






Idiomas
Páginas
Jurídico

Nuevas estrategias de tratamiento en tumores con mutaciones de BRCA
Emilio Alba UGCI Oncología
Hospital Universitario Regional y Virgen de la Victoria
Facultad de Medicina. Málaga
IBIMA

ÍNDICE DE LA PRESENTACIÓN
Mecanismo de acción
Magnitud del problema: frecuencia y penetrancia de BRCA
Cáncer de mama
Cáncer de ovario
Otros tumores
Conclusiones y perspectivas
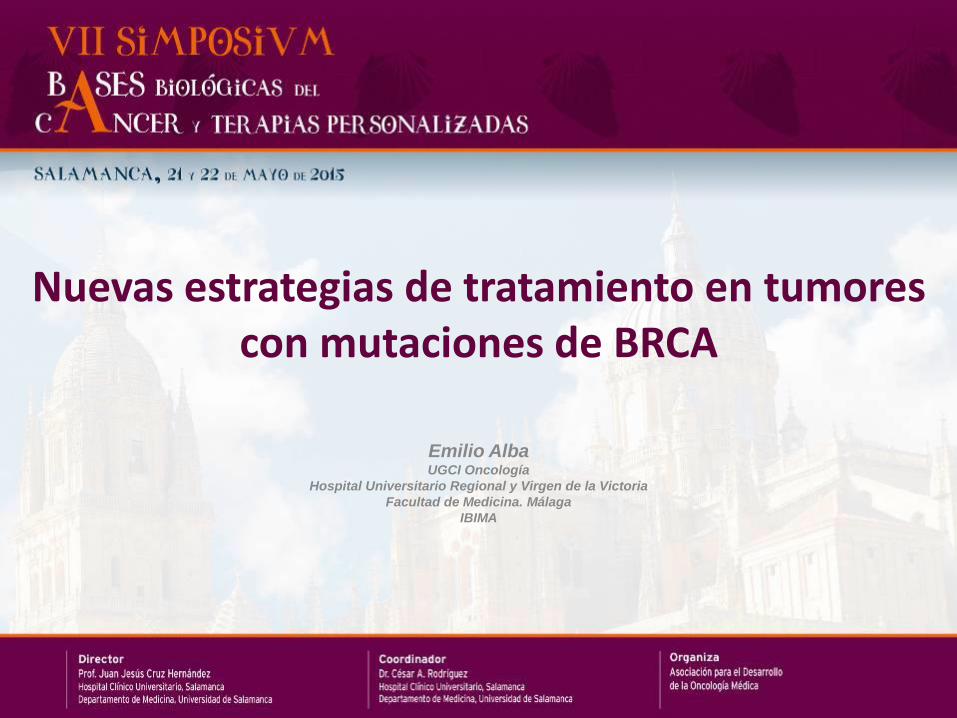
Mechanisms of Action of Olaparib
Survival
Normal cell
Repair by Homologous Recombination
No effective repair
(No HR pathway)
Cell death
Cancer cell with HRD
SSBs increased by dacarbazine, temozolomide and topotecan
DSBs increased by platinums
Mechanism 1:
Tumor specific killing
by olaparib
PARP
Replicating cells
olaparib
Mechanism 2: Potentiation
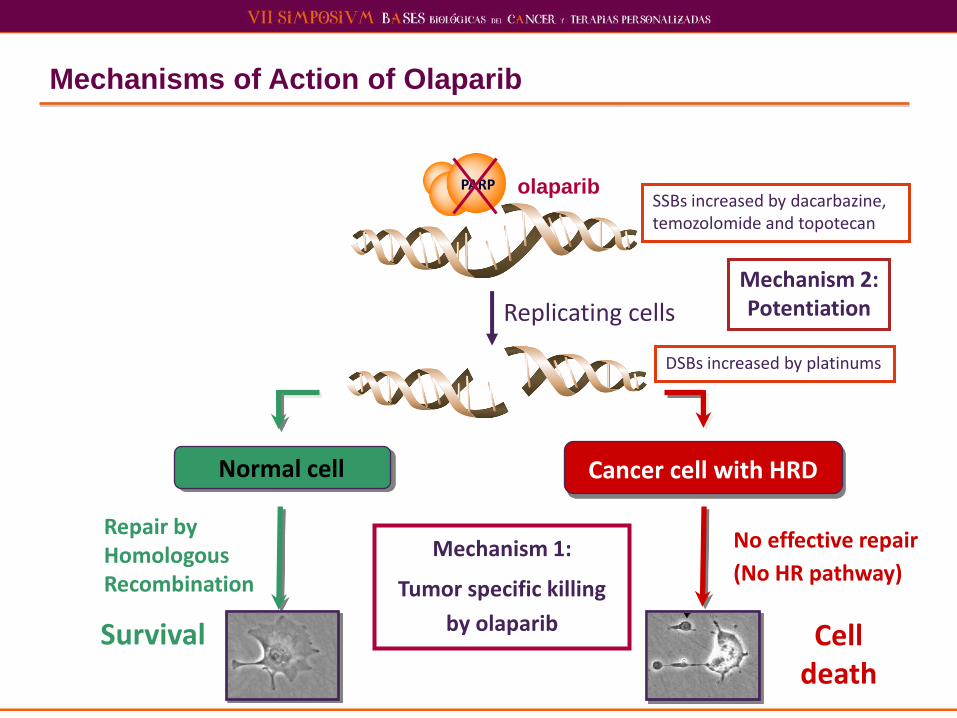
The Concept of Synthetic Lethality
(PARP) (BRCA)
Ashworth, A. J Clin Oncol; 26:3785-3790 2008

Riesgo de cáncer en personas con mutaciones de los genes BRCA 1/2
BRCA 1 BRCA 2
Mama 65-71% 45-84%
Ovario 12-63% 7-27%
Mama-varón 3-10% 7%
Próstata ? 5.2-7.5%
Páncreas 1.2% 1.5-4%
