Prasugrel y ticagrelor en el SCA - Sociedad Española...
37
Prasugrel y ticagrelor en el SCA José A. Barrabés Unidad Coronaria Servicio de Cardiología Hospital Universitario Vall d’Hebron Barcelona Curso Casa del Corazón Madrid 15 junio 2012
Transcript of Prasugrel y ticagrelor en el SCA - Sociedad Española...

Prasugrel y ticagrelor
en el SCA
José A. Barrabés
Unidad Coronaria Servicio de Cardiología
Hospital Universitario Vall d’Hebron
Barcelona
Curso Casa del Corazón
Madrid
15 junio 2012
Conflicto de intereses:
Honorarios (modestos) por consultoría y/o charlas de: ASTRA-ZENECA,
BAYER, BMS, CHIESI, DAIICHI-SANKYO, URIACH
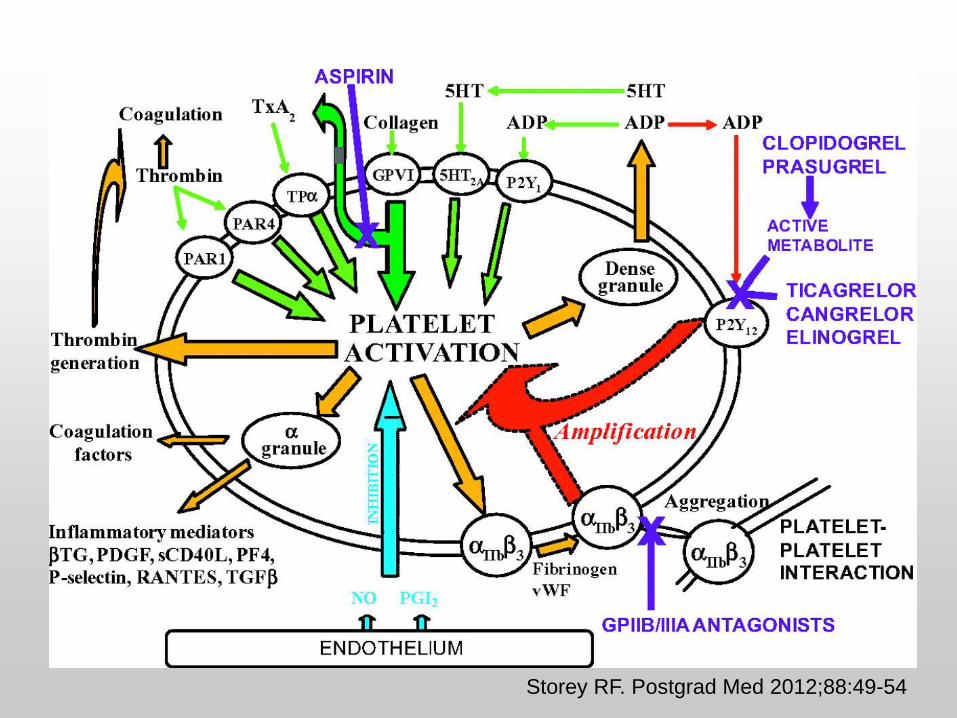
Storey RF. Postgrad Med 2012;88:49-54
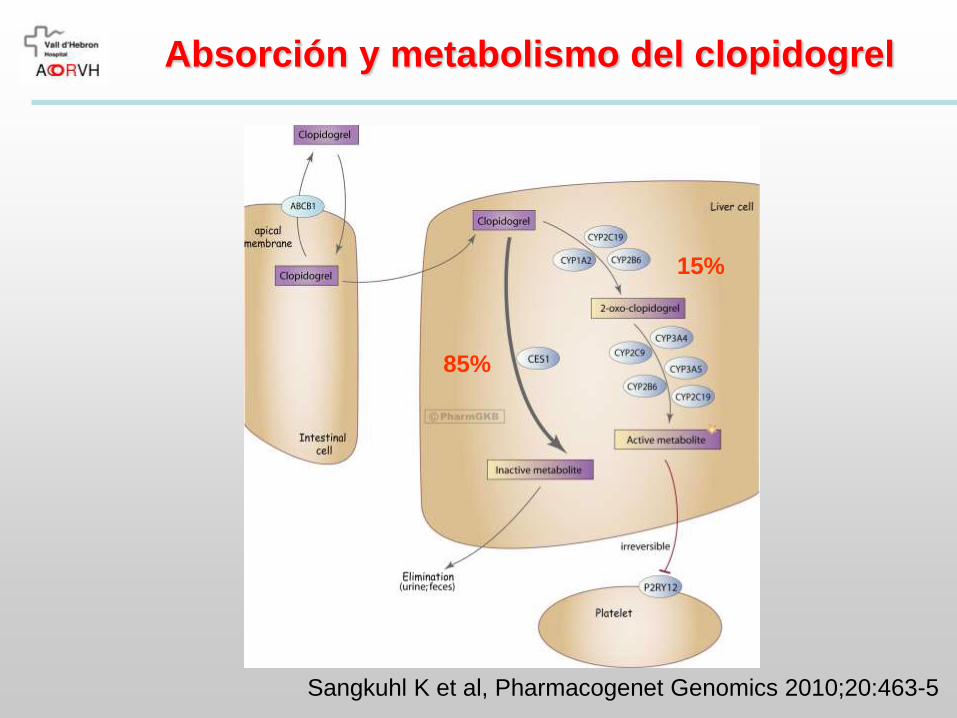
Sangkuhl K et al, Pharmacogenet Genomics 2010;20:463-5
Absorción y metabolismo del clopidogrel
85%
15%
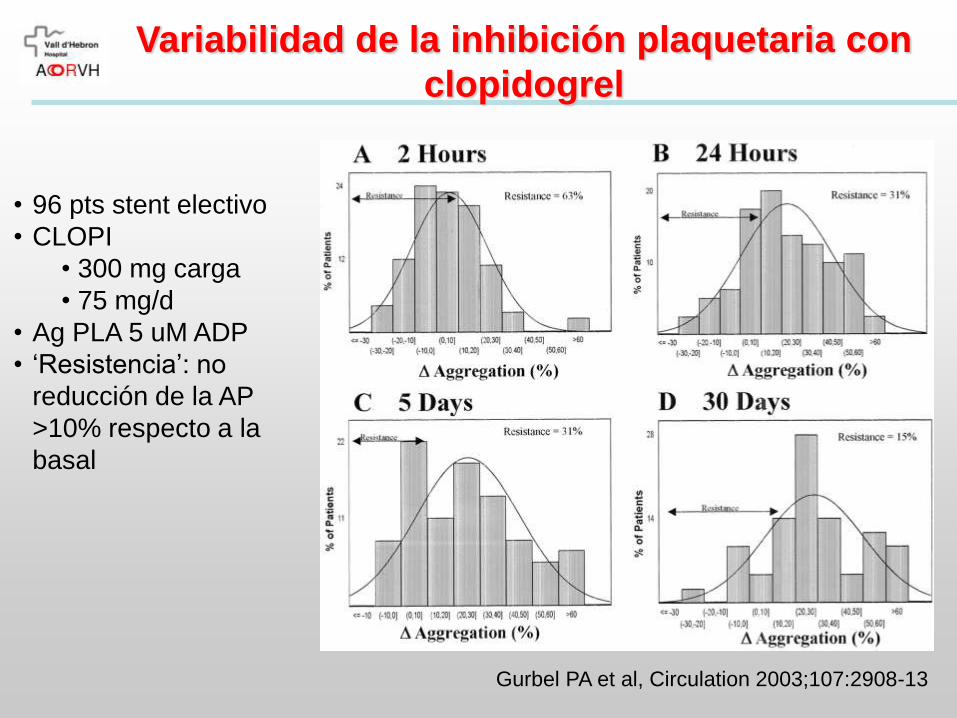
Variabilidad de la inhibición plaquetaria con
clopidogrel
Gurbel PA et al, Circulation 2003;107:2908-13
• 96 pts stent electivo
• CLOPI
• 300 mg carga
• 75 mg/d
• Ag PLA 5 uM ADP
• ‘Resistencia’: no
reducción de la AP
>10% respecto a la
basal
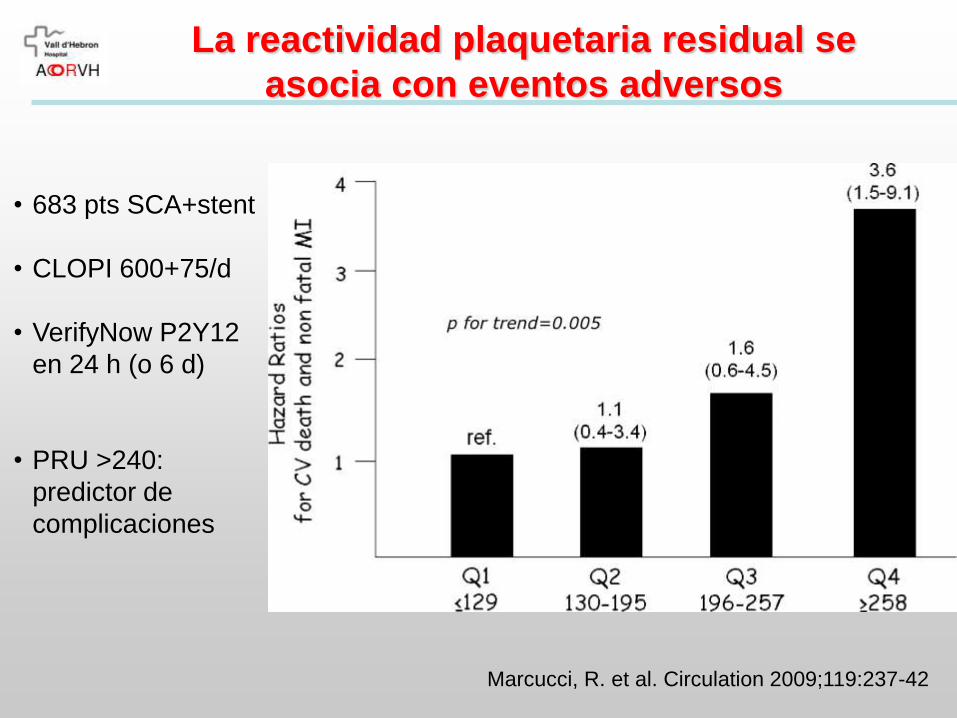
