their positions to appear asmirror images of those in Figure 6. (See Figure 7.)
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
15/34
FUZZY HEALTH, ILLNESS, AND DISEASE 619
Fig. 7. The same state-of-health fuzzy sets as in Fig. 6 based upon patienthood.
Fig. 6. A tentative illustration of some state-of-health fuzzy sets. All of them may bedefined by complementation, dilation, and concentration of the primary fuzzy setwell. Even borderline cases may be construed as some sort of ‘not well and notill’. Concentration by ‘very’ lowers membership degrees generating a deeper curve.Dilation by ‘more or less’ raises membership degrees generating a higher curve.Note that illness is very(very(not(well))) = unwellness4. For instance, a healthvalue of 0.4 corresponds to an illness of degree 0.5. An individual who is healthyto the extent 0.4, is ill to the extent 0.5, i.e. healthy and ill at the same time. Hence,health and illness are not contradictory and disjoint. And interestingly enough, thesame individual is also not ill to the extent 0.5. Hence, being ill and not being ill atthe same time is possible, though a contradictory state. The logic of clinical lan-guage, and consequently the logic of medicine, is a non-classical one that admitsof contradictions (see Section VII).
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
16/34
KAZEM SADEGH-ZADEH620
V. FUZZY DISEASE
Suffering abounds in the human world. But it falls within the responsibil-ity of medicine only if it is a facet of patienthood and phenomenologicallyappears as a state of ill health = ill state of health = illness as explicated inthe last section and illustrated in Figures 6 and 7. Illness in this sense, orsickness, may be generated by a multitude of causes from among the classof maladies, including a cause of a particular type called disease. What isdisease?
In natural languages the predicate ‘is’ plays at least four logically dif-ferent roles. It indicates
membership: David is young a ∈ Y,subsethood: man is a mammal Man Mammal,equality: two and three is five (2 + 3) = 5,equivalence: not true is false not true α ↔ false α.
For this reason the question “What is disease?” is by no means clear and isthus usually misunderstood. Let us, therefore, reformulate it: How could
the term ‘disease’ be defined if one were to define it?The word ‘disease’, like any other term, may be defined in n = ∞ differ-ent ways. For example, x is a disease if and only if x = 33. None of theseinnumerable possible definitions is right or wrong. For a definition putforward is not subject to verification or falsification according to anyscientific standards, but to the acceptance or rejection by those peoplewhose lives it affects. For this pragmatic reason, a concept of disease foruse in medicine should not be constructed irrespective of potential patientsand non-patients whose lives will be affected by that concept (Sadegh-
Zadeh, 1977, p. 39).In contrast with a linguistic definition introduced and printed in a publi-
cation, the decision of the public about how to use a concept may betermed a social definition. For example, by their opposition to classifyingseveral types of sexual behavior as diseases, people in Western societieshave changed medicine’s concept of disease during the last four decades.This political behavior of the public demonstrates a social definition of thenotion of ‘disease’.
Any concept of disease that, in medical literature and communities, may
underlie medical practice and research exists for the sake of the public, notfor medicine’s own sake. In order for a linguistic definition of such aconcept to be comprehensible to the public and to guide their social defini-tion, it should orient itself to their real lifeworld, needs and interests.
⊃
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
17/34
FUZZY HEALTH, ILLNESS, AND DISEASE 621
According to this axiom of functionality, it is advisable to ground thedisease language of medicine not on abstract, “unworldly” concepts, such
as quantum field theory or the evolution of the species, which the com-monsense would be unable to assess, but on something that people un-questionably consider a disease. In this way, all philosophical pseudo-problems that medicine and some of its philosophers generate in connec-tion with the concept of disease will disappear. Despite all paradigm shiftsin the last three millennia, no rational human being since Hippocrates’times would deny that there are instances of death caused by dramatic lifeevents such as heart attack, stroke, and breast cancer, or would disagreewith labeling such a real-life drama a dis-ease = disease. That means thatobviously there are some anthropological constants which all rationalhuman beings would be prepared to label a ‘disease’ by pointing to themand declaring, “look: this is a disease!”. Why not use such generally ac-cepted, demonstrable prototypes as a point of departure? I will do so andwill choose this lifeworldly grounded, paradigmatic-extensional approachin hopes of furthering constructive inquiry (Sadegh-Zadeh, 1982; 1997;forthcoming c).
