Taquicardias ventriculares no estructurales
33
ARRITMIAS VENTRICULARES Ana Isabel Nieva Silva R1 Medicina Interna
-
Upload
ana-isabel-nieva-silva -
Category
Health & Medicine
-
view
133 -
download
0
Transcript of Taquicardias ventriculares no estructurales

ARRITMIAS VENTRICULARE
S
Ana Isabel Nieva SilvaR1 Medicina Interna

Clasificación de las arritmias
ventricularesHemodinámicamen
te estable
Asintomática
Síntomas mínimos
Ej. palpitaciones
Hemodinámicamente inestable
Presíncope
Síncope
Presentación clínica
– Mareo– Aturdimiento– Debilidad– «Vista nublada»

AsV Hemodinámicamente inestables
Muerte por parada circulatoria inesperada, normalmente por arritmia cardiaca, que tiene lugar en la primera hora desde el inicio de los síntomas
MCSMCS o parada cardiaca, en la que la intervención médica (p. ej., desfibrilación) revierte el cuadro
Paro cardiac
o súbito

Clasificación
• 3 o más latidos de duración, que termina espontáneamente en menos de 30 s.
• La TV es una arritmia cardiaca de 3 o más complejos consecutivos de duración que proceden del ventrículo a una velocidad > 100 lat/min (duración del ciclo < 600 ms)
TVNS
• TV de más de 30 s de duración y/o que requiere terminación, debido a deterioro hemodinámico, en menos de 30 s
TV sostenid
a
Electrofisiología

TVNS
Monomórfica
TVNS con morfología de un
único QRS
Polimórfica
TVNS con morfología QRS
cambiante con una duración del ciclo
entre 600 y 180 ms

TV sostenidaMonomórfi
ca
TV sostenida con una morfología única estable de
QRS
Polimórfica
TV sostenida con morfología
cambiante o QRS multiformes con una
duración del ciclo entre 600 y 180 ms


Zipes DP, et al. Guía de la Sociedad Europea de Cardiología: manejo de pacientes con arritmias ventriculares y la prevención en la muerte cardiaca súbita. Rev Esp Cardiol. 2006;59(12):1328.e1-51

ARRITMIAS VENTRICULARES
SIN CARDIOPATÍA ESTRUCTURAL
Monomorfas Polimorfas 'benignas'
(canalopatías)
'letales'
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

ARRITMIAS VENTRICULARES MONOMORFAS
• Suelen tener un buen pronóstico
• Están descritos casos de muerte súbita
• Participan en el desarrollo de taquicarmiodiopatías
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

TAQUICARMIODIOPATÍAS
• Cardiopatía inducida por latidos ectópicos aislados, sin taquicardia ventricular (TV) sostenida acompañante.
• Su aparición es más probable en aquellos casos en los que se objetive al menos >10 000 latidos ectópicos ventriculares al día.
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

TV monomorfas
TV de tracto de salida
TSVD la más frecuente
Postpotenciales tardíos
TV idiopáticas fasciculares
Mecanismo de reentrada
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

ARRITMIAS POLIMORFAS O CANALOPATÍAS
1. Son menos frecuentes.
2. Se asocian generalmente a trastornos genéticos con alteraciones a nivel molecular.
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

ARRITMIAS POLIMORFAS O CANALOPATÍAS
Síndrome QT largo
Síndrome de
Brugada
FV idiopátic
a
TV polimorfa catecolaminérgic
a
Síndrome QT corto
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

Síndrome QT largo
QTc >440 ms
varones QTc >460 ms mujeres
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

Síndrome QT largo
Tamariz Amalia et al. Canalopatías. Cardiol Clin 2012; 26: 335-53.

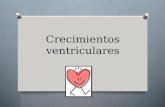
Síndrome QT largo• Subtipos: LQT1, LQT2, LQT3
ECG de sindrome de QT largo (QTc 480 ms. Ondas T amplias y picudas).
Tamariz Amalia et al. Canalopatías. Cardiol Clin 2012; 26: 335-53.

Tamariz Amalia et al. Canalopatías. Cardiol Clin 2012; 26: 335-53.

Síndrome QT largo• Tratamiento
Con o sin clínica
Evitar actividad física extenuante
BB Pacientes con riesgo elevado
de muerte súbita
SQTL tipo 3Puntas torcidasResucitados MSC
DAI
Tamariz Amalia et al. Canalopatías. Cardiol Clin 2012; 26: 335-53.

Síndrome de Brugada
Tamariz Amalia et al. Canalopatías. Cardiol Clin 2012; 26: 335-53.