La reactividad plaquetaria residual se
asocia con eventos adversos
Marcucci, R. et al. Circulation 2009;119:237-42
• 683 pts SCA+stent
• CLOPI 600+75/d
• VerifyNow P2Y12
en 24 h (o 6 d)
• PRU >240:
predictor de
complicaciones
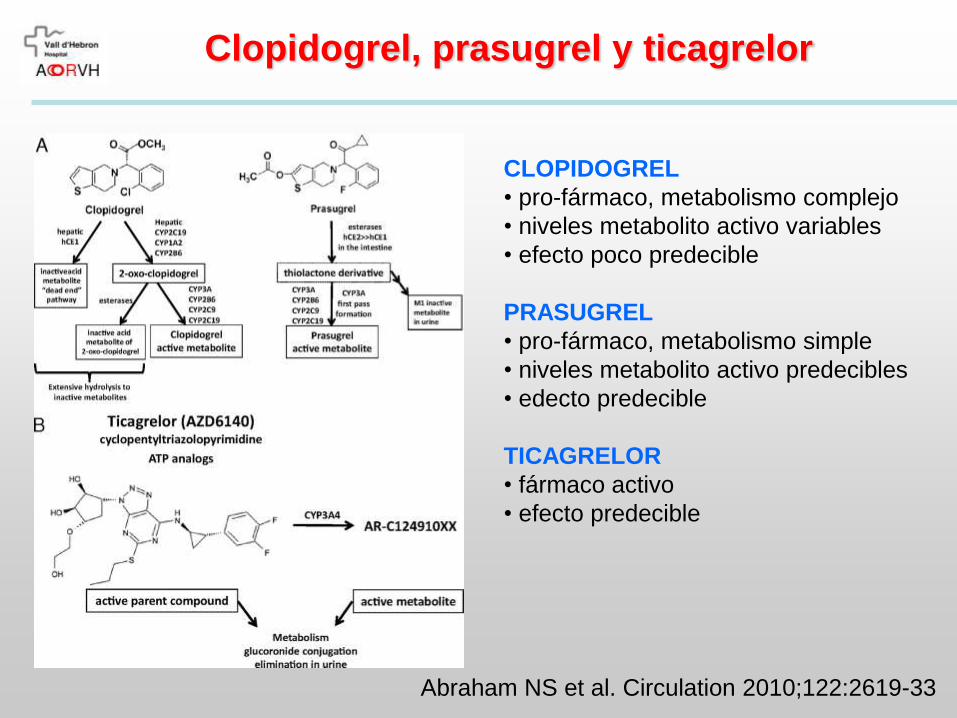
Clopidogrel, prasugrel y ticagrelor
Abraham NS et al. Circulation 2010;122:2619-33
CLOPIDOGREL
• pro-fármaco, metabolismo complejo
• niveles metabolito activo variables
• efecto poco predecible
PRASUGREL
• pro-fármaco, metabolismo simple
• niveles metabolito activo predecibles
• edecto predecible
TICAGRELOR
• fármaco activo
• efecto predecible