Potential candidates for ‘disease’ are complex human conditions like
heart attack, stroke, breast cancer, etc. Such complex human conditionsare not, and should not be, merely confined to biological states of theorganism. They may be viewed and represented as large fuzzy sets whichalso contain parts that may refer to the subjective, religious, transcenden-tal and social world of the ill, such as, for example, pain, distress, feelingsof loneliness, beliefs, behavioral disorders, etc.
Suppose there is a small set {D1, D2, ..., Dn} of about n = three, five orten human conditions such as {myocardial infarction, stroke, breast can-cer, tuberculosis of the lung, malaria, ...} each of which in a particular
human society is accepted as a disease because of a finite set of m ≥ 1criteria {C1, C2, ..., Cm} they may have in common to varying extents.Criteria of this kind may include, for example, being a bodily lesion,causing pain, distress, discomfort, incapacity, dependency, premature death,and the like. It is in principle possible for members of any such humansociety to achieve consensus about both the small base set {D1, D2, ..., Dn}and the few criteria {C1, C2, ..., Cm}.
Upon such a linguistically firm ground in that society one may tenta-tively seek for a quasi-inductive definition such as the following:
Basis: any element of the base set {D1, D2, ..., Dn} is a disease;Induction: any event that is similar to a disease with respect to the
criteria {C1, C2, ..., Cm} is a disease.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
18/34
KAZEM SADEGH-ZADEH622
The first step says that “D1 is a disease, D2 is a disease, ..., and Dn is adisease,” such as, for example, “Myocardial infarction is a disease, stroke
is a disease, ... malaria is a disease.” This basic step is unproblematicbecause it rests on consensus in that society. It would provide the membersof the society with the prototype elements of a quasi-inductive set to beconstructed and called “disease.” The only problem to resolve may lie inthe similarity relationship required in the induction step. There is fortu-nately an excellent concept of similarity that will assist us in this task(Kosko, 1997; Sadegh-Zadeh, 1999a). Fuzzy set difference indirectly de-fines similarity. The degree of difference between two fuzzy sets A and B,denoted by differ(A, B), is defined as follows:
∑imax (0, µ
A( x
i) – µ
B( x
i)) + ∑
i max (0, µ
B( x
i) – µ
A( x
i))
differ(A, B) = .c(A ∪ B)
In the denominator, c is the fuzzy set count and means the sum of a set’smembership degrees. For example, let X = {(x, 0.6), (y, 0.9)} be a fuzzyset, its count is c(X) = 0.6 + 0.9 = 1.5. Accordingly, given two fuzzysets:
X = {(x, 0.6), (y, 0.9)},Y = {(x, 0.7), (y, 0.4)},
then according to the definition above we have:
differ(X, Y) = [(0 + 0.5) + (0.1 + 0)]/(0.7 + 0.9) = 0.6/1.6 = 0.375.
Thus, set X differs from set Y to the extent 0.375. The notion of differencecaptures the gross deviation of membership degrees of sets A and B from
one another, averaged over the union count c(A ∪ B). The degree of equality or similarity beween two fuzzy sets A and B, denoted by similar(A, B), is the additive inverse of their difference:
Definition 4. similar(A, B) = 1 – differ(A, B).
The less two fuzzy sets differ from one another, the more similar they are.The two example fuzzy sets X and Y above are similar to the extent 1 –0.375 = 0.625. Fuzzy set difference and similarity are real numbers in the
interval [0, 1]. A very convenient method of computing similarities isprovided by the following interesting theorem that cannot be proved here(Sadegh-Zadeh, 1999a):
Theorem 1. similar(A, B) = c(A ∩ B)/c(A ∪ B).
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
19/34
FUZZY HEALTH, ILLNESS, AND DISEASE 623
That is, the degree of similarity between set A and set B equals the countof their intersection divided by the count of their union. Regarding our two
example sets X and Y above, we have, according to this theorem:
similar(X, Y) = (0.6 + 0.4)/(0.7 + 0.9) = 0.625.
Similarity, thus defined, is a relationship between fuzzy sets. Hence, todetermine the similarity between any of the prototype diseases {D1, D2, ...,Dn} above and any other phenomenon requires that they all be formulatedas fuzzy sets (for details see Sadegh-Zadeh 1997; forthcoming c).