Levy-Lahad E. BJC 2007
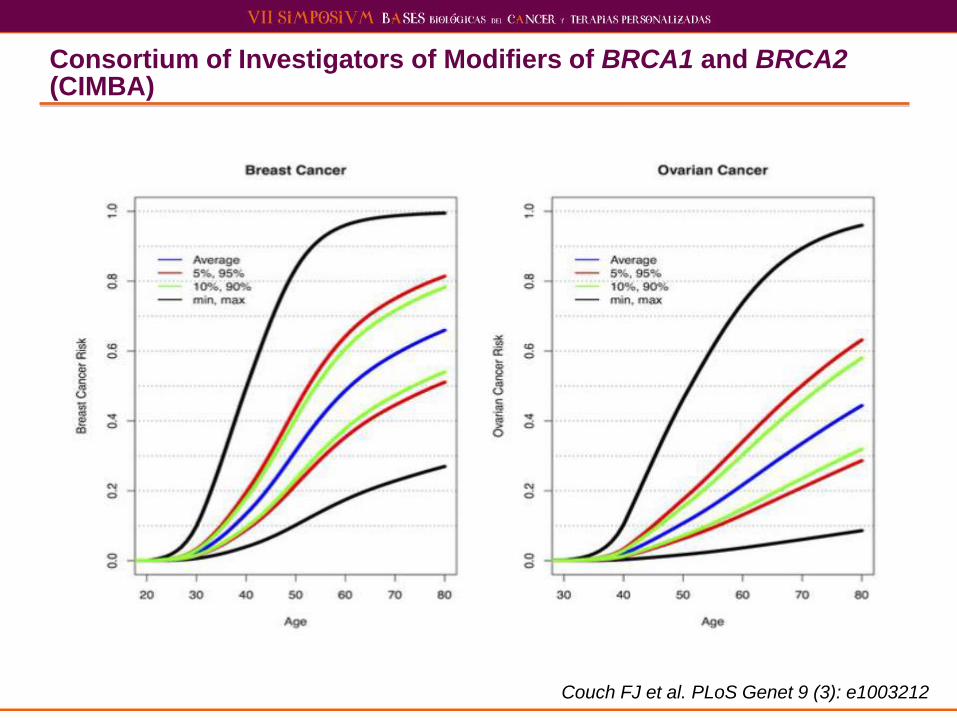
Consortium of Investigators of Modifiers of BRCA1 and BRCA2 (CIMBA)
Couch FJ et al. PLoS Genet 9 (3): e1003212

Chemotherapeutic Agents: Double Strand DNA Breaks
Kennedy R et al. JNCI 2004; 96:1659-1668
Alkylators DNA interstrand cross-links double strand (DS) DNA breaks
Cyclophosphamide
Platinums Forms adducts with DNA Cisplatin Carboplatin Oxaliplatin
Topoisomerase I poisons
Arrest of DNA replication forks
Etoposide Irinotecan Topotecan Mitoxantrone
Topoisomerase II poisons
DNA interstrand cross-linking, generation of O2 free radicals
Doxorubicin Epirubicin
Bleomycin Directly damages DNA DS DNA breaks
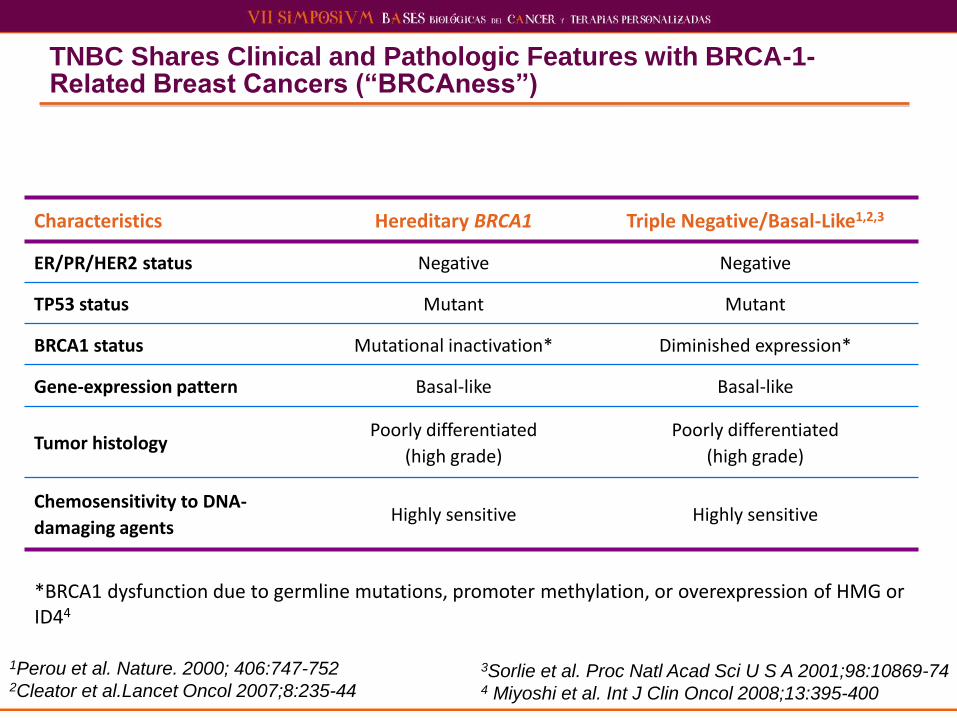
TNBC Shares Clinical and Pathologic Features with BRCA-1-Related Breast Cancers (“BRCAness”)
3Sorlie et al. Proc Natl Acad Sci U S A 2001;98:10869-74 4 Miyoshi et al. Int J Clin Oncol 2008;13:395-400
1Perou et al. Nature. 2000; 406:747-752 2Cleator et al.Lancet Oncol 2007;8:235-44
Characteristics Hereditary BRCA1 Triple Negative/Basal-Like1,2,3
ER/PR/HER2 status Negative Negative
TP53 status Mutant Mutant