Clopidogrel, prasugrel y ticagrelor
CLOPIDOGREL
• irreversible
• administración c/24 h
PRASUGREL
• irreversible
• administración c/24 h
TICAGRELOR
• reversible
• administración c/12 h
Husted S and van Giezen JJ. Cardiovasc Ther 2009
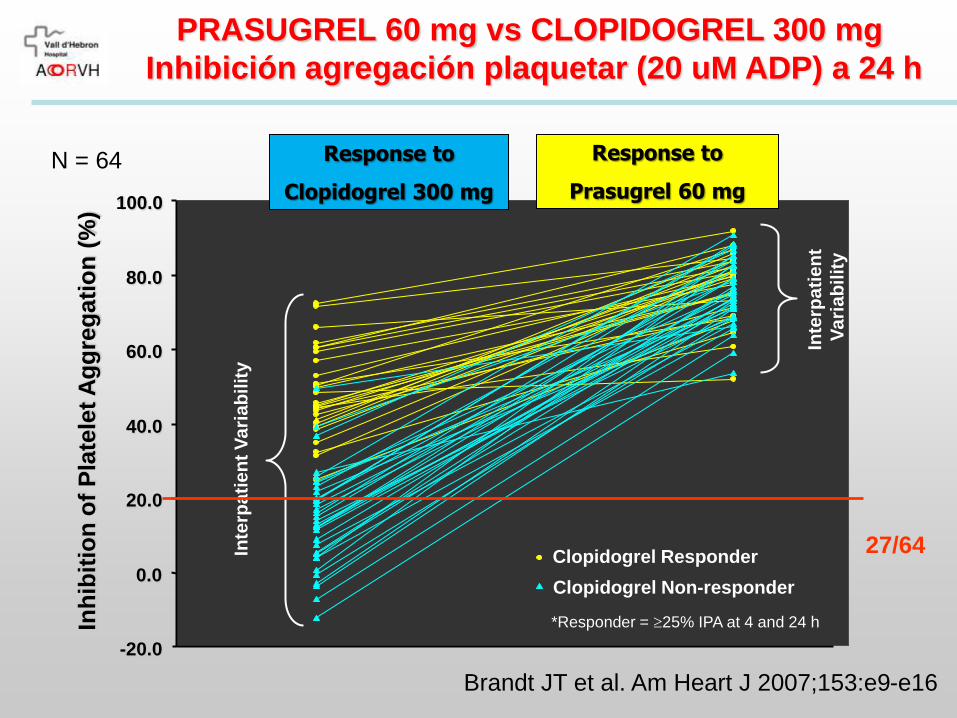
PRASUGREL 60 mg vs CLOPIDOGREL 300 mg
Inhibición agregación plaquetar (20 uM ADP) a 24 h
Brandt JT et al. Am Heart J 2007;153:e9-e16
-20.0
0.0
20.0
40.0
60.0
80.0
100.0
Inh
ibit
ion
of
Pla
tele
t A
gg
reg
ati
on
(%
)
Response to
Prasugrel 60 mg
Response to
Clopidogrel 300 mg
Clopidogrel Responder
Clopidogrel Non-responder
*Responder = 25% IPA at 4 and 24 h
Inte
rpa
tie
nt
Va
ria
bilit
y
Inte
rpa
tie
nt
Vari
ab
ilit
y
N = 64
27/64