For example, a human condition, such as myocardial infarction, may beconstrued as a set consisting of a large number of attributes, such as{myocardial ischemia, arrhythmia, abnormal ECG, elevation of LDH en-zyme, chest pain, fear of death, ... etc. ...}. In comparison, another humancondition, such as gastric ulcer, may be another set consisting of anotherlarge number of attributes. Although phenomena of these divers kinds arein principle comparable with one another, they are not easily comparablein their entirety. For this practical reason, I am not interested in similarity-in-general, but am seeking for similarity-in-some-particulars. Therefore,
in comparing those phenomena to determine the degree of their similarity,one does not compare them as a whole. One compares them only withrespect to a particular set of criteria, that is, with respect to a comparablesubset of their attributes. For example, one asks how similar they are withrespect to being a bodily lesion and causing pain, distress, discomfort,incapacity, dependency, and premature death, say, criteria {C1, C2, ..., Cm}with m ≥ 1. In other words, in comparing two large, possibly incommensu-rable human condition sets Di and D j, we ask: everything else left aside,how similar are Di and D j with respect to the few criteria {C1, C2, ..., Cm}
they share to varying extents? This kind of similarity confined to particu-lar criteria such as {C1, C2, ..., Cm} is referred to as partial similarity withrespect to this set of criteria.
Let A be a fuzzy set of arbitrary length, and let X be part of it. We writeA\X to indicate that A is a fuzzy set with X being part of it. For example,A\{(z, 0.7)} in a particular context may stand for fuzzy set A = {(x, 0.5),(y, 0.6), (z, 0.7)}. In this way, it becomes possible to arrange humanconditions such as myocardial infarction and gastric ulcer as uniform fuzzysets with respect to their comparable criteria {C1, C2, ..., Cm}:
myocardial infarction\{(C1, a1), (C2, a2), …, (Cm, am)},gastric ulcer\{(C1, b1), (C2, b2), …, (Cm, bm)}
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
20/34
KAZEM SADEGH-ZADEH624
as, for example:
myocardial infarction\{(bodily lesion, 1), (pain, 0.7), (distress, 0.8)}gastric ulcer\{bodily lesion, 1), (pain, 0.3), (distress, 0.5)} (10)
and to compare them with respect to their uniform, terminal criteria seg-ments:
X = {(C1, a1), (C2, a2), ..., (Cm, am)},Y = {(C1, b1), (C2, b2), ..., (Cm, bm)}.
Their remaining, initial, segments pertaining to ECG, blood pressure, en-zyme disorders, bacterial infection, etc. may not be comparable and are,therefore, not considered here. Partial comparisons sketched thus far re-veal degrees of partial similarity, symbolized by p-similar(A\X, B\Y), ac-cording to the following definition.
Definition 5. p-similar(A\X, B\Y) = r if and only if similar(X, Y) = r.
For instance, according to Definition 5 and Theorem 1, the two examplesin (10) display the following partial similarity:
p-similar(myocardial_infarction\X, gastric_ulcer\Y) = 0.72.
That means that with respect to their terminal criteria sets X and Y, myo-cardial infarction and gastric ulcer are p-similar to the extent 0.72.
I am now in a position to elaborate the previously envisaged quasi-inductive definition of ‘disease’. Let {D1, ..., Dn} be a small set of human
conditions such as {myocardial infarction, stroke, breast cancer, tubercu-losis of the lung, ..., malaria} each of which in a particular human societyis accepted as a disease because of a finite set of criteria {C1, ..., Cm} theymay have in common to varying extents. A concept of disease for that society may be constructed quasi-inductively if in that society there is aconsensus on a degree ε of p-similarity that will serve as a pillar of theconstruction:
Definition 6. 1. Any element of the base set {D1, ..., Dn} is a disease;
2. A human condition H\X is a disease if there is a diseaseDi \Y ∈ {D1, ..., Dn} and an ε > 0 such that p-similar(H\X,Di \Y) ≥ ε.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
21/34
FUZZY HEALTH, ILLNESS, AND DISEASE 625
Suppose, for instance, that the following set:
myocardial infarction\{(C1, 1), (C2, 0.7), (C3, 0.8)} (11)
is an element of the base set {D1, ..., Dn} and thus a disease according toclause 1 of Definition 6. The question as to whether or not something likehemorrhoids, bald head, pregnancy, homosexuality or drapetomania thatis not contained in the base set {D1, ..., Dn} is a disease is easily decided bydetermining the least degree of partial similarity required in clause 2 of Definition 6. If, for example, ε = 0.6 is required and there is a humancondition such as:
hemorrhoids\{(C1, 0.9), (C2, 0.2), (C3, 0.55)},
then we have:
p-similar(hemorrhoids\X, myocardial_infarction\Y) = 0.66.