BRCA1 status Mutational inactivation* Diminished expression*
Gene-expression pattern Basal-like Basal-like
Tumor histology Poorly differentiated
(high grade)
Poorly differentiated
(high grade)
Chemosensitivity to DNA-
damaging agents Highly sensitive Highly sensitive
*BRCA1 dysfunction due to germline mutations, promoter methylation, or overexpression of HMG or ID44
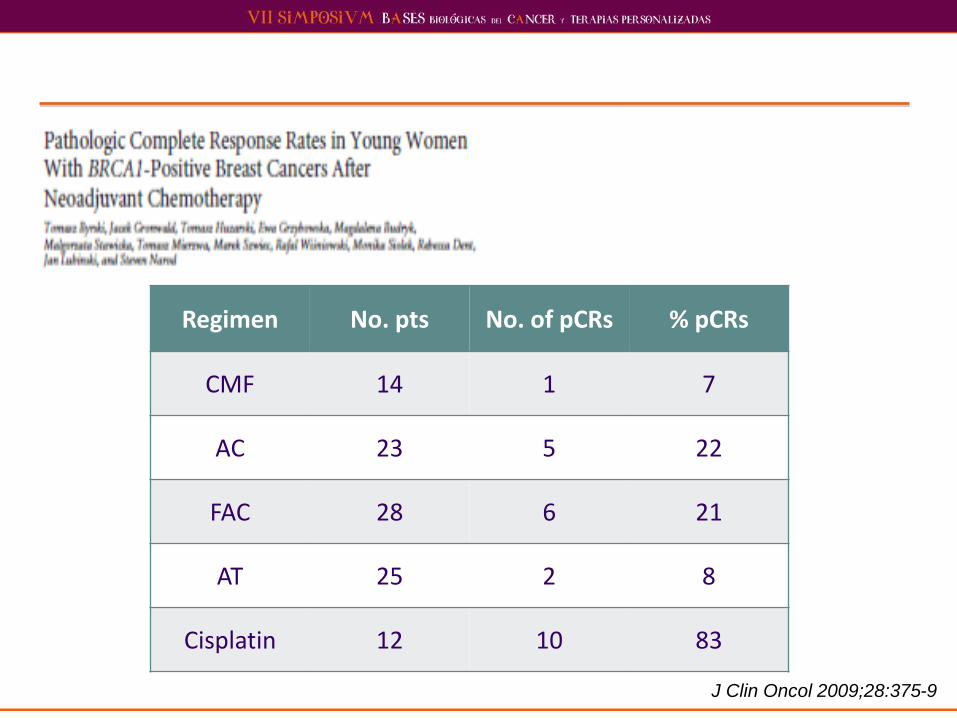
Regimen No. pts No. of pCRs % pCRs
CMF 14 1 7
AC 23 5 22
FAC 28 6 21
AT 25 2 8
Cisplatin 12 10 83
J Clin Oncol 2009;28:375-9
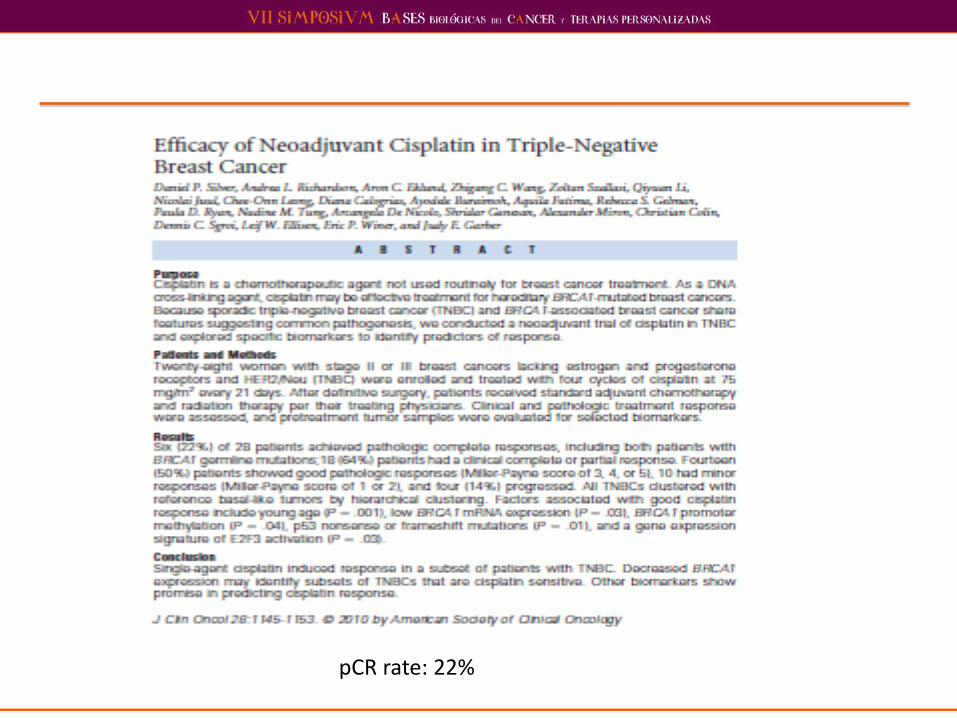
pCR rate: 22%
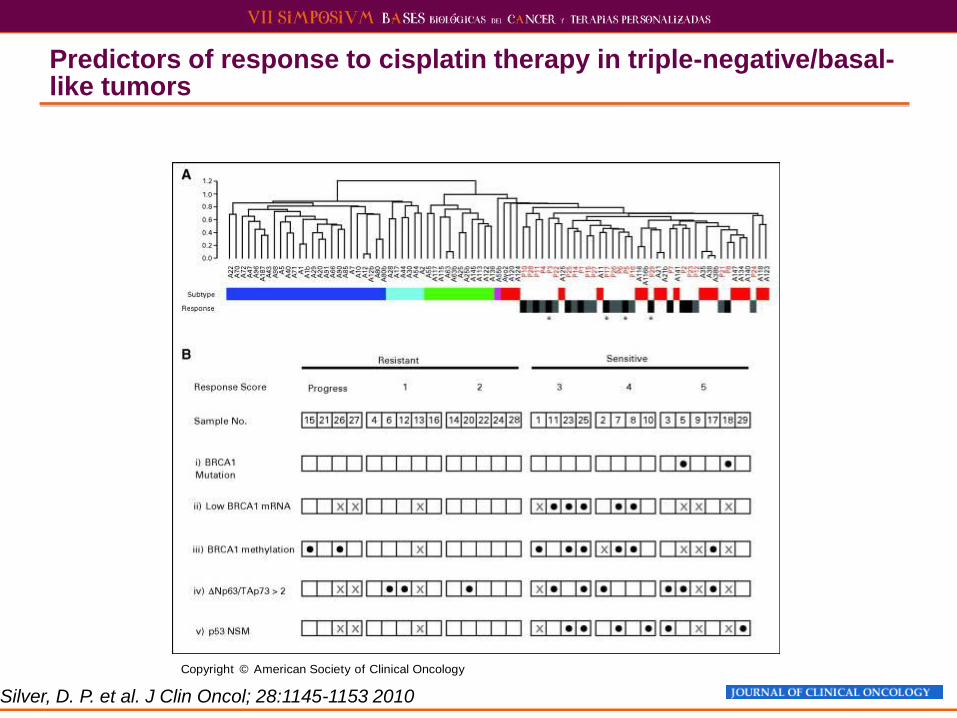
Predictors of response to cisplatin therapy in triple-negative/basal-like tumors
Copyright © American Society of Clinical Oncology
Silver, D. P. et al. J Clin Oncol; 28:1145-1153 2010
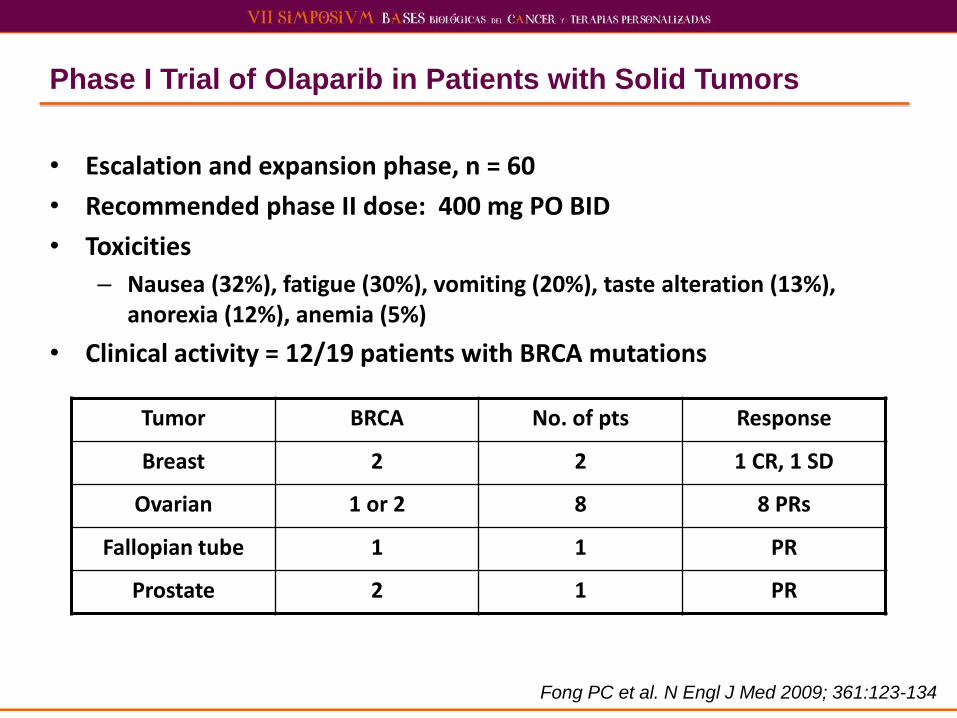
Phase I Trial of Olaparib in Patients with Solid Tumors
• Escalation and expansion phase, n = 60
• Recommended phase II dose: 400 mg PO BID
• Toxicities
– Nausea (32%), fatigue (30%), vomiting (20%), taste alteration (13%), anorexia (12%), anemia (5%)