PRASUGREL 60 mg vs CLOPIDOGREL 600 mg
Inhibición agregación plaquetar (20 uM ADP)
Wiviott SD et al. Circulation 2007;116:2923-32
IPA (%; 20 M ADP) IPA (%; 20 M ADP)
Hours 14 Days
0 4 8 12 16 20 24 28 Clopidogrel
150 mg
Prasugrel
10 mg
p<0.0001
45.4
61.9
Clopidogrel 600 mg 32.6
69.3
Prasugrel 60 mg
p<0.0001 for each N=201
74.8
64.5
30.8
31.8
20.3
4.9
0
20
40
60
80
100
0
20
40
60
80
100
PRINCIPLE-TIMI 44 Study

PRASUGREL 60/10 mg vs CLOPIDOGREL 600/75 mg
Efecto de añadir el metabolito activo
Wallentin L et al. Eur Heart J 2008;29:21-30
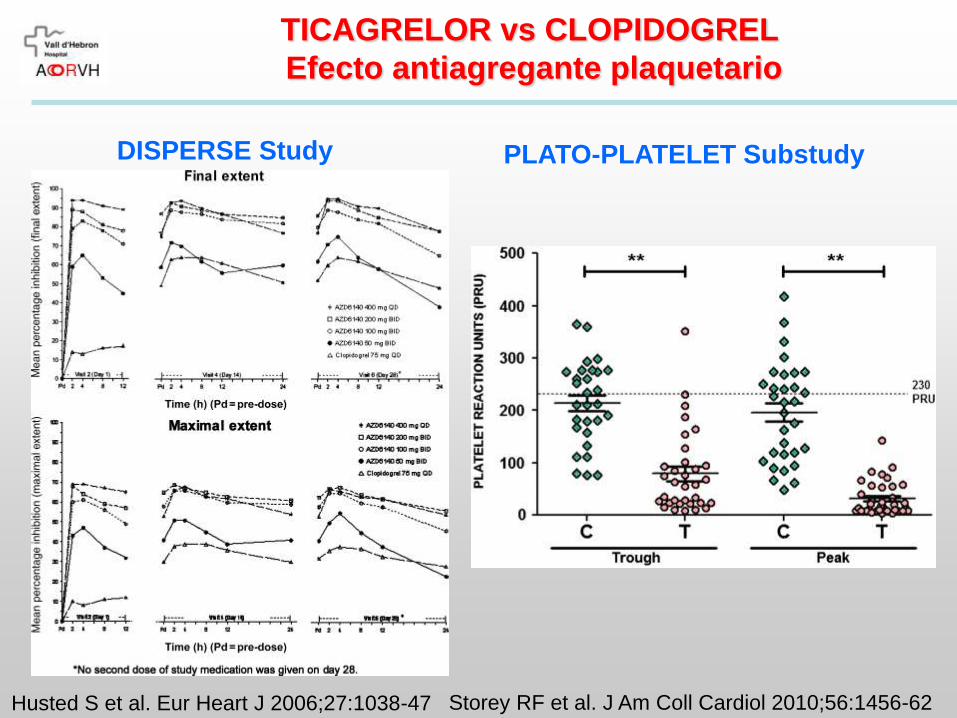
TICAGRELOR vs CLOPIDOGREL
Efecto antiagregante plaquetario
Storey RF et al. J Am Coll Cardiol 2010;56:1456-62 Husted S et al. Eur Heart J 2006;27:1038-47
DISPERSE Study PLATO-PLATELET Substudy
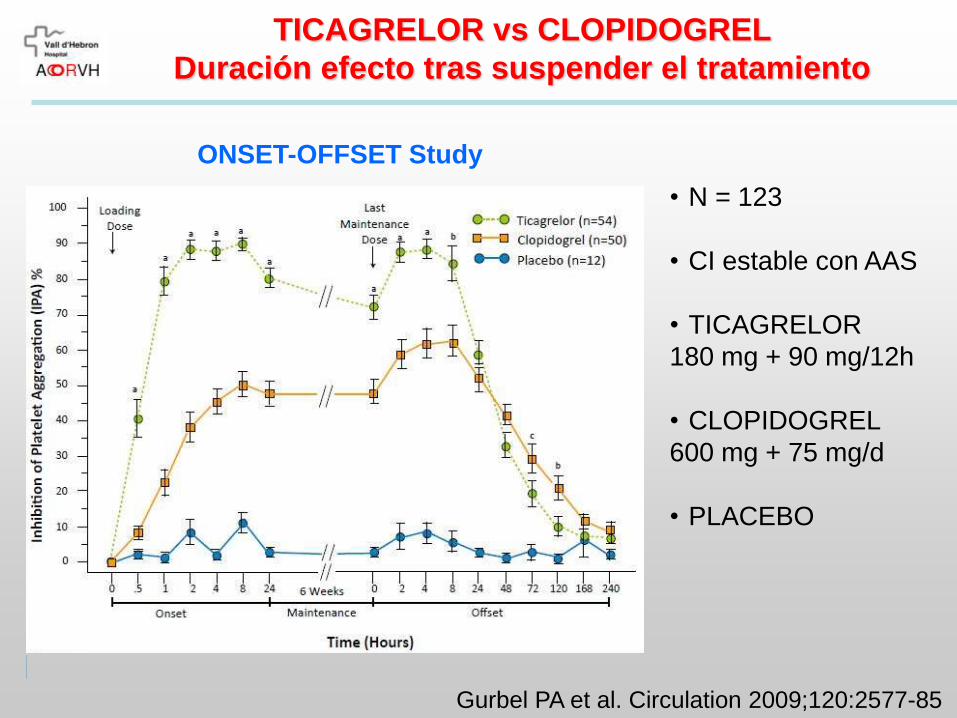
TICAGRELOR vs CLOPIDOGREL
Duración efecto tras suspender el tratamiento
ONSET-OFFSET Study
Gurbel PA et al. Circulation 2009;120:2577-85
• N = 123
• CI estable con AAS
• TICAGRELOR
180 mg + 90 mg/12h
• CLOPIDOGREL
600 mg + 75 mg/d
• PLACEBO

PRASUGREL vs CLOPIDOGREL en SCA
tratado con ICP: TRITON-TIMI 38 Study
Wiviott SD et al. Am Heart J 2006;152:627-35 Wiviott SD et al. N Engl J Med 2007;357:2001-15

PRASUGREL 60/10 vs CLOPIDOGREL 300/75 en SCA
tratado con ICP: TRITON-TIMI 38 Study
138 events
HR 0.81
(0.73-0.90)
p<0.001
NNT=46
35 events
HR 1.32
(1.03-1.68)
p=0.03
NNH=167
Endpoin
t (%
)
0 270 360 450
Days
90
9.9
12.1
30 180 60
1.8
2.4
TIMI Major
NonCABG Bleeds
CV Death / MI / Stroke
Prasugrel
Clopidogrel
0
5
10
15
Wiviott SD et al. New Engl J Med 2007;357:2001-15

