
NUEVAS DIANAS TERAPÉUTICAS EN CÁNCER DE...
46
Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla, Santander Organizado por: Fundación para el progreso de la oncología en Cantabria NUEVAS DIANAS TERAPÉUTICAS EN CÁNCER DE ENDOMETRIO Dra. Eva Guerra Alía Unidad de tumores de mama y ginecológico Hospital Ramón y Cajal Madrid 4/7/18
Transcript of NUEVAS DIANAS TERAPÉUTICAS EN CÁNCER DE...
Coordinación científica:Dr. Fernando RiveraHospital Universitario Marqués de Valdecilla,
Santander
Organizado por: Fundación para el progreso
de la oncología en Cantabria
NUEVAS DIANAS
TERAPÉUTICAS EN CÁNCER DE
ENDOMETRIODra. Eva Guerra Alía
Unidad de tumores de mama y ginecológico
Hospital Ramón y Cajal Madrid
4/7/18

ÍNDICE
-INTRODUCCIÓN
-NUEVA CLASIFICACIÓN: TCGA
-PATHWAYS IDENTIFICADOS:
*RECEPTORES HORMONALES
*PI3K/AKT/Mtor
*RECEPTORES TIROSIN-KINASA
*ANGIOGÉNESIS
*RECOMBINACIÓN HOMÓLOGA
-CONCLUSIONES
INTRODUCCIÓN
- El cáncer de endometrio es el tumor ginecológico más frecuente en países desarrollados,
representando el 6% de los diagnósticos de cáncer y siendo el responsable del 3% de las
muertes por cáncer.
- La mayoría se diagnostican en estadios localizados (72%), sin embargo un 15-20% de
estos tumores, presentarán una recaída.
- La mediana de supervivencia a los 5 años:
Estadio I: 90%
Estadio II: 60-77%
Estadio III: 27-40%
Estadio IV: 0-5%
- Para la enfermedad avanzada, la supervivencia ha permanecido sin cambios en los
últimos 25 años ( mediana de supervivencia: 7-15 meses), siendo necesario el desarrollo
de nuevas terapias.
TRATAMIENTO ACTUAL ENFERMEDAD AVANZADA
• Quimioterapia:
– Primera línea: Taxanos, doxorrubicina, platino
– Respuestas en monoterapia: 35%; en combinación: 70%
– Esquemas muy tóxicos
– Carboplatino-Taxol esquema más ampliamente utilizado
– PFS: 8 m; OS: 15 m
– Segunda línea: no claro consenso: agentes en monoterapia: RR 4-22%
• Hormonoterapia:
– Progestágenos, antiestrógenos, inhibidores de la aromatosa
– Tumores endometrioides y de curso indolente: RR 30%
– No segunda línea claramente establecida

CLASIFICACIÓN DICOTÓMICA
Murali R, Lancet Oncol 2014
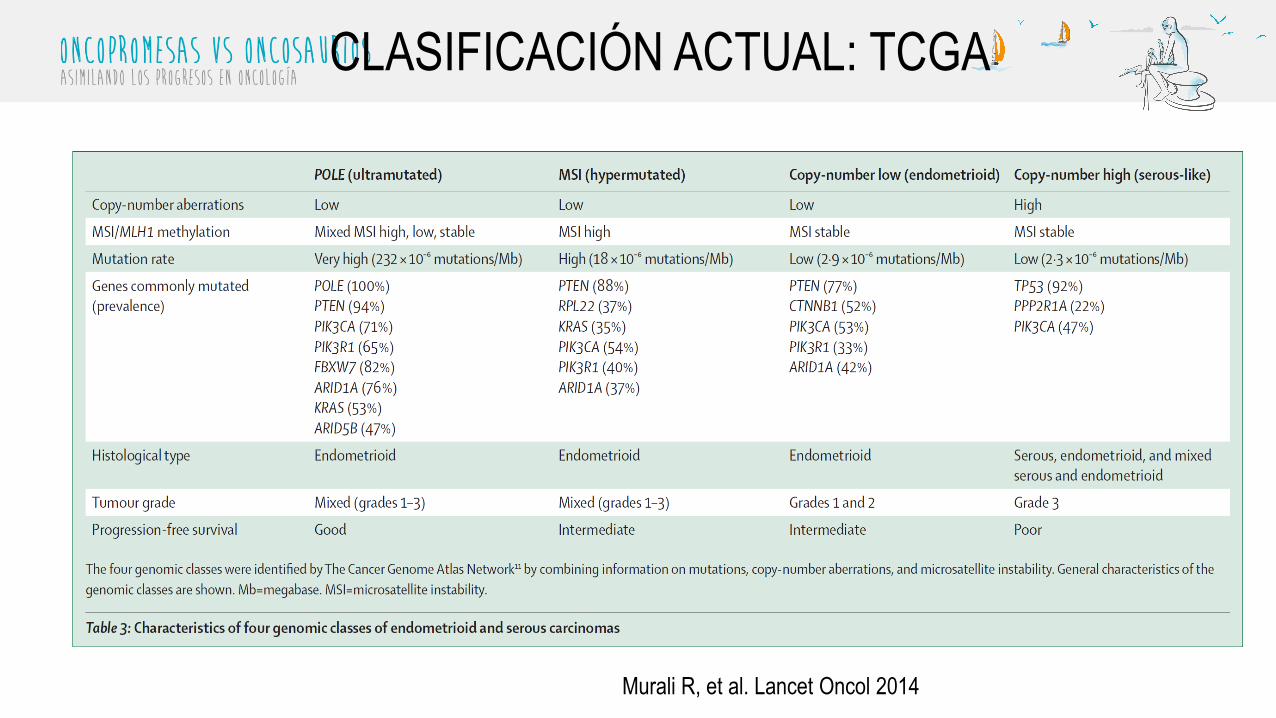
CLASIFICACIÓN ACTUAL: TCGA
Murali R, et al. Lancet Oncol 2014
POTENCIALES NUEVAS DIANAS
TERAPÉUTICAS

NUEVAS ESTRATEGIAS TTO HORMONAL
• Anastrozol→ Ensayo ANZGOG0903 actualmente en reclutamiento
• Fulvestrant→ Alta afinidad por RE pero no efecto agonista. Fase II demostró mayor
respuesta en RP + (20%) que en RE+ (16%)
• BN83495 → inhibidor irresversible de la sulfatasa esteroidea impidiendo la formacion de
esteroides activos con efecto estrogénico. Existe un fase II en marcha que compara este
compuesto frente megestrol acetato (NCT00910091).
• Onapristona→ nuevo antagonista de RP tipo I. Fase I completo actualmente en
reclutamiento el fase II
Covens AL et al. Gynecol Oncol 2011
Woo LW et al Chem Med Chem 2011
Cottu H et al. J Clin Oncol 2015, abstr 5593
Cortesía Dr. Pérez Fidalgo
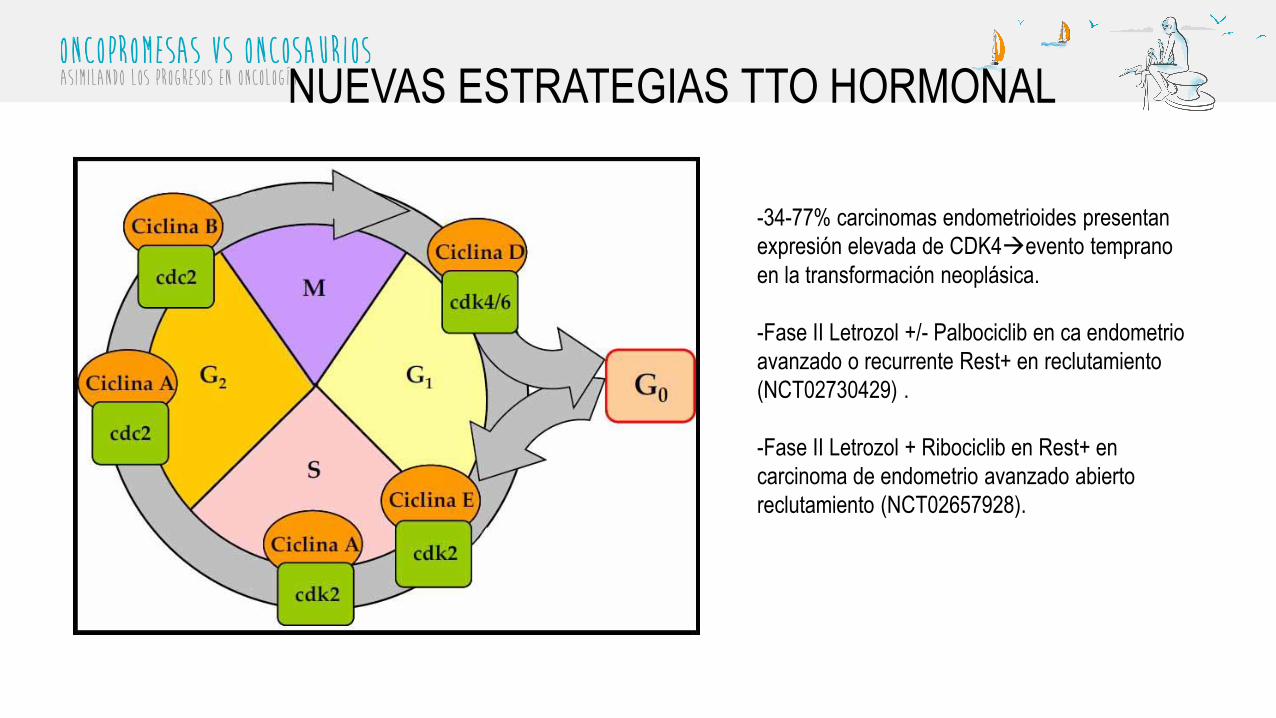
NUEVAS ESTRATEGIAS TTO HORMONAL
-34-77% carcinomas endometrioides presentan
expresión elevada de CDK4→evento temprano
en la transformación neoplásica.