• Clinical activity = 12/19 patients with BRCA mutations
Tumor BRCA No. of pts Response
Breast 2 2 1 CR, 1 SD
Ovarian 1 or 2 8 8 PRs
Fallopian tube 1 1 PR
Prostate 2 1 PR
Fong PC et al. N Engl J Med 2009; 361:123-134
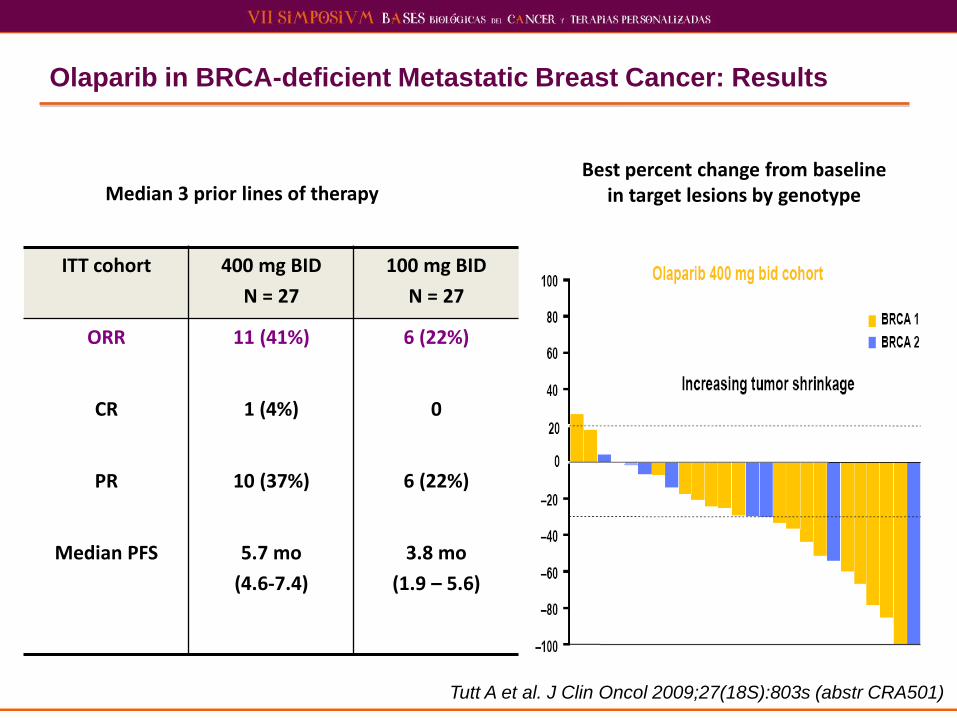
Olaparib in BRCA-deficient Metastatic Breast Cancer: Results
ITT cohort 400 mg BID
N = 27
100 mg BID
N = 27
ORR 11 (41%) 6 (22%)
CR 1 (4%) 0
PR 10 (37%) 6 (22%)
Median PFS 5.7 mo
(4.6-7.4)
3.8 mo
(1.9 – 5.6)
Tutt A et al. J Clin Oncol 2009;27(18S):803s (abstr CRA501)
Best percent change from baseline in target lesions by genotype Median 3 prior lines of therapy

Objective Response Rate (by RECIST)
Gelmon KA et al. Proc ASCO 2010;Abstract 3002.
BRCA Mutation-Positive BRCA Mutation-Negative
Ovarian 7/17 (41.2%) 11/46 (23.9%)
Breast 0/8 (0) 0/15 (0)
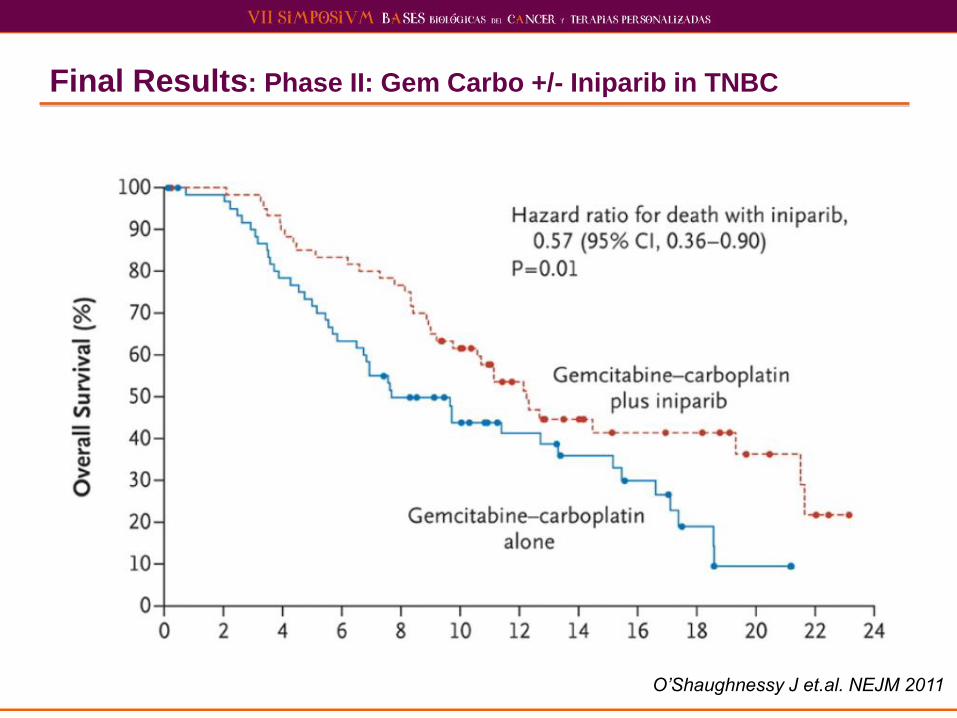
Final Results: Phase II: Gem Carbo +/- Iniparib in TNBC
O’Shaughnessy J et.al. NEJM 2011
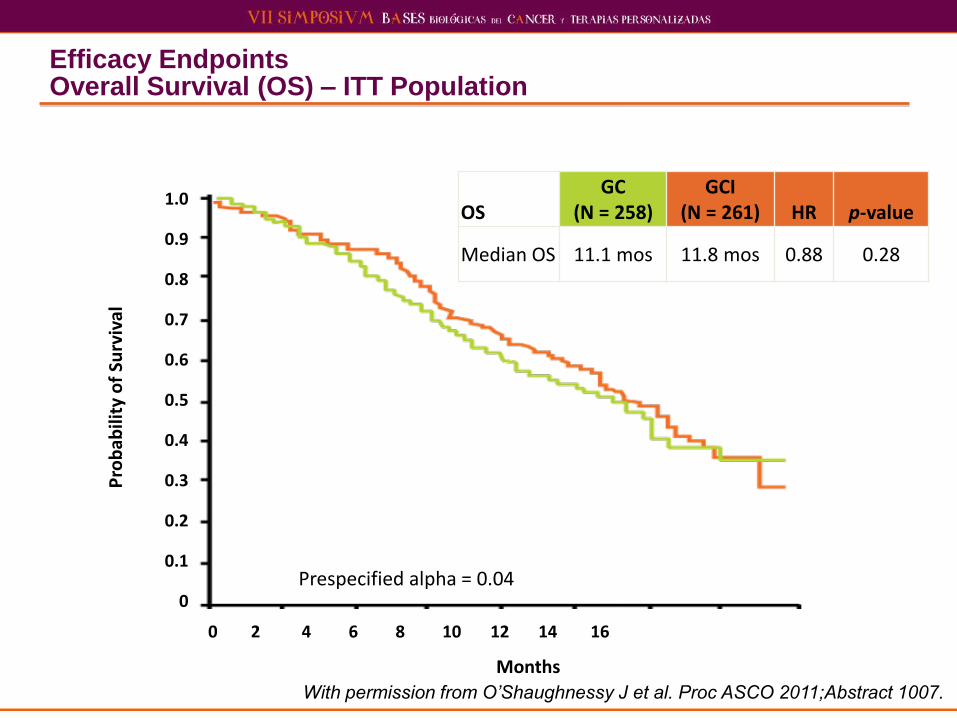
Efficacy Endpoints Overall Survival (OS) – ITT Population
With permission from O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.