Thus, hemorrhoids may also be labeled a ‘disease’. Regarding any otherhuman condition one may proceed analogously.
Note that, due to the continuity of the similarity degree ε appearing inthe quasi-inductive scheme of Definition 6, the number of theoreticallypossible concepts of disease-in-general is infinite because there are infi-nite options to choose an ε (Sadegh-Zadeh, 1977, p. 15). The smaller ε, thelarger the class of emerging diseases. So the question arises: What ε tochoose and who will decide about this question to obtain a particularconcept of disease for use in health care? From what has already been saidabove, the answer to this question is clear: not medicine, but the public,will have to make that decision.8
The class of diseases ensuing from a general concept of disease accord-ing to the scheme of Definition 6 is not fuzzy, for a human condition suchas those listed in (10) above either definitely is, or definitely is not, adisease according to that scheme. From a particular theoretical perspectiveit may appear desirable to have a concept of fuzzy disease, however. Anindividual disease entity produced by such a concept would not be a cate-gorical, YES or NO, disease any more, but a graded one, i.e., a disease toa particular extent . This option is demonstrated by the following, modi-fied quasi-inductive scheme.
Definition 7. Let H be the set of human conditions. A fuzzy setD overH is called the set of diseases if and only if there is a subset {D1, ..., Dn}of H and a function µ
D such that:
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
22/34
KAZEM SADEGH-ZADEH626
µD
: H → [0, 1]
with:
1, if Hi \X ∈ {D1, …, Dn}, called a prototype or coredisease;
µD (Hi \X) = ε, if there is a prototype disease H j \Y with
p-similar(Hi \X, H j \Y) = ε, and there is no prototypedisease Hk \Z with p-similar (H i \X, H k \Z) > ε,
and D = {(Hi, µD (Hi)) | Hi ∈ H }.
This modified scheme does not require a limiting threshold similarity. Itproduces a fuzzy set of the type D = {(D1, µD (D1)), ..., (Dq, µD (Dq))}consisting of individual disease entities that are members of the set D todifferent degrees, i.e., diseases to different degrees. The membership de-gree µ
D(Di) ranges from 1 to 0. According to this method of concept
formation, an individual’s health condition:
hemorrhoids\{(C1, 0.9), (C2, 0.2), (C3, 0.55)},
as compared to a prototype disease like (11) above may turn out to be adisease to the extent 0.66, whereas another individual with
hemorrhoids\{(C1, 0.2), (C2, 0.1), (C3, 0.1)}
will have a disease of negligible degree 0.16.
It is evident from these examples that a person who has a disease of aparticular degree r, has a non-disease of degree 1 – r at the same time. Thereason is that an occurrence that according to Definition 7 is a disease Di tothe extent r, is a non-disease to the extent 1 – r because to this extent itbelongs to the complement fuzzy set D c. An individual’s having thedisease Di to the extent r therefore means that she does not have it to theextent 1 – r. Thus, fuzzy disease is non-Aristotelian. You both have it anddo not have it. The existence of contradictory states of this kind damagesthe trust in the acceptability of classical logic that is based upon the princi-
ple of non-contradiction (see Section VII, D below).
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
23/34
FUZZY HEALTH, ILLNESS, AND DISEASE 627
VI. THE PROTOYPE RESEMBLANCE THEORY OF DISEASE
Building upon the conceptual preliminaries above, one may also speculateabout the entities that in a human society are termed diseases, using a newparadigm that among other things may assist in developing new approach-es to nosology. (For details, see Sadegh-Zadeh, 1997; forthcoming b).