-Fase II Letrozol +/- Palbociclib en ca endometrio
avanzado o recurrente Rest+ en reclutamiento
(NCT02730429) .
-Fase II Letrozol + Ribociclib en Rest+ en
carcinoma de endometrio avanzado abierto
reclutamiento (NCT02657928).

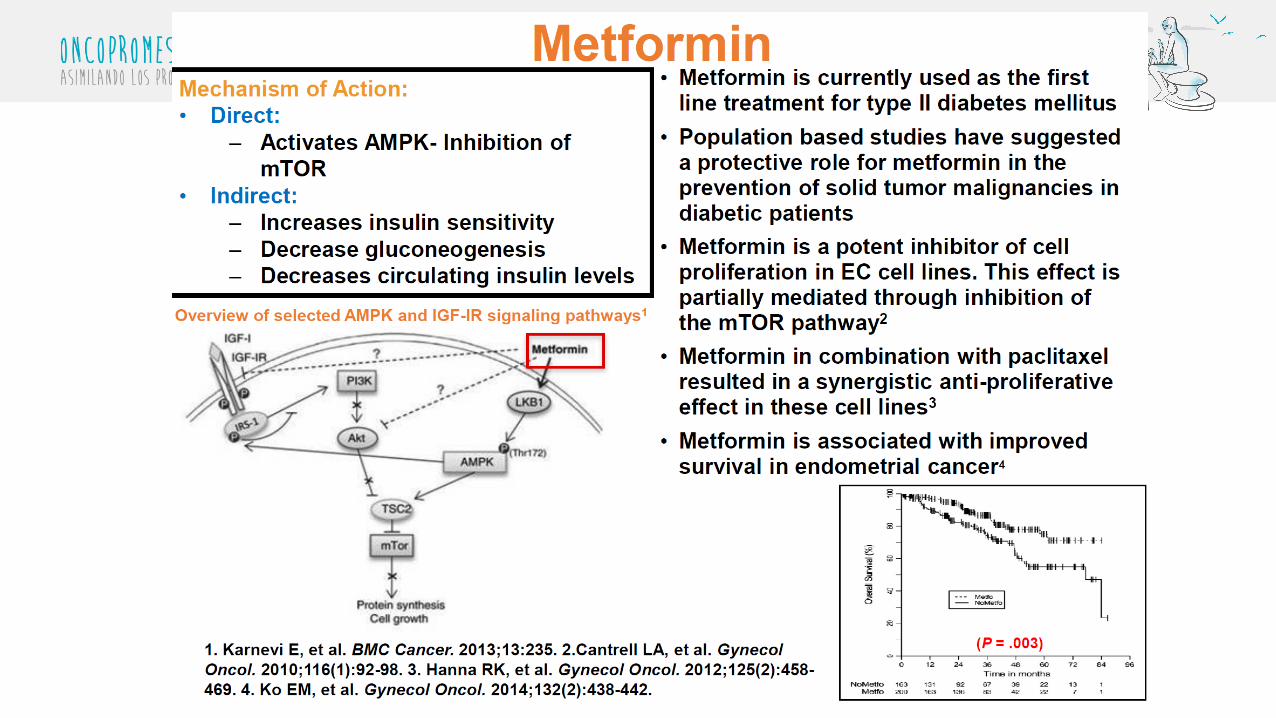
PI3K/AKT/Mtor/PTEN Signaling Pathway in endometrial cancer
Eritja N, et al. Advances in Experimental Medicine and Biology, 2017
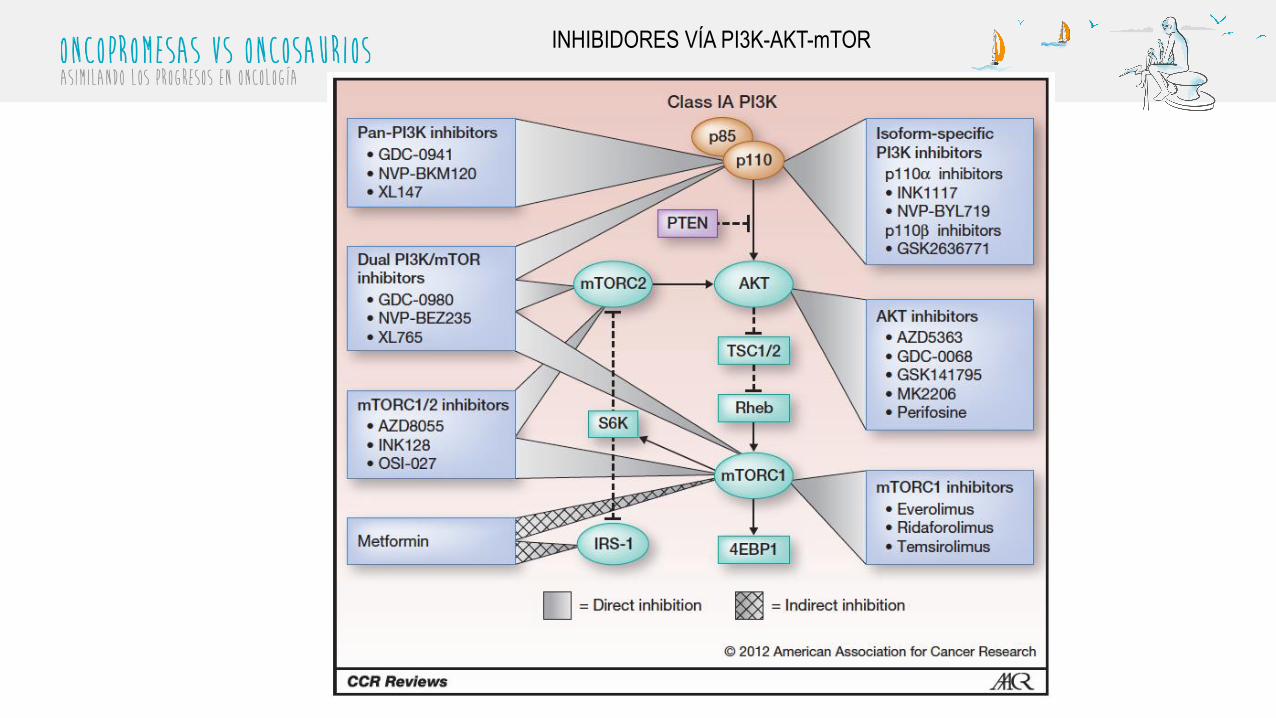
INHIBIDORES VÍA PI3K-AKT-mTOR
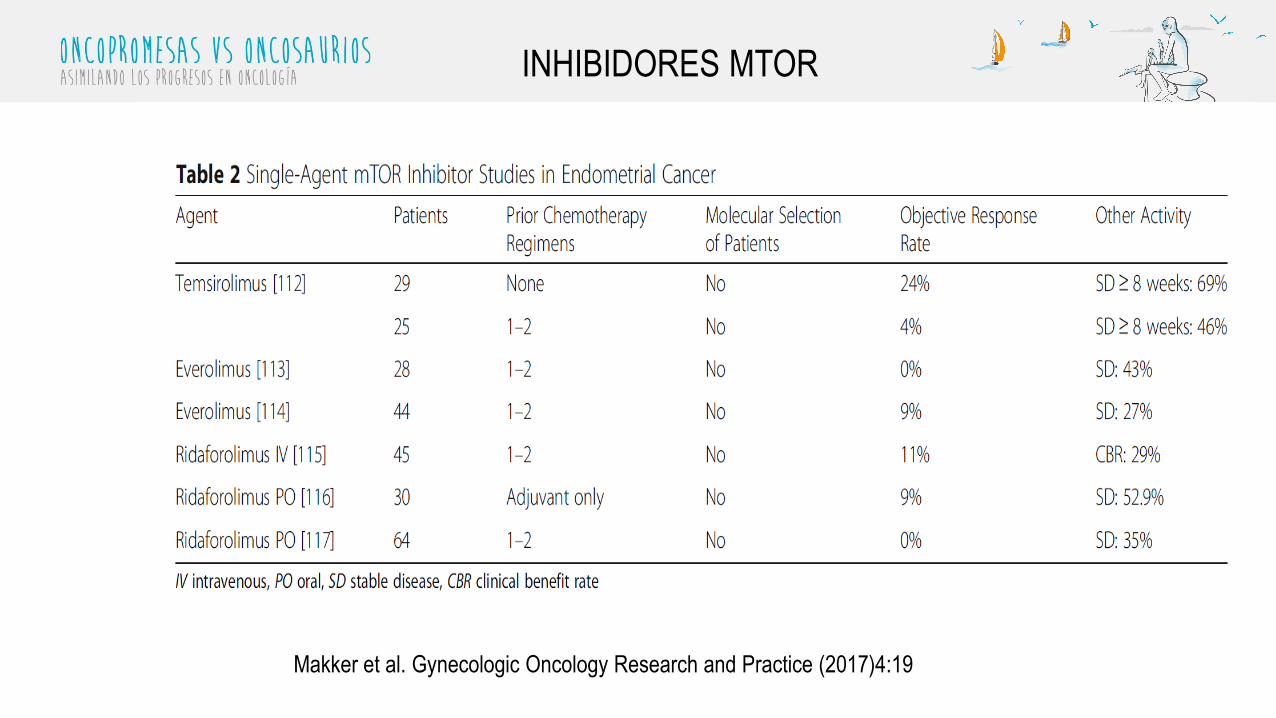
INHIBIDORES MTOR
Makker et al. Gynecologic Oncology Research and Practice (2017)4:19

- Se incluyeron 38 pacientes
- Objetivo → CBR (RC+RP+EE)
- Pacientes fueron tratados