Pro
bab
ility
of
Surv
ival
Prespecified alpha = 0.04
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0 2 4 6 8 10 12 14 16
OS GC
(N = 258) GCI
(N = 261) HR p-value
Median OS 11.1 mos 11.8 mos 0.88 0.28
Months

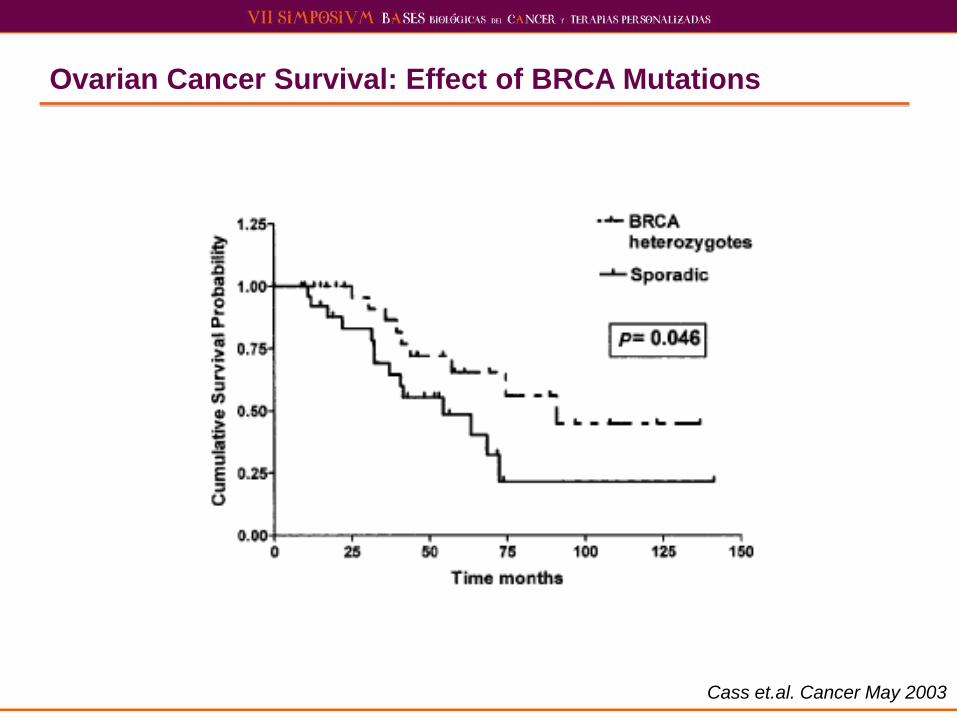
Ovarian Cancer Survival: Effect of BRCA Mutations
Cass et.al. Cancer May 2003
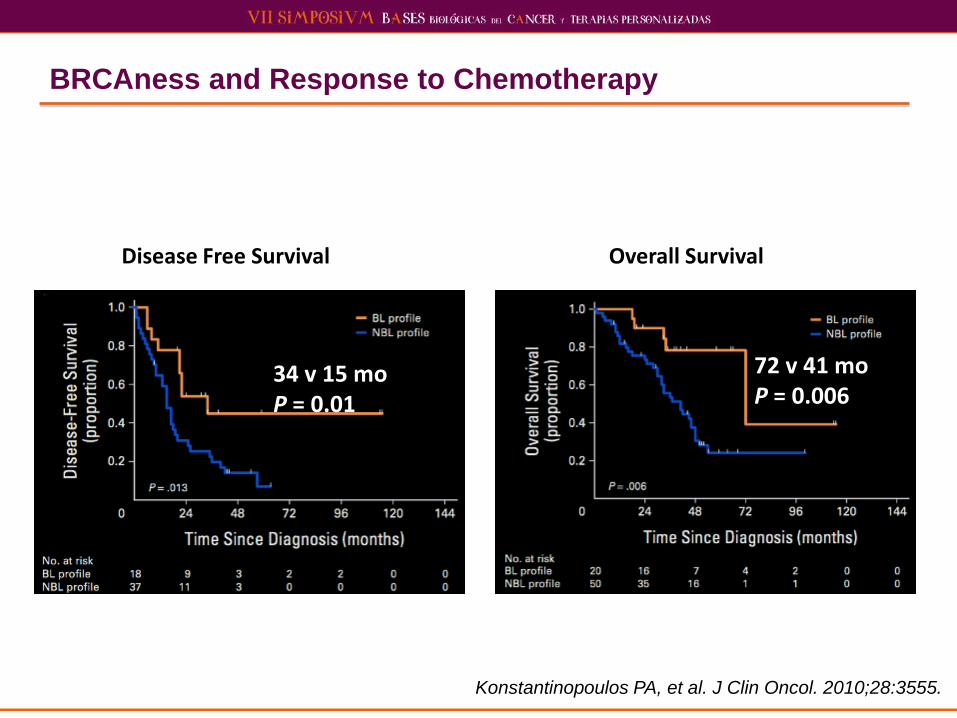
BRCAness and Response to Chemotherapy
Konstantinopoulos PA, et al. J Clin Oncol. 2010;28:3555.