Síndrome de Brugada

Síndrome de BrugadaManejo terapéutico actual recomendado:
La quinidina y el isoproterenol pueden ser útiles en pacientes con tormentas eléctricas, incluso en presencia de un DCI.
Tamariz Amalia et al. Canalopatías. Cardiol Clin 2012; 26: 335-53.

TV polimorfa catecolaminérgica
• Producida por un alteración en la homeostasis del calcio intracelular.
• Su forma de presentación clínica es síncope o muerte súbita inducida por el ejercicio físico.
• ECG basal suele ser normal.
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

Síndrome QT corto• Es muy poco frecuente.
• Se define por un intervalo QT <300-320 ms.
• La indicación de DAI es exclusivamente como prevención secundaria.
EN Prystowsky ,et al.J Am Coll Cardiol 2012; 59:1733-1744.

TV y cardiopatía estructural
• El desfibrilador implantable (DAI) proporciona una protección significativa contra el riesgo de muerte súbita.
• La ablación de TVs con cartografía electro-anatómica, y, en casos seleccionados, el abordaje percutáneo del espacio pericárdico.
Paolo Della Bella, et al. Management of Ventricular Tachycardia in the Setting of a Dedicated Unit for the Treatment of Complex Ventricular Arrhythmias: Long-Term Outcome After Ablation.. Circulation. 2013;127:1359-
1368.

Management of PVCs. aSee table for definitions of structural heart disease; bMedical therapy ± ICD; aAbsence of high scar burden suggests reversibility.
Christian Torp Pedersen et al. Europace 2014;16:1257-1283
The article has been co-published with permission in EP-Europace, Journal of Arrhythmia and Heart Rhythm. All rights reserved in respect of Journal of Arrhythmia and Heart Rhythm. ©The Author 2014. For EP-Europace, ©The Author 2014

Evaluation for the presence or absence of structural heart disease.
Christian Torp Pedersen et al. Europace 2014;16:1257-1283
The article has been co-published with permission in EP-Europace, Journal of Arrhythmia and Heart Rhythm. All rights reserved in respect of Journal of Arrhythmia and Heart Rhythm. ©The Author 2014. For EP-Europace, ©The Author 2014

(A) Right ventricular (RV) outflow tract VT. (B) Left coronary cusp VT.
Christian Torp Pedersen et al. Europace 2014;16:1257-1283
The article has been co-published with permission in EP-Europace, Journal of Arrhythmia and Heart Rhythm. All rights reserved in respect of Journal of Arrhythmia and Heart Rhythm. ©The Author 2014. For EP-Europace, ©The Author 2014

Electrocardiograms (ECGs) in long OT syndrome, short OT syndrome, Brugada syndrome, arrhythmogenic right ventricular cardiomyopathy, hypertrophic cardiomyopathy, WPW
syndrome.
Christian Torp Pedersen et al. Europace 2014;16:1257-1283
The article has been co-published with permission in EP-Europace, Journal of Arrhythmia and Heart Rhythm. All rights reserved in respect of Journal of Arrhythmia and Heart Rhythm. ©The Author 2014. For EP-Europace, ©The Author 2014

Sustained monomorphic ventricular tachycardia evaluation and management.
Christian Torp Pedersen et al. Europace 2014;16:1257-1283
The article has been co-published with permission in EP-Europace, Journal of Arrhythmia and Heart Rhythm. All rights reserved in respect of Journal of Arrhythmia and Heart Rhythm. ©The Author 2014. For EP-Europace, ©The Author 2014

Sustained polymorphic ventricular tachycardia/ventricular fibrillation. aLV function should be reassessed at 40 days after MI or 90 days after revascularization.
Christian Torp Pedersen et al. Europace 2014;16:1257-1283
The article has been co-published with permission in EP-Europace, Journal of Arrhythmia and Heart Rhythm. All rights reserved in respect of Journal of Arrhythmia and Heart Rhythm. ©The Author 2014. For EP-Europace, ©The Author 2014

Management of VAs in CHD. ATP, antitachycardia pacing; CHD, congenital heart disease; d-TGA, transposition of the great vessels; ICD, implantable cardioverter-defibrillator; LVOTO, LV outflow tract obstruction; PMVT, polymorphic ventricular tachycardia; SMVT, sustained
monomorphic ventricular tachycardia.
Christian Torp Pedersen et al. Europace 2014;16:1257-1283
The article has been co-published with permission in EP-Europace, Journal of Arrhythmia and Heart Rhythm. All rights reserved in respect of Journal of Arrhythmia and Heart Rhythm. ©The Author 2014. For EP-Europace, ©The Author 2014

Gracias