hasta toxicidad, progresion o
RC
- CBR→ 40% (14/35) 9 RC y 2
RP
- Histologia serosa: mejor
predictor de ausencia de
respuesta
COMBINACIONES INHIBIDORES MTOR
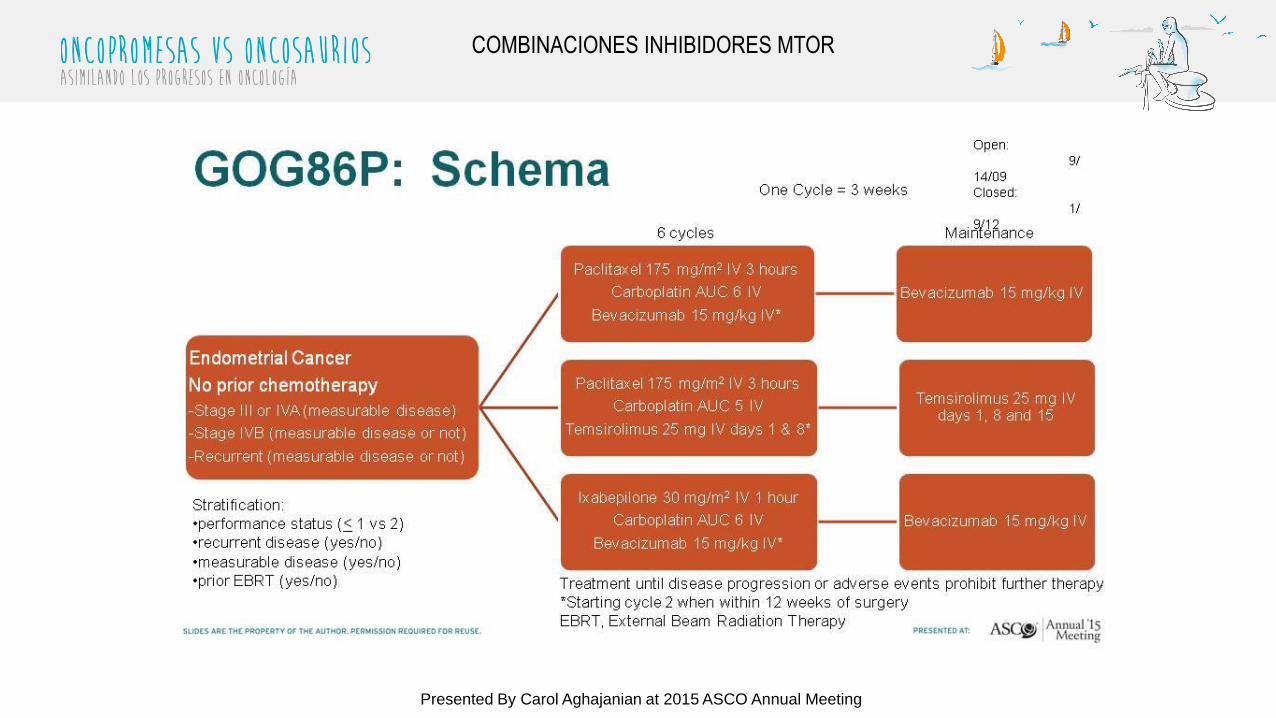
GOG86P: Schema
Presented By Carol Aghajanian at 2015 ASCO Annual Meeting
COMBINACIONES INHIBIDORES MTOR
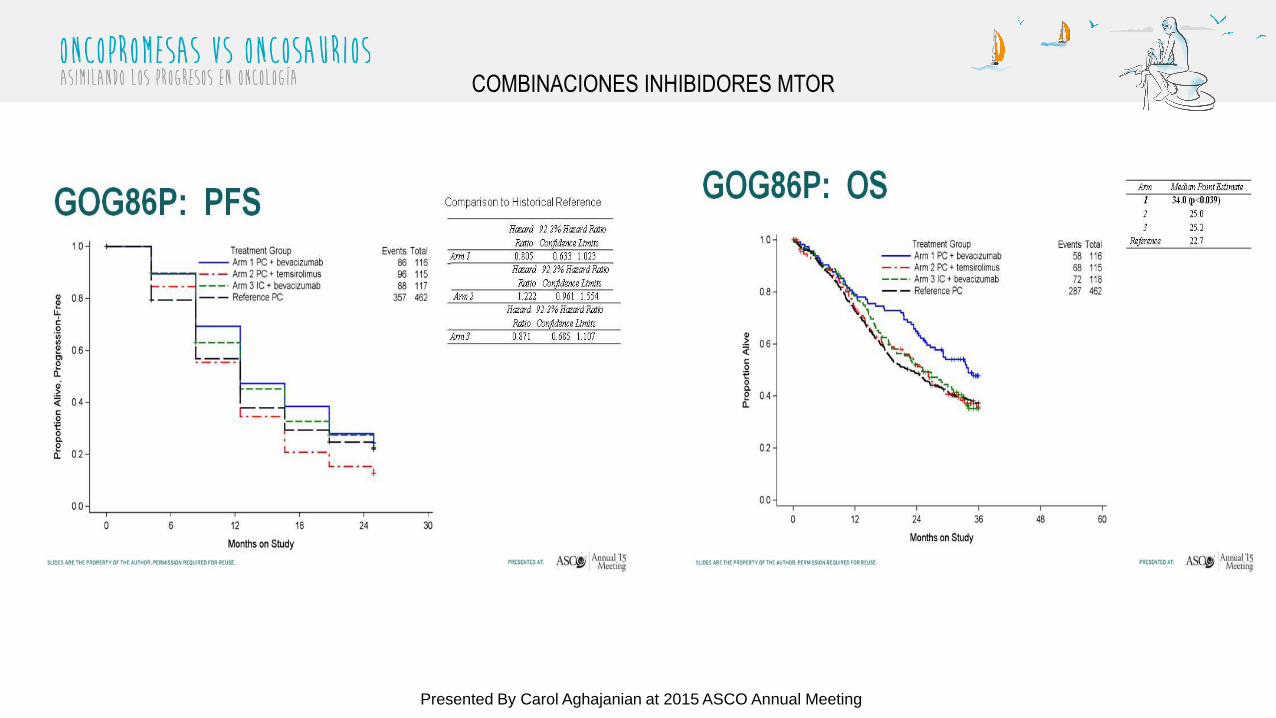
GOG86P: PFS
Presented By Carol Aghajanian at 2015 ASCO Annual Meeting
COMBINACIONES INHIBIDORES MTOR
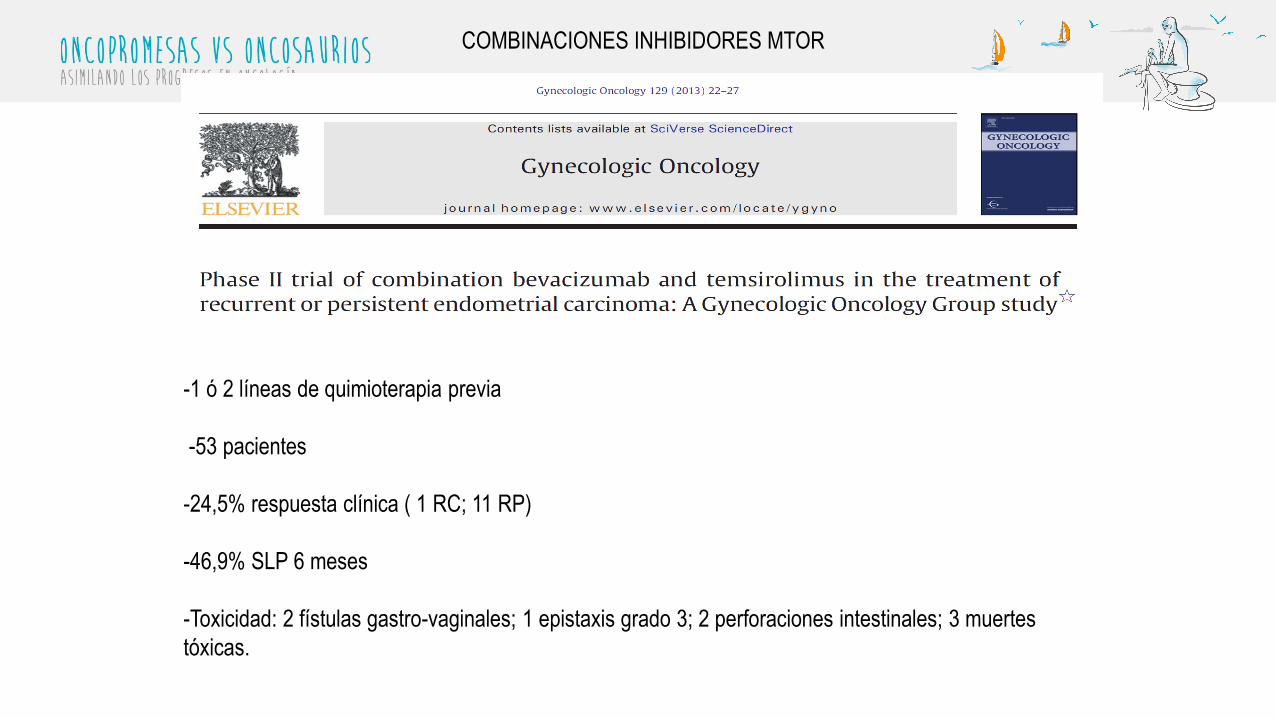
-1 ó 2 líneas de quimioterapia previa
-53 pacientes
-24,5% respuesta clínica ( 1 RC; 11 RP)
-46,9% SLP 6 meses
-Toxicidad: 2 fístulas gastro-vaginales; 1 epistaxis grado 3; 2 perforaciones intestinales; 3 muertes
tóxicas.