A disease in a human society is a point in a multidimensional ballcentered around a value-laden prototype human condition undesirable inthat society. The undesirability of the prototype determines the content of the ball through similarity relationships. This anthropological hypothesisin favor of the normativist perspective on disease may be explicated in thefollowing way.
Let H = {H1, H2, ...} be the set of human conditions. Its elements H1,H2, ... may be formulated as partial fuzzy sets Hi \X of the type above, suchas Hi \{(C1, a1), ..., (Cm, am)} where an ak is the degree of membership of the criterion Ck in the set Hi, for example:
myocardial_infarction\{(bodily_lesion, 1), (pain, 0.7), (distress, 0.8)},gastric_ulcer\{(bodily_lesion, 1), (pain, 0.3), (distress, 0.5)},
hemorrhoids\{(bodily_lesion, 0.9), (pain, 0.2), (distress, 0.55)},bald_head\{(bodily_lesion, 0.1), (pain, 0), (distress, 0.01)},pregnancy\{(bodily_lesion, 0.1), (pain, 0.2), (distress, 0.4)},homosexuality\{(bodily_lesion, 0), (pain, 0), (distress, 0)},drapetomania\{(bodily_lesion, 0), (pain, 0), (distress, 0)},being_in_love\{(bodily_lesion, 0), (pain, 0), (distress, 0)}.
And let a partial difference function for fuzzy sets, p-differ(H i \X, H
j \Y), be
defined by:
p-differ(Hi \X, H j \Y) = r if and only if differ(X, Y) = r.
This partial difference function measures the distance between any twohuman conditions with respect to their criteria:
X = {(C1, a1), (C2, a2), ..., (Cm, am)},Y = {(C1, b1), (C2, b2), ..., (Cm, bm)},
and thus provides a metricd
overH
(see Sadegh-Zadeh, 1997; 1999a;1999b; forthcoming b). The structure becomes a metric spacewith:
d: H × H → [0, 1],
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
24/34
KAZEM SADEGH-ZADEH628
where H × H is the set of all pairs comprising pairs (Hi, H j) of humanconditions, and the distance between two such human conditions equals
their partial difference, i.e.:
d(Hi, H j) = p-differ(Hi \X, H j \Y) = differ(X, Y).
Given any element Hi of H and any particular degree δ of partial differ-ence, a ball of radius δ, called a δ-ball, centered at the point Hi and denotedby Bδ(Hi), may be defined in the following way:
Bδ(H
i) = {H
j | d(H
i, H
j) < δ} an open δ-ball,
Bδ(Hi) = {H j | d(Hi, H j) ≤ δ} a closed δ-ball.
The latter, closed δ-ball, for example, reads: the set of all human condi-tions H j whose distance from Hi equals δ at most.
Seen from this perspective, any non-fuzzy concept of disease that isintroduced according to Definition 6 with {D1, ..., Dn} as the set of itsprototype diseases creates for each prototype disease Di ∈ {D1, ..., Dn} aclosed δ-ball D i = Bδ(Di) of diseases centered at the point Di, where δ = 1
– ε with ε being the minimum similarity required in the definition. Thus,one obtains the following balls of diseases:
Bδ(D1) = D 1Bδ(D2) = D 2 (12)..Bδ(Dn) = D n
such that each disease ball Di yields a metric space with:
d: D i × D i → [0, 1], where d(D j, Dk) = p-differ(D j \X, Dk \Y).
The set (12) of the balls D 1, ..., D n comprises disease balls of differentsize and structure. Their entirety may be termed the nososphere of thegenerating concept of disease. They may, or may not, be co-centered at thecluster {D1, ..., Dn} of prototype diseases. In the former case, an overallball D = D 1 ∪ ... ∪ D n of diseases will ensue. (For details, see thegeometry of disease in Sadegh-Zadeh, 1997; forthcoming b).
The expressive power of this framework enables one to define nosologyas an endeavor that deals, over the setH of human conditions, with closedδ-balls of diseases centered at the chosen prototype diseases, D1, ..., Dn. If
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
25/34
FUZZY HEALTH, ILLNESS, AND DISEASE 629
you change any one of these prototypes or your δ, you will generate a newnososphere, and your nosological system and your health care will change.