TRITON-TIMI 38 Study: Efficacy end points
Wiviott SD et al. New Engl J Med 2007;357:2001-15
0
2
4
6
8
10
12
14
CVD
/MI/C
VA
CV d
eath
Non
fata
l MI
Non
fata
l CVA
Dea
th
Urg
ent T
VR
Ste
nt thr
ombo
sis
Clopidogrel Prasugrel
%
P<0.001
P<0.001
P<0.001
P<0.001 P=NS P=NS
P=NS

TRITON-TIMI 38 Study: Bleeding end points
Wiviott SD et al. New Engl J Med 2007;357:2001-15
P=0.01
P=0.002
P=0.03
P=NS
1,8
0,10,3
3,8
2,4
1,4
0,4 0,3
5
0,9
0
1
2
3
4
5
6
TIMI major Life
threatening
Fatal ICH TIMI
major/minor
Clopidogrel Prasugrel
%
%
Non-CABG-related CABG-related
P<0.001
P=0.002
ICH in pts w/ previous stroke/TIA (n=518):
0 vs 2.3% (P=0.02)

TRITON-TIMI 38 Study: Timing of benefit
Wiviott SD et al. New Engl J Med 2007;357:2001-15

TRITON-TIMI 38 Study:
Subgroup analysis
Wiviott SD et al. New Engl J Med 2007;357:2001-15

TRITON-TIMI 38 Study
Subgroup analysis by bleeding risk
Wiviott SD et al. New Engl J Med 2007;357:2001-15

TRITON-TIMI 38 Study
STEMI cohort
Montalescot G et al. Lancet 2009;373:723-31
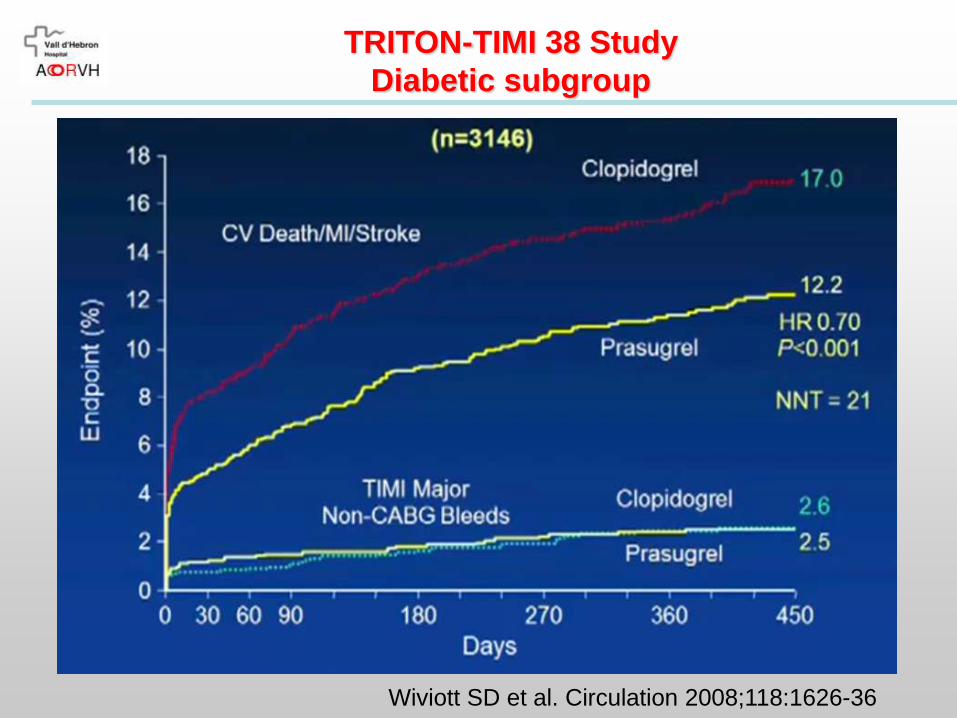
TRITON-TIMI 38 Study
Diabetic subgroup
Wiviott SD et al. Circulation 2008;118:1626-36