COMBINACIONES INHIBIDORES MTOR

• 67 pacientes
• 1 ó 2 líneas previas
• ORR 6%
• PFS>6 meses: 11,9%
• Toxicidad: rash, diarrea, astenia, fundamentalmente grado 1-2
• Favorable perfil de toxicidad, con mínima actividad antitumoral
PAN-INHIBIDOR PI3K
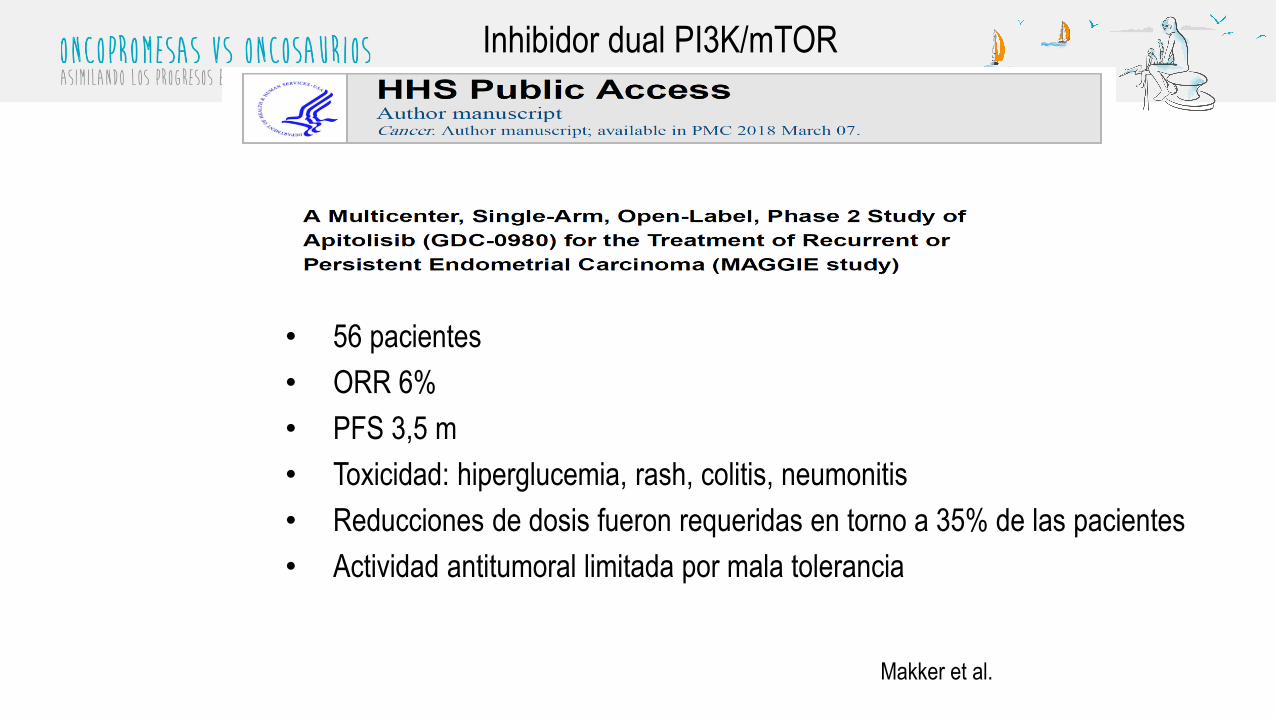
Inhibidor dual PI3K/mTOR
• 56 pacientes
• ORR 6%
• PFS 3,5 m
• Toxicidad: hiperglucemia, rash, colitis, neumonitis
• Reducciones de dosis fueron requeridas en torno a 35% de las pacientes
• Actividad antitumoral limitada por mala tolerancia
Makker et al.
ALTERATIONS IN RECEPTOR TYROSINE KINASES IN
ENDOMETRIAL CANCER
• Papel clave en regular el desarrollo y progresión del cáncer de
endometrio
• EGFR
• FGFR
• IGFR
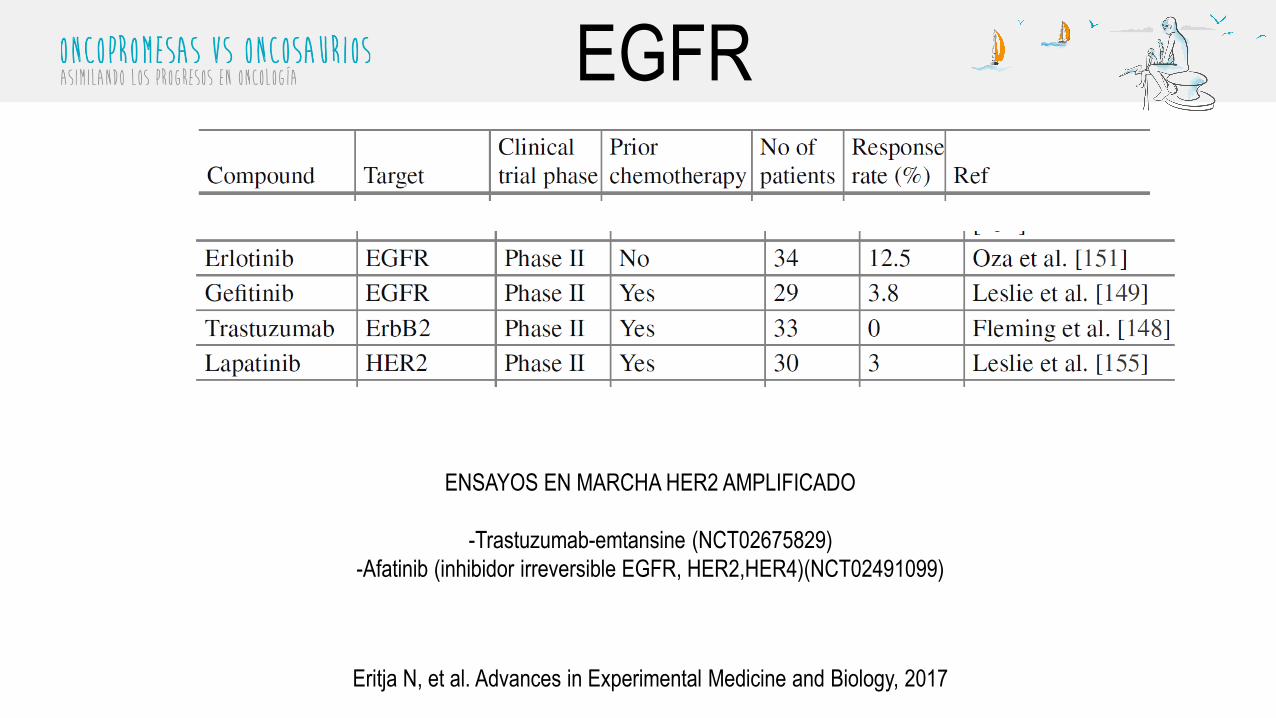
EGFR
ENSAYOS EN MARCHA HER2 AMPLIFICADO
-Trastuzumab-emtansine (NCT02675829)
-Afatinib (inhibidor irreversible EGFR, HER2,HER4)(NCT02491099)
Eritja N, et al. Advances in Experimental Medicine and Biology, 2017

Vía FGFR
Konecki G et al. Lancet 2015
Se han identificado mutaciones de FGFR2 en 10-16% de los
adenocarcinomas de endometrio
• Estudio fase II (2 est Simon) de brazo unico
• Objetivo ppal→ Beneficio clinico (CB)
• 248 pts sometidas a screening → 27 (11%) FGFR2 mutados
• Se tratan 27 FGFR2mut y 31 FGFR2 no mut
• 7 y 9 pts respect libres de recaida a 18 m
• Ninguno de los grupos continúo a stage 2
Konecki G et al. Lancet 2015
DOVITINIB EN SEGUNDA LÍNEA
Cortesia Dr. Andrés Poveda
Phase II study of everolimus, letrozole and metformin in women with advanced/recurrent endometrial cancer
Presented By Pamela Soliman at 2016 ASCO Annual Meeting
Phase II study of everolimus, letrozole, and metformin
in women with advanced/recurrent endometrial cancer.