Also, any fuzzy concept of disease that is introduced according to Defi-nition 7 with a set of prototype diseases {D1, ..., Dn}, yields closed δ-ballscentered at the points {D1, ..., Dn}. In this case, the balls are cloudy. A ballmay extend as far as δ = 1 and house gradual diseases. The disease inten-sity of a human condition decreases as it moves from the core to theperiphery of the ball. In the realm of such a fuzzy nosology, a humancondition is medically treated not because it is a disease, but because it isa disease to a particular extent that is no longer tolerable. Presumably,real-world health care rests upon such a fuzzy nosology (Sadegh-Zadeh,1997; forthcoming c).
VII. MEDICAL AND PHILOSOPHICAL PERSPECTIVES
Thus far, I have taken only a first step toward a new logic of the conceptsof health, illness, and disease. Although this novel, fuzzy-theoretic per-spective seems to be promising enough to provide a fertile ground for
substantial inquiries, I have not yet been able to say anything about thenature of health, illness, and disease as they may now appear. This poten-tial of the framework may be examined by future research and criticism.Here only a few practical and theoretical aspects will be outlined.
Fuzzy Nosology
First, individual disease entities, such as myocardial infarction, gastriculcer, and multiple sclerosis, may be conceptualized as fuzzy sets (seeSection V). Disease criteria, symptoms, and signs would then belong to an
individual disease to particular extents. Thus, an individual disease wouldappear as a multidimensional cloud rather than a clear-cut phenomenon. Itwould manifest itself quite differently in different patients and at differentstages. The myriad of individual patients presenting a particular disease,such as myocardial infarction, are just the scattered points of manifesta-tion of such a multidimensional cloud. The main source of misunderstand-ings and disagreements both in nosology and in the philosophy of healthand disease is basically this inherent fuzziness of the subject that has notyet been sufficiently recognized to evoke the need for an appropriate con-
ceptual apparatus and methodology. (For a multidimensional geometry of disease, see Sadegh-Zadeh, 1997; forthcoming b.)
For the sake of simplicity, I have in this non-technical paper present-ed fuzzy disease concepts as fairly primitive sets, such as, myocar-
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
26/34
KAZEM SADEGH-ZADEH630
dial_infarction\{(C1, a1), ..., (Cm, am)}, which entails a disease criterion Ciwith a single, sharp membership degree ai. In a more realistic and viable
way a fuzzy disease D may be represented by a more intricate type of fuzzy set, such as:
D\{(C1, [0.4, 0.8]) , (C2, [0, 0.9]), ..., (Cm, [0.6, 1])},
giving for each criterion Ci a membership interval [ai, bi] with a lowerbound ai and an upper bound bi of membership. Alternatively, this com-plex membership indicator [ai, bi] may be replaced with an even morecomplex one, i.e., a fuzzy number.9
However, I have preferred not to go into technical details here. It mayonly be noted that methods of this type would enable us to come to gripswith vague disease descriptions, such as: “ECG is usually normal, butheart beat is slightly accelerated , cholesterol is moderately increased , redblood count is highly decreased ....”.
As Definition 7 demonstrates, the class of disease-in-general itself mayalso be conceived of as a fuzzy set, such that being or not being an individ-ual disease entity may itself be handled as a matter of degree. In this case,
a disease entity may be graded as being, for example, of degree 1, of degree 0.9, of degree 0.8, etc., or by using linguistic fuzzifiers such assevere, moderate and mild , which may also be further diversified by ap-plying modifiers such as very and the like. The practices of tumor stagingand malignancy grading are examples of this kind of fuzzy nosology thathave already developed independently of fuzzy theory.
The next step in fuzzifying a nosological system would consist in allo-cating an individual disease entity to different fuzzy classes of diseases.For example, gastric ulcer may turn out to be a disease of the digestive
tract to the extent 1, an infectious disease to the extent 0.8, and a psycho-somatic disease to the extent 0.3.
In any event, fuzzy nosology would present itself as the science and artof framing, structuring, and analyzing the mutidimensional nosospherethat an underlying concept of disease generates (Sadegh-Zadeh, 1977).