Disease Free Survival Overall Survival
34 v 15 mo P = 0.01
72 v 41 mo P = 0.006
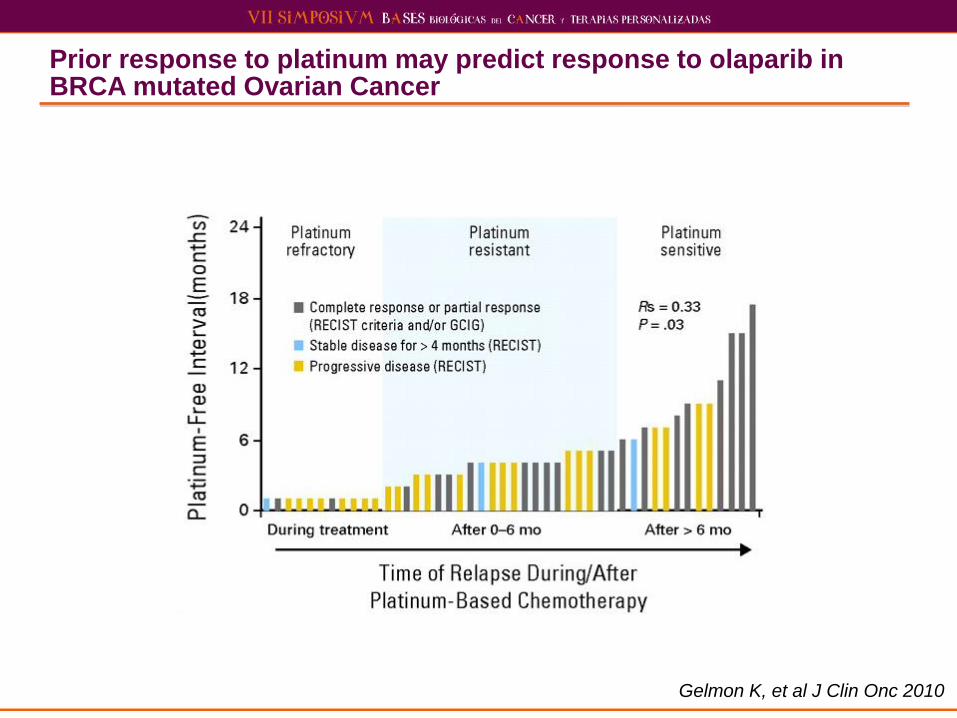
Prior response to platinum may predict response to olaparib in BRCA mutated Ovarian Cancer
Gelmon K, et al J Clin Onc 2010
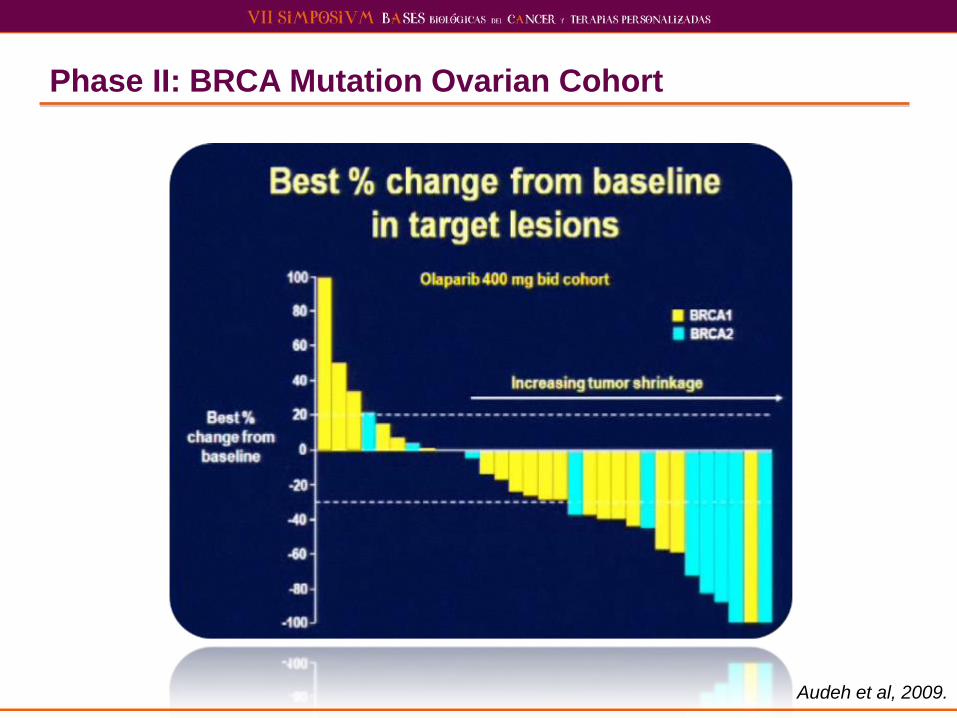
Phase II: BRCA Mutation Ovarian Cohort
Audeh et al, 2009.
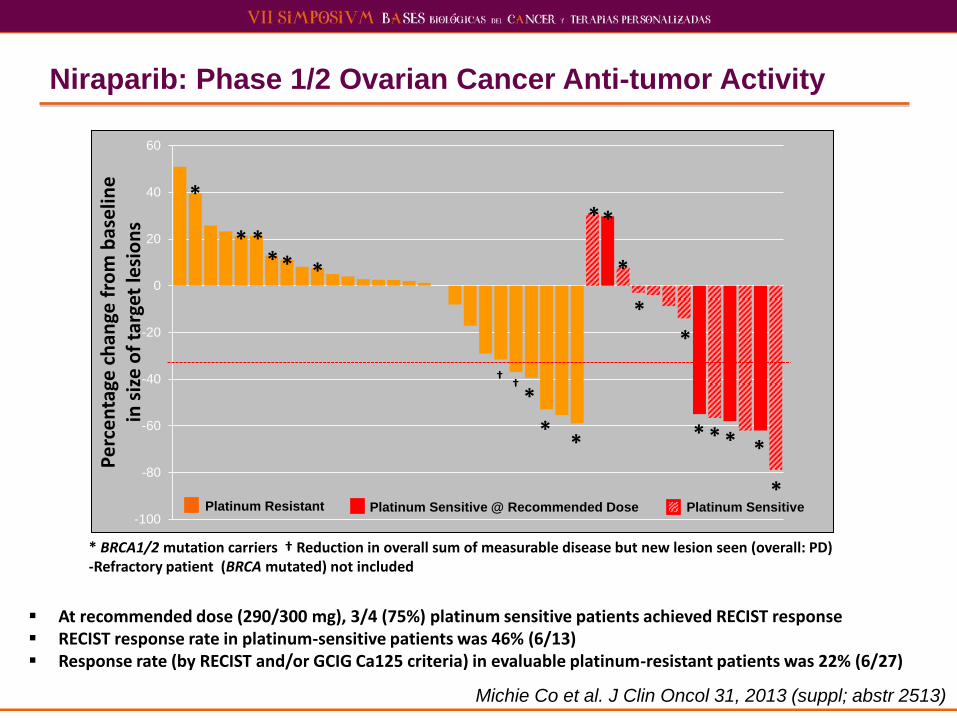
Niraparib: Phase 1/2 Ovarian Cancer Anti-tumor Activity
Michie Co et al. J Clin Oncol 31, 2013 (suppl; abstr 2513)
At recommended dose (290/300 mg), 3/4 (75%) platinum sensitive patients achieved RECIST response RECIST response rate in platinum-sensitive patients was 46% (6/13) Response rate (by RECIST and/or GCIG Ca125 criteria) in evaluable platinum-resistant patients was 22% (6/27)
* BRCA1/2 mutation carriers † Reduction in overall sum of measurable disease but new lesion seen (overall: PD) -Refractory patient (BRCA mutated) not included
-100
-80
-60
-40
-20
0
20
40
60
Pe
rce
nta
ge c
han
ge f
rom
bas
elin
e
in s
ize
of
targ
et le
sio
ns
Platinum Resistant Platinum Sensitive Platinum Sensitive @ Recommended Dose
*
*
* * * *
*
* *
*
*
* *
* * * *
*
*
† †
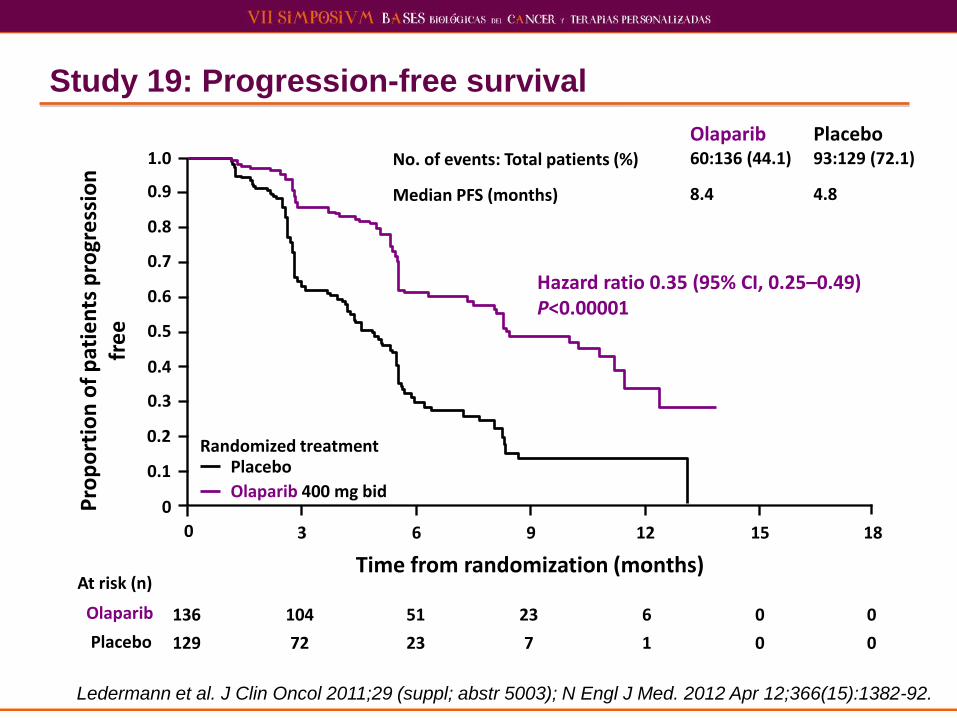
Study 19: Progression-free survival
Ledermann et al. J Clin Oncol 2011;29 (suppl; abstr 5003); N Engl J Med. 2012 Apr 12;366(15):1382-92.
0
Time from randomization (months)
136 104 51 23 6 0 0
129 72 23 7 1 0 0
At risk (n)
Olaparib
Placebo
0.6
0.8
0.9
0
0.1
0.2
0.3
0.4
0.5
0.7
1.0
3 6 9 12 15 18
No. of events: Total patients (%) Median PFS (months)