• Estudio fase II (2 est Simon) de brazo unico
• Objetivo ppal→ Beneficio clinico (CB)
• Biomarcador a explorar → mutacion KRAS
• 58 pacientes incluidos.
• CB ratio 66.7% (32/48)→ 29% RP y 38% EE
• No se aprecian diferencias según status KRAS (73.1% CBR Kras
mut vs 64.3% wt, p=0.72)
• Tox: gastrointesintal (diarrea), anemia, astenia
Soliman PT et al. ASCO 2015
ESTUDIOS EN MARCHA CON METFORMINA
• Paclitaxel and Carboplatin With or Without Metformin Hydrochloride
in Treating Patients With Stage III, IV, or Recurrent Endometrial
Cancer. ClinicalTrials.gov Identifier: NCT02065687– A Randomized Phase II/III Study of Paclitaxel/Carboplatin/Metformin (NSC#91485)
Versus Paclitaxel/Carboplatin/Placebo as Initial Therapy for Measurable Stage III or IVA,
Stage IVB, or Recurrent Endometrial Cancer
• A Phase II, Single-Arm Study of RAD001 (Everolimus), Letrozole, and
Metformin in Patients With Advanced or Recurrent Endometrial
Carcinoma. ClinicalTrials.gov Identifier: NCT01797523
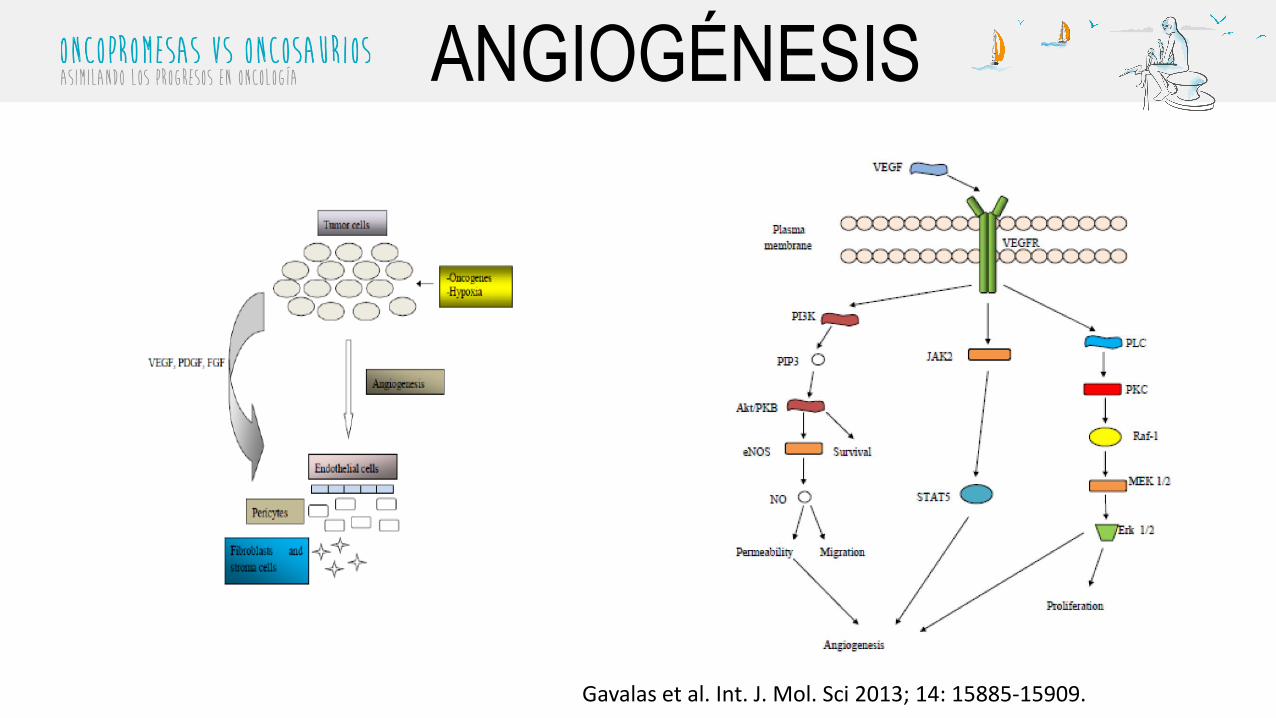
ANGIOGÉNESIS
Gavalas et al. Int. J. Mol. Sci 2013; 14: 15885-15909.
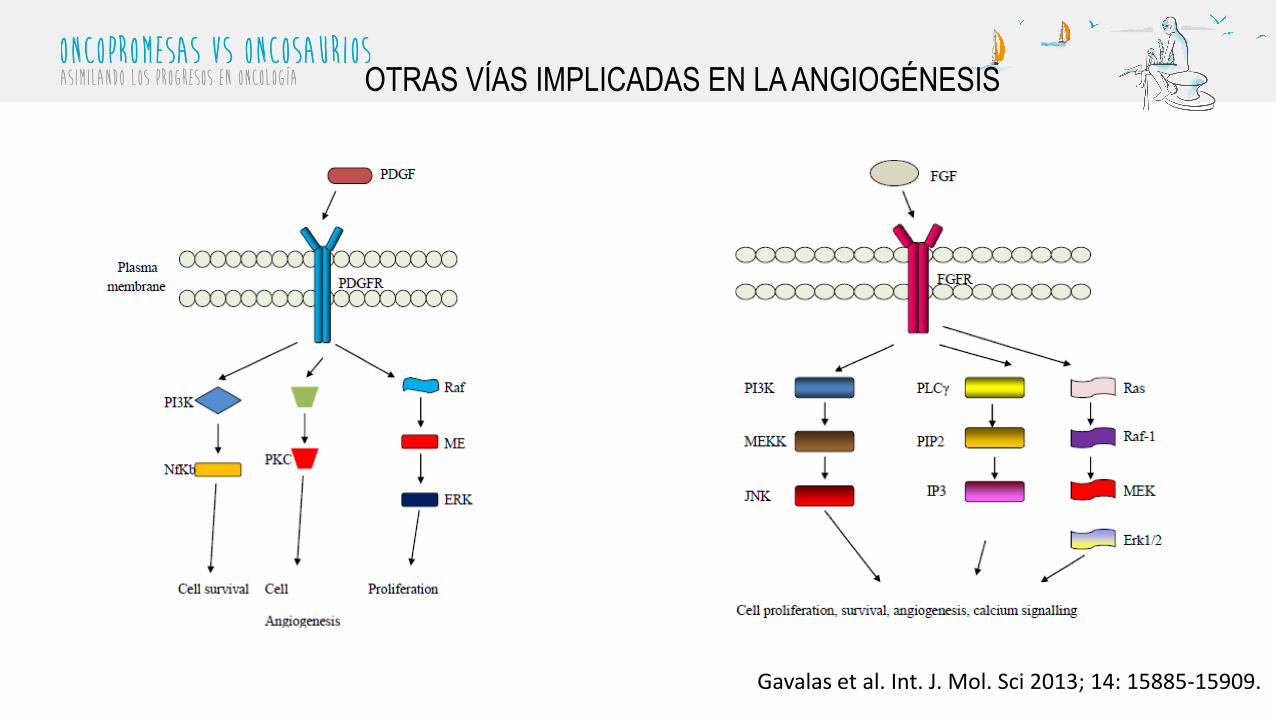
OTRAS VÍAS IMPLICADAS EN LA ANGIOGÉNESIS
Gavalas et al. Int. J. Mol. Sci 2013; 14: 15885-15909.