Prasugrel en pacientes no seleccionados con ACS
Wiviott SD et al. Circulation 2008;118:1626-36
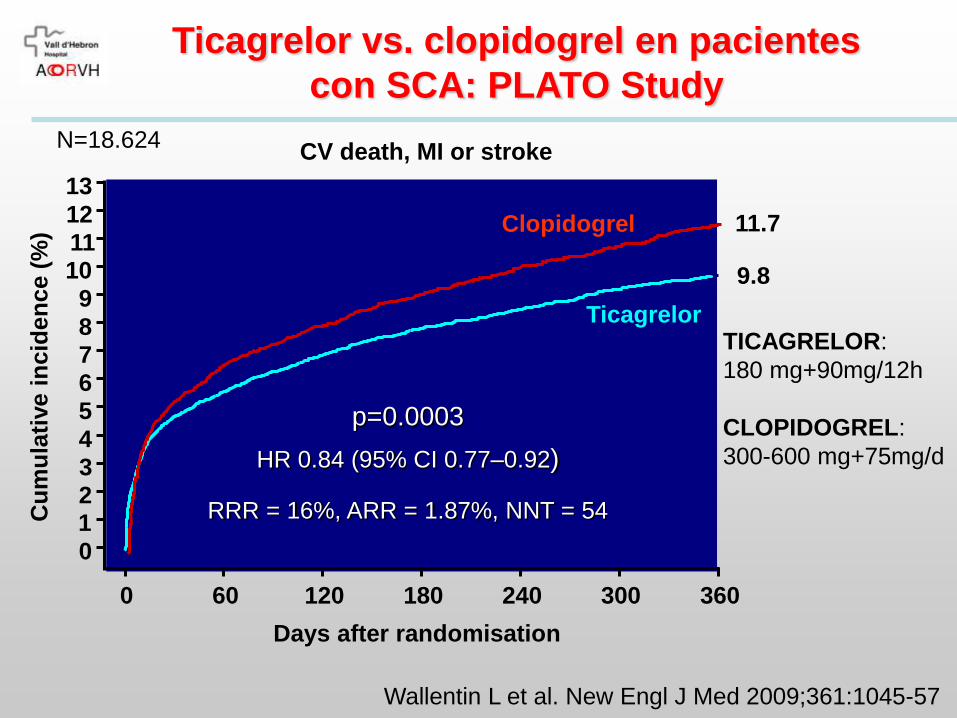
Ticagrelor vs. clopidogrel en pacientes
con SCA: PLATO Study
Wallentin L et al. New Engl J Med 2009;361:1045-57
Days after randomisation
0 60 120 180 240 300 360
12
11 10
9
8 7
6
5
4
3
2 1
0
13
Cu
mu
lati
ve i
ncid
en
ce (
%)
9.8
11.7 Clopidogrel
Ticagrelor
p=0.0003
HR 0.84 (95% CI 0.77–0.92)
RRR = 16%, ARR = 1.87%, NNT = 54
N=18.624
TICAGRELOR:
180 mg+90mg/12h
CLOPIDOGREL:
300-600 mg+75mg/d
CV death, MI or stroke

PLATO Study: Efficacy end points
Wallentin L et al. New Engl J Med 2009;361:1045-57
0
2
4
6
8
10
12
14
CVD
/MI/C
VA
CV d
eath M
I
CVA
Dea
th
Sev
ere
rec.
Isch
.
Ste
nt thr
ombo
sis
Clopidogrel Ticagrelor
%
P<0.001
P=0.005
P=NS
P=0.009
P<0.001
P=NS
P<0.001

PLATO Study: Bleeding end points
Wallentin L et al. New Engl J Med 2009;361:1045-57
11,2
3,8
2,2
7,9
5,8 5,8
0,2
11,6
4,5
2,8
7,4
5,35,8
0,3
0
2
4
6
8
10
12
14
PLA
TO m
ajor
Non
-CABG
PLA
TO m
ajor
NON-C
ABG T
IMI m
ajor
CABG P
LATO
maj
or
CABG T
IMI m
ajor
Life- t
hreat
enin
gIC
H
Clopidogrel Ticagrelor
%
P=NS
P=0.03
P=NS
P=0.03
P=NS
P=NS
P=NS

Ticagrelor vs. Prasugrel: timing of benefit

PLATO Study: Subgroup analysis
Wallentin L et al. New Engl J Med 2009;361:1045-57

PLATO Study: Patients with prior stroke
James S et al. Circulation 2012;125:2914-21
Primary
endpoint
Major
bleeding

PLATO Study: Invasive vs noninvasive strategy
James S et al. BMJ 2011;342:d3527
3.9%
5.0%
6.1%
8.2%