Olaparib 60:136 (44.1) 8.4
Placebo 93:129 (72.1) 4.8
Hazard ratio 0.35 (95% CI, 0.25–0.49) P<0.00001
Olaparib 400 mg bid
Placebo Randomized treatment
Pro
po
rtio
n o
f p
atie
nts
pro
gre
ssio
n
fre
e
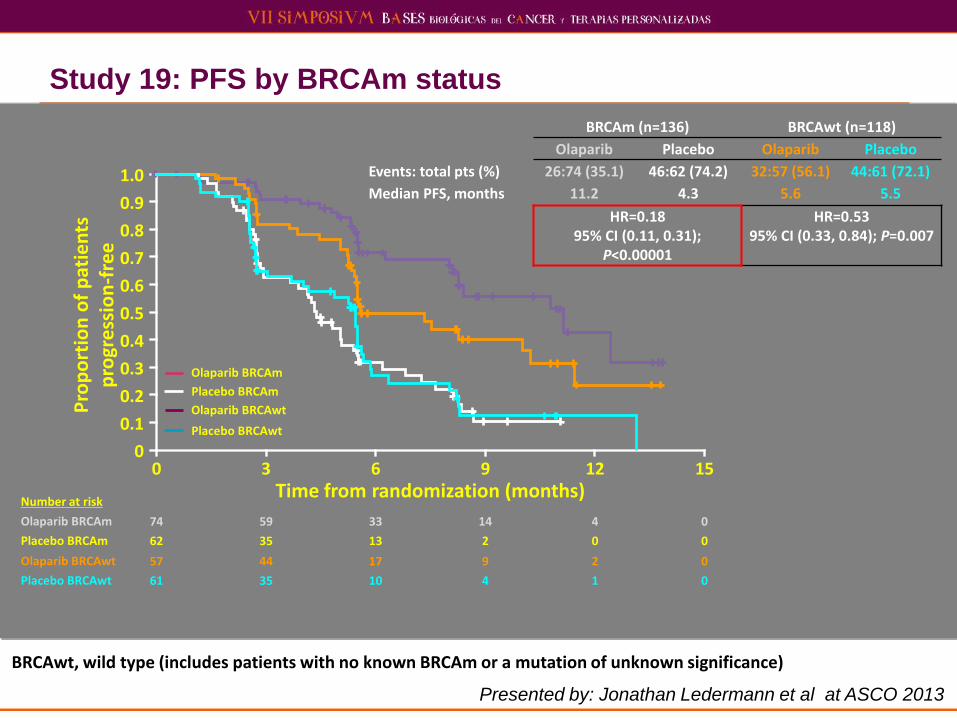
Study 19: PFS by BRCAm status
Presented by: Jonathan Ledermann et al at ASCO 2013
0 Time from randomization (months)
0
1.0
Pro
po
rtio
n o
f p
atie
nts
p
rogr
ess
ion
-fre
e
3 6 9 12 15
Olaparib BRCAm
Olaparib BRCAwt
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
BRCAm (n=136) BRCAwt (n=118)
Olaparib Placebo Olaparib Placebo
Events: total pts (%) 26:74 (35.1) 46:62 (74.2) 32:57 (56.1) 44:61 (72.1)
Median PFS, months 11.2 4.3 5.6 5.5
HR=0.18 95% CI (0.11, 0.31);
P<0.00001
HR=0.53 95% CI (0.33, 0.84); P=0.007
Placebo BRCAm
Placebo BRCAwt
Number at risk
Olaparib BRCAm
Olaparib BRCAwt
Placebo BRCAm
Placebo BRCAwt
74 59 33 14 4 0
57 44 17 9 2 0
62 35 13 2 0 0
61 35 10 4 1 0
BRCAwt, wild type (includes patients with no known BRCAm or a mutation of unknown significance)
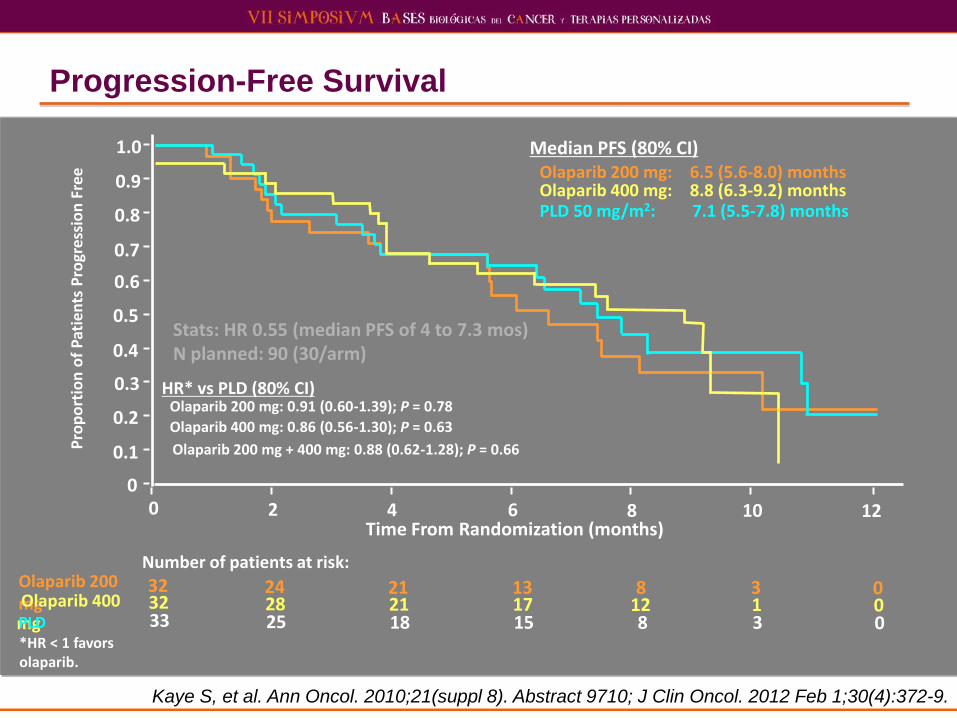
Progression-Free Survival
Olaparib 200 mg: 6.5 (5.6-8.0) months
Median PFS (80% CI)
Olaparib 400 mg: 8.8 (6.3-9.2) months PLD 50 mg/m2: 7.1 (5.5-7.8) months
HR* vs PLD (80% CI) Olaparib 200 mg: 0.91 (0.60-1.39); P = 0.78
Olaparib 400 mg: 0.86 (0.56-1.30); P = 0.63
Olaparib 200 mg + 400 mg: 0.88 (0.62-1.28); P = 0.66
Time From Randomization (months)
Pro
po
rtio
n o
f P
atie
nts
Pro
gre
ssio
n F
ree
0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0 12 10 8 6 4 2