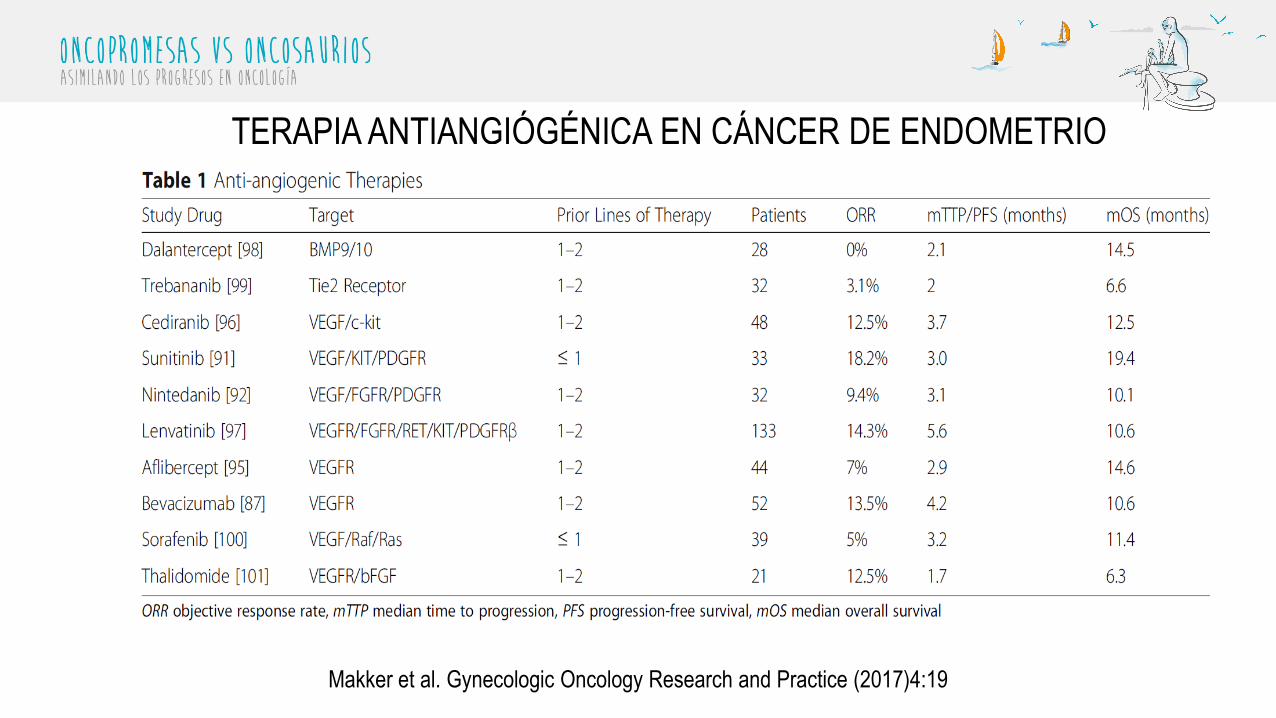
TERAPIA ANTIANGIÓGÉNICA EN CÁNCER DE ENDOMETRIO
Makker et al. Gynecologic Oncology Research and Practice (2017)4:19
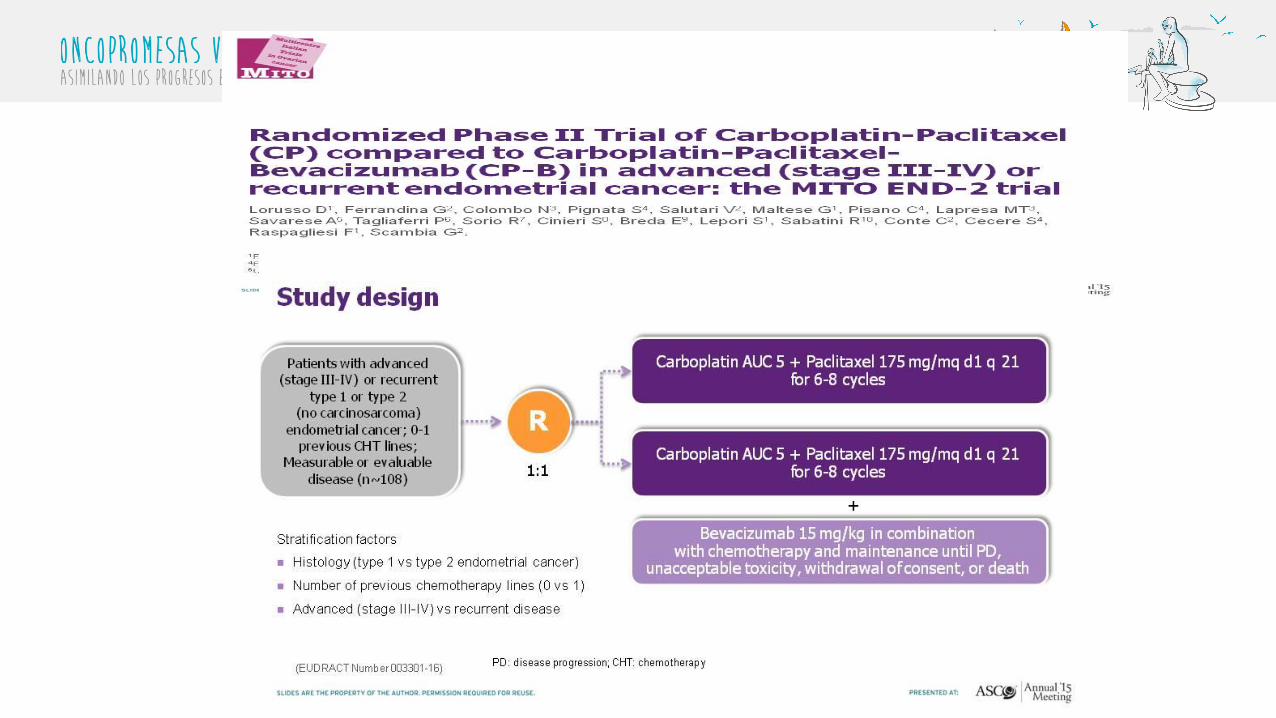
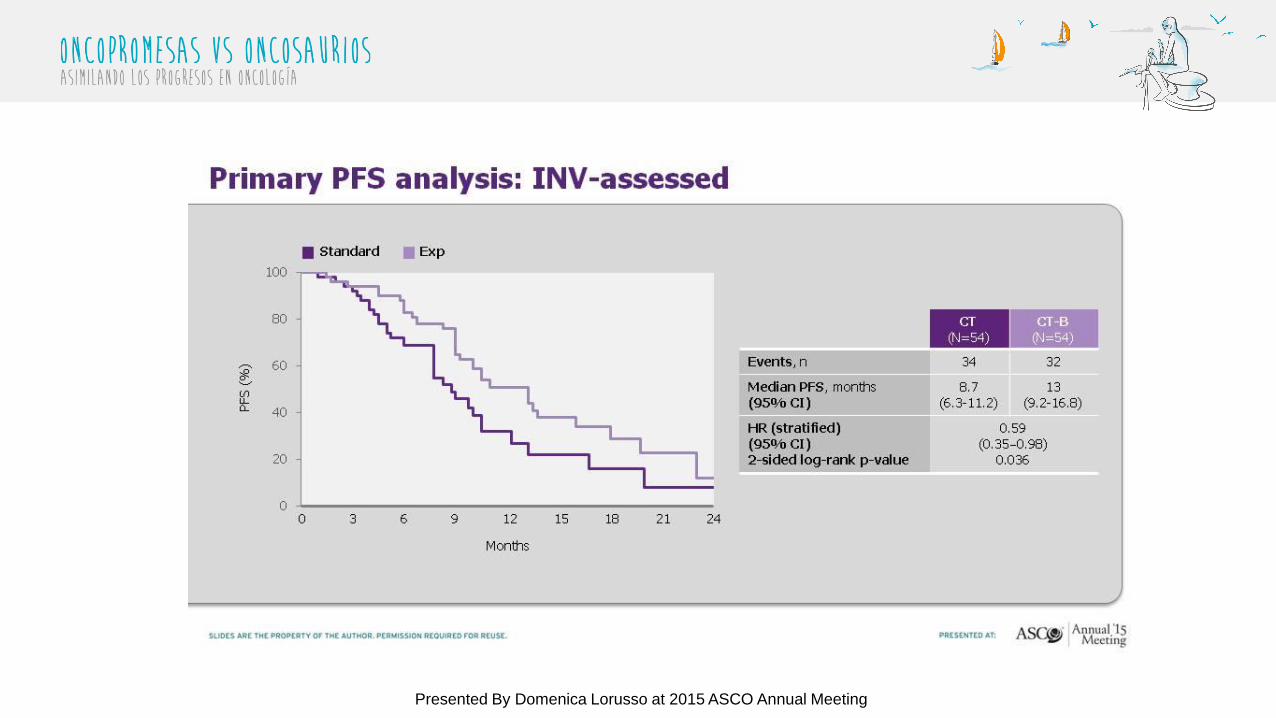
Primary PFS analysis: INV-assessed
Presented By Domenica Lorusso at 2015 ASCO Annual Meeting
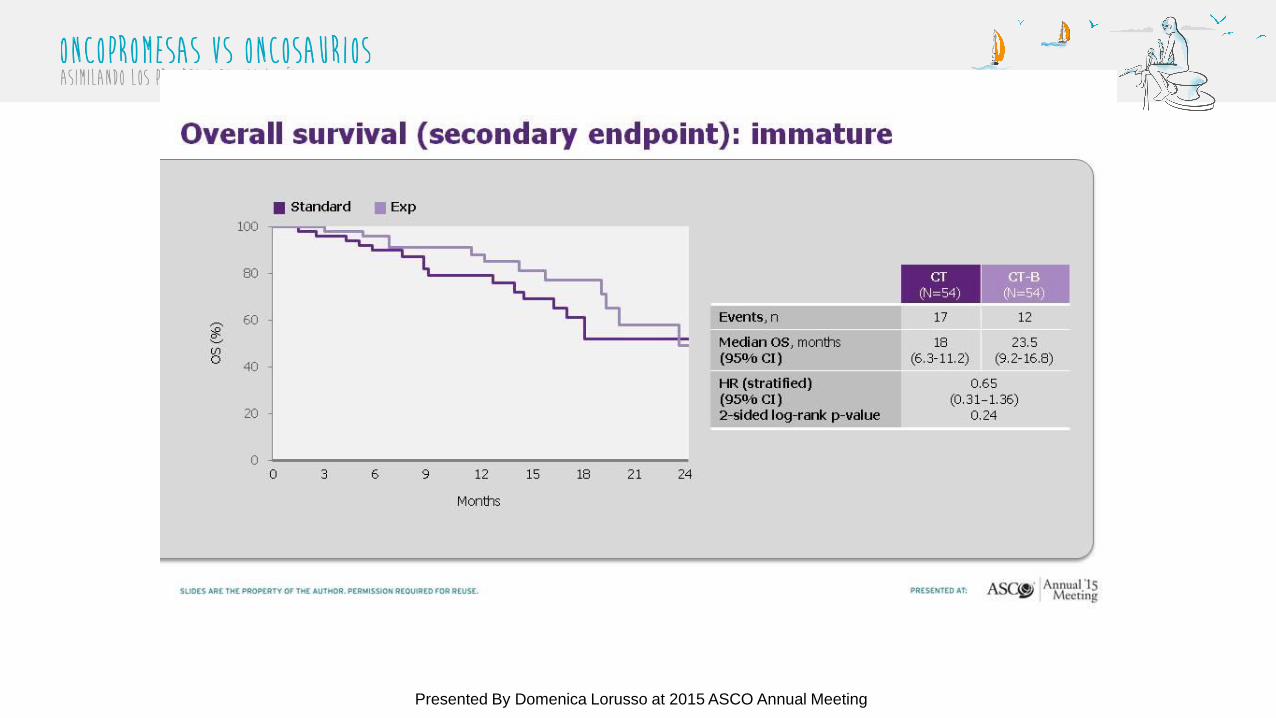
Overall survival (secondary endpoint): immature
Presented By Domenica Lorusso at 2015 ASCO Annual Meeting
• Ca endometrio con 1-2 lineas previas PS0-2
• Objetivo ppal: Rpta + PFS6m(2 est de Simon)
• 49 pacientes incluidos.
• PFS6m 41% (32/48)→ se alcanzo el objetivo preespecificado de PFS6m
(23%)
• Tox: cardiovascular severa (27% gr3-4), 2 muertes tox (perforación GI y
rotura arterial)
Coleman RL et al. Gynecol Oncol 2012
ESTUDIO FASE II AFLIBERCEPT
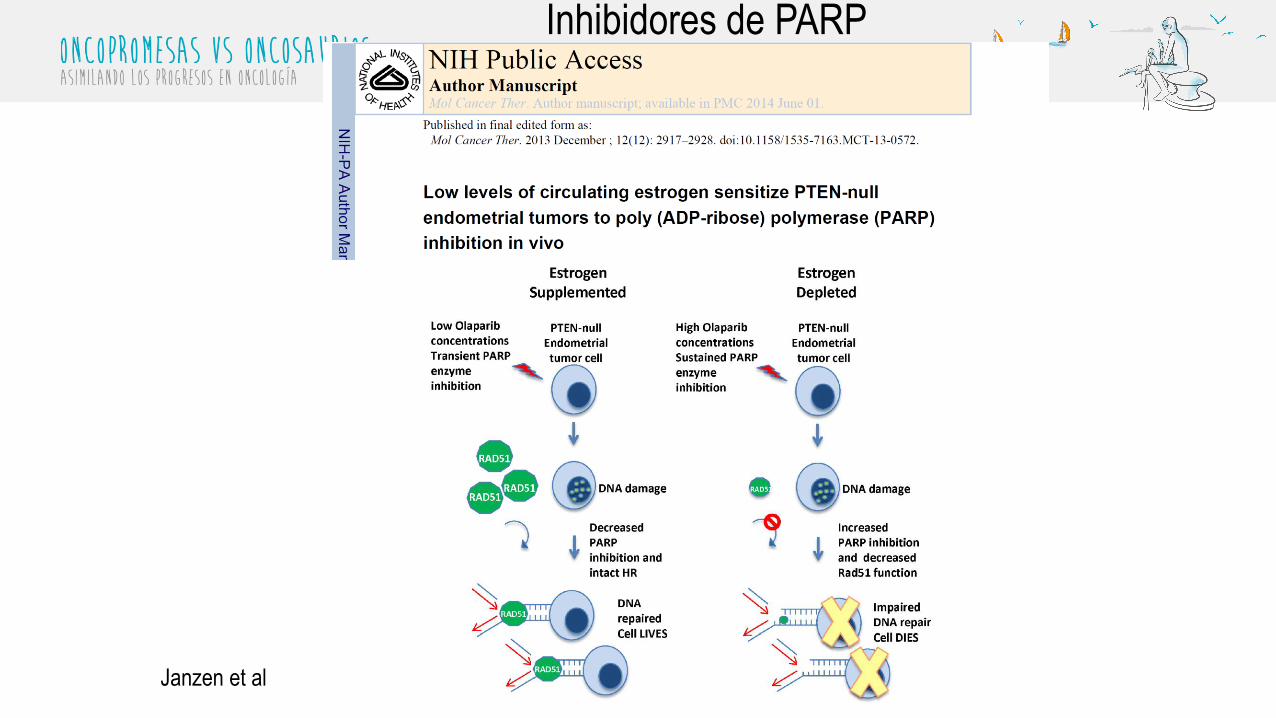
Inhibidores de PARP
Janzen et al
Inhibidores de PARP
• Fase II Niraparib en cáncer de endometrio recurrente
• Fase I :
– Olaparib + AZD2014 ( Inhibidor Mtorc1/2)
– Olaparib + AZD5363 (Inhibidor AKT)
iPARP + Inh. mTORC1y2
Phase I trial of olaparib (PARP inhibitor) and
vistusertib (mTORC1/2 inhibitor) in recurrent