PLATO Study: Diabetic subgroup
James S et al. Eur Heart J 2010;31:3006-16

PLATO Study: Diabetic subgroup

TRITON vs PLATO: Diferencias metodológicas
TRITON PLATO
POBLACIÓN SCA que se trata con ICP SCA (manejo invasivo o no)
TTO PREVIO No Permitido
Dosis
clopidogrel
300 mg 300-600 mg
CABG 2.7% 10.2%
Manejo médico 0% 16.9%
Duración estudio
(mediana)
14.5 meses 9 meses
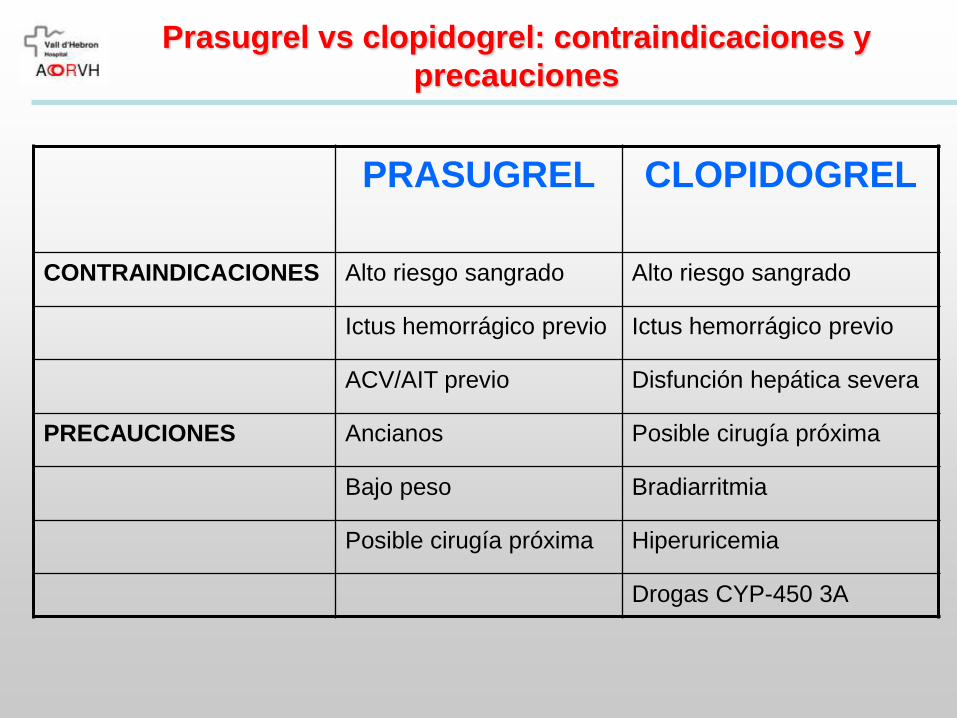
Prasugrel vs clopidogrel: contraindicaciones y
precauciones
PRASUGREL CLOPIDOGREL
CONTRAINDICACIONES Alto riesgo sangrado Alto riesgo sangrado
Ictus hemorrágico previo Ictus hemorrágico previo
ACV/AIT previo Disfunción hepática severa
PRECAUCIONES Ancianos Posible cirugía próxima
Bajo peso Bradiarritmia
Posible cirugía próxima Hiperuricemia
Drogas CYP-450 3A
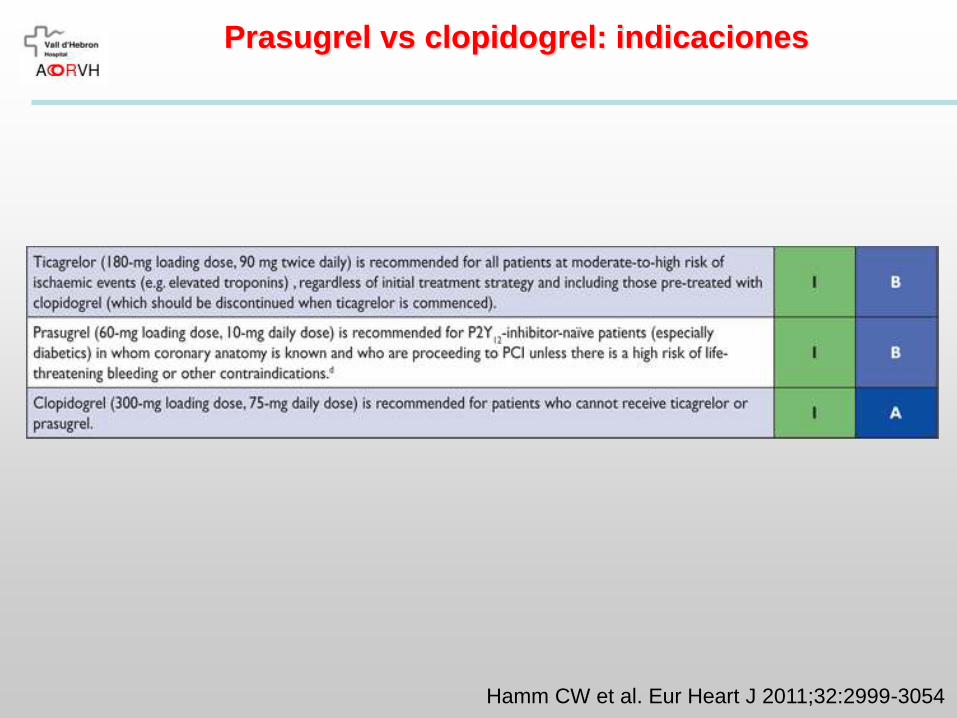
Prasugrel vs clopidogrel: indicaciones
Hamm CW et al. Eur Heart J 2011;32:2999-3054

Prasugrel vs clopidogrel: sólo en SCA!!
Trenk D et al. J Am Coll Cardiol 2012;59:2159-64
TRIGGER PCI Study
423 pts tras SFA por CI estable y con reactividad plaquetaria elevada con clopidogrel

Muchas gracias