Fuzzy Diagnosis and Therapy
Fuzzy nosology yields fuzzy diagnosis and fuzzy clinical decision-making(Sadegh-Zadeh, 2000b). First, one may be given a patient who displays
her complaints, symptoms, and signs at different levels of severity, inten-sity or clarity, such as {(cough, 1), (fatigue, 0.5), (fever, 0.7), (hypercho-lesterolemia, 0.6), ...}. She may thus belong to different fuzzy diseaseclasses at the same time and to different extents. Appropriate methods of
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
27/34
FUZZY HEALTH, ILLNESS, AND DISEASE 631
analysis will be necessary to handle these modes of fuzzy multi-classmembership. This kind of investigation is currently emerging in the area
of medical knowledge-based systems research.10 A prerequisite for fruit-ful work will be a medical epistemology which clearly suggests how med-ical knowledge – nosological, symptomatological, pathophysiological, di-agnostic knowledge, etc. – may be represented in fuzzy terminology. Thiswill bring with it the next prerequisite: i.e., a logic that would enable us todeal with fuzzy knowledge. Fuzzy logic, the logic part of fuzzy theory,seems to be a suitable candidate (see below).
Second, due to the ineluctable vagueness of physician and patientpreferences, goals, and constraints in clinical settings, on the one hand,and to uncertainties in treatment efficacy evaluations, on the other, treat-ment decisions also are likely to become subject to fuzzy decision-making(see Bellman and Zadeh, 1970).
Health, Illness, and Disease as Meinongian Objects
As I have argued in the preceding sections, fuzzy health, illness, and diseaseare non-Aristotelian attributes because they violate the principles of exclud-ed middle and non-contradiction. I consider fuzzy disease as an example
which shows that health, illness, and disease are not only subjects of medi-cal and philosophical concern, but also intriguing ontological objects.Let a particular disease such as gastric ulcer be reconstructed as a fuzzy
disease. We have seen in Section V that a patient suffering from fuzzygastric ulcer both does and does not have it at the same time. But a state-ment of the form ‘x has A and x does not have A’ is a classical-logicalcontradiction. A state of affairs described by such a contradiction is usual-ly viewed as impossible, and thus as non-existent, because the classical-logical principle of non-contradiction, initially formulated by Aristotle,
precludes its existence.11 It is, therefore, said that an impossible state of affairs does not exist. However, fuzzy disease states demonstrate that theimpossible does exist. All diseased patients and all recovering patientsindeed exhibit such existent impossibles every day. Hence, the principleof non-contradiction is not true. This is lethal to classical logic.
To put it positively, we may also suggest that health, illness, and diseaseare Meinongian objects. Alexius Meinong, an Austrian psychologist andphilosopher (1835-1920), developed a highly original and controversialtheory of objects according to which “there are objects that do not exist ...”
(Meinong, 1904; Grossman, 1974). Every such object, he said, may bedescribed nonetheless (for example, a round square). Something is a roundsquare if it is round and if it is square. If it is round, it is not square. Thus,it is square and it is not square: a contradictory object.
b y g u e s t onF e b r u ar y 7 ,
2 0 1 1
j m p. ox f or d j o ur n
al s . or g
D ownl o a d e d f r om
http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/http://jmp.oxfordjournals.org/
-
8/18/2019 Lógica DIfusa Salud Enfermedad y Malestar
28/34
KAZEM SADEGH-ZADEH632
In Meinong’s theory of objects, an impossible object is one that violatesthe principle of non-contradiction: e.g., a round square. And an incompleteobject is one that violates the principle of excluded middle. In this sense,health, illness, and disease states of individual human beings are Mei-nongian objects. And because they exist in the real world, I call them realMeinongian objects. A serious consequence of this finding may be brieflysketched in the next subsection.
The Logic of Medicine
A domain such as medicine that entails real Meinongian objects generatesinconsistent theories in the sense of classical logic. Inconsistencies trivial-ize a theory and destroy its meaning in that such a theory classical-logical-ly implies anything (ex falso quod libet ). Therefore, one cannot reasonablysubscribe to both and must abandon one of them, either the theory orclassical logic.
Classical logic may be a useful tool in consistent areas, though it isobviously not an appropriate tool for medicine as a whole. Medicine is toonon-homogeneous an area. The theories produced by its subdomains suchas anatomy, physiology, pathophysiology, clinical disciplines, etc., are
conceptually, syntactically and semantically too different from one anoth-er to assume one and the same logic. As I have shown elsewhere (Sadegh-Zadeh, 1994; forthcoming