endometrial, ovarian and triple negative breast
cancer.
2018 ASCO Annual Meeting!
-Combinación bien tolerada
-RR ca endometrio: 27-30%
-67% de pacientes respondedores presentaron mutaciones en PI3K, ARID1A y
FBXW7
-Respuestas prometedoras en ambas histologias: endometrioide y seroso.
Inmunoterapia
• PD-1 y PDL-1 se encuentran sobreexpresados entre el 60-80% de los tumores primarios
de endometrio y en el 100% de los tumores metastásicos.
• La alta carga mutacional en el subtipo POLE ultramutado y en el subtipo con
inestabilidad de microsatélites hipermutado, se correlaciona con la expresión de PD-1.
• Aproximadamente el 26% de las recaídas de cáncer de endometrio presentan estos dos
subtipos, con lo que se convierten en excelente candidatas para la terapia anti PD-1.
• En el resto de variantes, hay que buscar fármacos más dirigidos y estrategias de
combinación.

INMUNOTERAPIA• Pembrolizumab:
– En pacientes con cáncer colorrectal: 78% immune related PFS en MMR-deficient
cancer and 11% in MMR-proficient
– MMR status predice beneficio clínico de pembrolizumab
– 13% de respuestas parciales en cáncer de endometrio con PDL-1>1%.
• Lenvatinib:
– Disminuye significativamente los macrófagos asociados a tumor
– Aumento de la actividad antitumoral y de la upregulación de los inhibidores de PD-
1.
– Estudio fase IB/II de la combinación de Lenvatinib con Pembrolizumab en marcha:
ORR 24w: 50%. ASCO 2018. Actividad en MMR-D y P.
ESTUDIOS EN MARCHA INMUNOTERAPIA: MONOTERAPIA
• Study of Pembrolizumab (MK-3475) in Participants With Advanced Solid Tumors (MK-3475-158/KEYNOTE-158) ClinicalTrials.gov Identifier: NCT02628067
• Inclusion Criteria:
• Histologically or cytologically-documented, advanced solid tumor of one of the following types:
– Endometrial Carcinoma (sarcomas and mesenchymal tumors are excluded)
– Cervical Squamous Cell Carcinoma
– Vulvar Squamous Cell Carcinoma
– Any advanced solid tumor, with the exception of colorectal carcinoma (CRC), which is MicrosatelliteInstability (MSI)-High (MSI-H)
• Progression of tumor or intolerance to therapies known to provide clinical benefit. There is no limit to the numberof prior treatment regimens
• Pembrolizumab in Ultramutated and Hypermutated Endometrial Cancer. ClinicalTrials.gov Identifier: NCT02899793
• Inclusion Criteria:
• Patients must have histologically confirmed endometrial cancer that is recurrent or progressive following at leastone prior chemotherapy regimen.
• Patients with the following histologic epithelial cell types are eligible: Endometrioid adenocarcinoma, serousadenocarcinoma, clear cell carcinoma, undifferentiated carcinoma, mixed epithelial carcinoma, carcinosarcoma, and adenocarcinoma not otherwise specified (N.O.S.).
• Tumors must demonstrate ultramutation (POLE-mutation) and/or hyper-mutation (due to MMR gene defect) in a representative primary or metastatic tumor site by next generation sequencing (NGS) and ComprehensiveGenomic Profiling (CGP) testing.

ESTUDIOS EN MARCHA INMUNOTERAPIA: MONOTERAPIA
• MK-3475 Immunotherapy in Endometrial Carcinoma. ClinicalTrials.gov Identifier: NCT02630823
Study DescriptionDue to the high expression of PD-L1 in endometrial cancers as well as in ovarian cancers which are molecularly similar to uterine serous cancers, using pembrolizumab
should be beneficial in this patient population. Since the investigators are able to get a pre-treatment research- related endometrial biopsy as well as the surgical
specimen post two cycles of pembrolizumab, the investigators will be able to evaluate the mechanism of action of this drug on the endometrial cancer tumor
environment.
•Experimental: Arm 1: MK-3475
•Patients will undergo endometrial biopsy followed by 2 doses of MK-3475 3 weeks apart. 3-4 weeks after the
second dose of MK-3475, the standard of care surgical resection will take place, followed by standard of care
adjuvant therapy. Tissue and blood will be collected at the time of surgical resection for immune analysis. For
patients whose pathology confirms high-risk features and advanced stage, MK-3475 will be given every 3 weeks
starting 4 -6 weeks after completion of adjuvant therapy for a maximum of 4 doses post-surgery.
•MK-3475 will be given intravenously at a dose of 200 mg over the course of 30 minutes.
•The standard of care chemotherapy will consist of 6 cycles of paclitaxel and carboplatin AUC 5 every 3 weeks for
6 cycles.
•The decision to administer radiation therapy will be per the treating physician. If the patient does not receive
radiation therapy, then the patient will start MK-3475 every 3 weeks x 4 doses after the completion of
chemotherapy.
ESTUDIOS EN MARCHA INMUNOTERAPIA: MONOTERAPIA
• Study of Avelumab in Patients With MSS, MSI-H and POLE-mutated Recurrent or Persistent Endometrial Cancer.
ClinicalTrials.gov Identifier: NCT02912572
• Inclusion Criteria:
• -Participants must be classified into one of two cohorts of recurrent or persistent endometrial cancer of any histology:
• --The first cohort (MSI/POLE cohort) includes endometrial cancers that are: MSI-H as determined by immunohistochemical
complete loss of expression (absence of nuclear immunoreactivity) of at least one of the mismatch repair genes MSH2, MSH6,
MLH1 and PMS2. This test is now done routinely for every newly diagnosed endometrial cancer patient in most centers in the
US.
• And/OR:
• POLE-mutated, i.e. endometrial cancers known to harbor mutations in the exonuclease domain (amino acid residues 268-471)
of polymerase e (POLE) as determined by targeted sequencing or other next generation sequencing assay. Any Clinical
Laboratory Improvement Amendments (CLIA)-approved genomic test documenting mutations in the exonuclease domain of
POLE gene (amino acid residues 268-471) in the tumor will be accepted as proof of presence of POLE mutations and will lead
to classification into this patient cohort.
• The second cohort (MSS cohort) includes:
• Endometrial cancers that are MSS as determined by normal immunohistochemical nuclear expression of all the mismatch repair
genes MSH2, MSH6, MLH1 and PMS2. Tumors which have not been sequenced for POLE mutations (i.e. their POLE mutations
status is unknown) but are MSS, will be included in this cohort.
• All patients must have measurable disease as defined by RECIST 1.1. Measurable disease is defined as at least one lesion that
can be accurately measured in at least one dimension (longest diameter to be recorded). Each lesion must be >= 10 mm when
measured by CT, MRI or caliper measurement by clinical exam; or >= 20 mm when measured by chest x-ray. Lymph nodes
must be > 15 mm in short axis when measured by CT or MRI.
ESTUDIOS EN MARCHA INMUNOTERAPIA: COMBINACIONES
• A Study of Durvalumab With or Without Tremelimumab in Endometrial Cancer.
ClinicalTrials.gov Identifier: NCT03015129
• A Phase 2 Trial of Durvalumab [MEDI4736](Anti-PD-L1 Antibody) With or Without Tremelimumab
(Anti-CTLA-4 Antibody) in Patients With Persistent or Recurrent Endometrial Carcinoma and
Endometrial Carcinosarcoma
• Inclusion Criteria:
• Subjects must have recurrent or persistent endometrial carcinoma (including: Endometrioid
adenocarcinoma, serous adenocarcinoma, undifferentiated carcinoma, dedifferentiated carcinoma,
clear cell adenocarcinoma, mixed epithelial carcinoma, adenocarcinoma not otherwise specified
(N.O.S.), mucinous adenocarcinoma, squamous cell carcinoma, and transitional cell carcinoma) or
endometrial carcinosarcoma). Histologic documentation of diagnosis of carcinoma is required
• Pembro/Carbo/Taxol in Endometrial Cancer. ClinicalTrials.gov Identifier: NCT02549209
• Phase II Study of Pembrolizumab in Combination With Carboplatin and Paclitaxel for Advanced or
Recurrent Endometrial Adenocarcinoma
OTRAS VÍAS MOLECULARES
• RAS-RAF-MEK-ERK Signaling pathway:– Mutaciones en RAS-RAF.
– Inhibidores de RAF y MEK: Limitada actividad terapéutica en monoterapia.
– Combinaciones con inhibores de PI3K/AKT/mtor, actividad en modelos preclínicos en cáncer de endometrio.
• WNT/ Beta-Catenin– Ruta de mucha complejidad: múltiples isoformas de ligandos y receptores
– Fase inicial de la tumorogénesis: diferenciación irreversible que no responde a inhibición de WNT
– Estudios en fases muy iniciales
• Ciclo celular:– Mutaciones p53
– Sobreexpresión de determinadas ciclinas y CDK: asociación con estadios más avanzados, tumores menos diferenciados, menor expresión del receptor de estrógeno.
– Aurora Kinasa A
• TGF-BETA:– Papel en la transformación neoplásica del cáncer de endometrio
– Potencial nueva diana: estudios preclínicos
CONCLUSIONES• La nueva clasificación que integra elementos morfológicos, moleculares y biológicos derivada
del TCGA, ha permitido determinar las principales rutas alteradas donde dirigir el desarrollo de nuevos fármacos.
• Los estudios con inhibidores de PI3K-AKT-mtor han tenido pocos resultados clínicos y necesitan ser dirigidos por estudio de mutaciones así como utilizando estrategias de combinación.
• Los estudios con inhibidores tirosin-quinasa precisan una mejor selección de los paciente,conmuestras enriquecidas y utilizando combinaciones.
• La inactiviación de la angiogénesis presenta actividad y parece una vía prometedora, estudios más avanzados con bevacizumab.
• Necesidad de nuevos biomarcadores para clarificar el papel de cada vía y las mutaciones más relevantes, así como estudiar posibles mecanismos de resistencia.


