*HR < 1 favors olaparib.
32 0 3 8 13 21 24 32 0 1 12 17 21 28 33 0 3 8 15 18 25
Number of patients at risk: Olaparib 200 mg Olaparib 400 mg PLD
Stats: HR 0.55 (median PFS of 4 to 7.3 mos) N planned: 90 (30/arm)
Kaye S, et al. Ann Oncol. 2010;21(suppl 8). Abstract 9710; J Clin Oncol. 2012 Feb 1;30(4):372-9.
Summary: PARPi in Phase III Development as Maintenance Therapy in Ovarian Cancer
1. AZD 2281 (KU-0059436) = Olaparib – SOLO-1 = Front-line HGS maintenance in BRCAmut
– SOLO-2 = Platinum sensitive HGS maintenance in BRCAmut
2. MK-4827 = Niraparib – NOVA = Platinum sensitive HGS maintenance in BRCAmut and
BRCAwt
3. CO-338 (AG014699, PF-01367338) = Rucaparib – ARIEL-3 = Platinum sensitive HGS and endometrioid maintenance
in BRCAmut and BRCAwt
PARPi in Phase III Development in Ovarian Cancer
1. AZD 2281 (KU-0059436) = Olaparib
2. MK-4827 = Niraparib
3. CO-338 (AG014699, PF-01367338) = Rucaparib
Others with randomized trials in devleopment ABT-888 = Veliparib
BMN 673
No direct clinical comparisons!
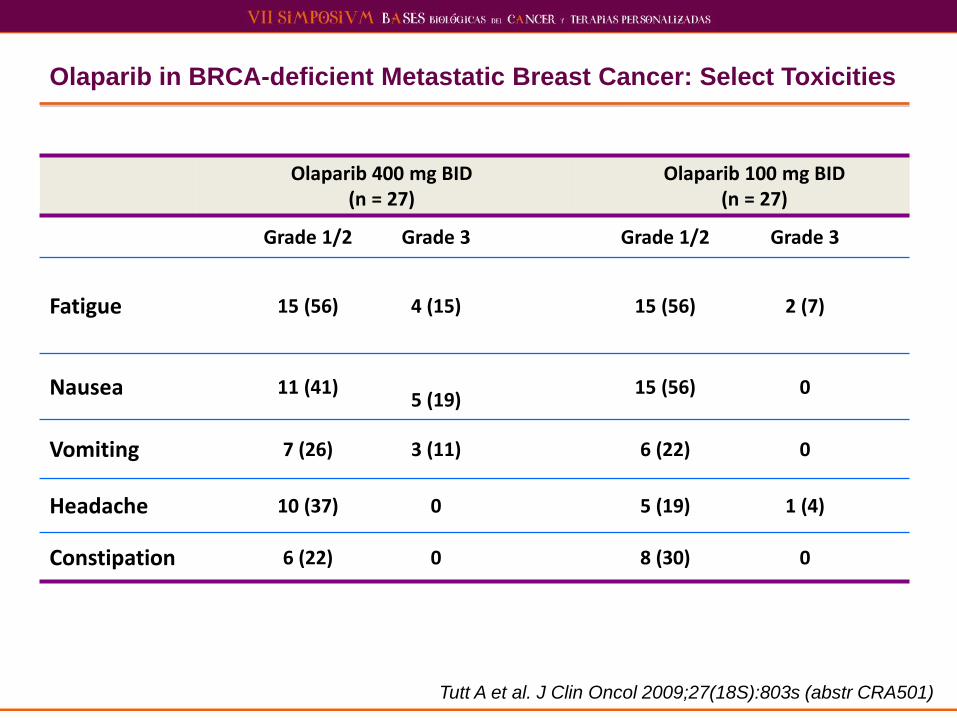
Olaparib in BRCA-deficient Metastatic Breast Cancer: Select Toxicities
Tutt A et al. J Clin Oncol 2009;27(18S):803s (abstr CRA501)
Olaparib 400 mg BID (n = 27)
Olaparib 100 mg BID (n = 27)
Grade 1/2 Grade 3 Grade 1/2 Grade 3
Fatigue 15 (56) 4 (15) 15 (56)
2 (7)
Nausea 11 (41)
5 (19) 15 (56) 0
Vomiting 7 (26) 3 (11) 6 (22) 0
Headache 10 (37) 0 5 (19) 1 (4)
Constipation 6 (22) 0 8 (30) 0

Kaufman B et al. JCO 2015; 33(3)
Tumor Response Rates

Kaufman B et al. JCO 2015; 33(3)
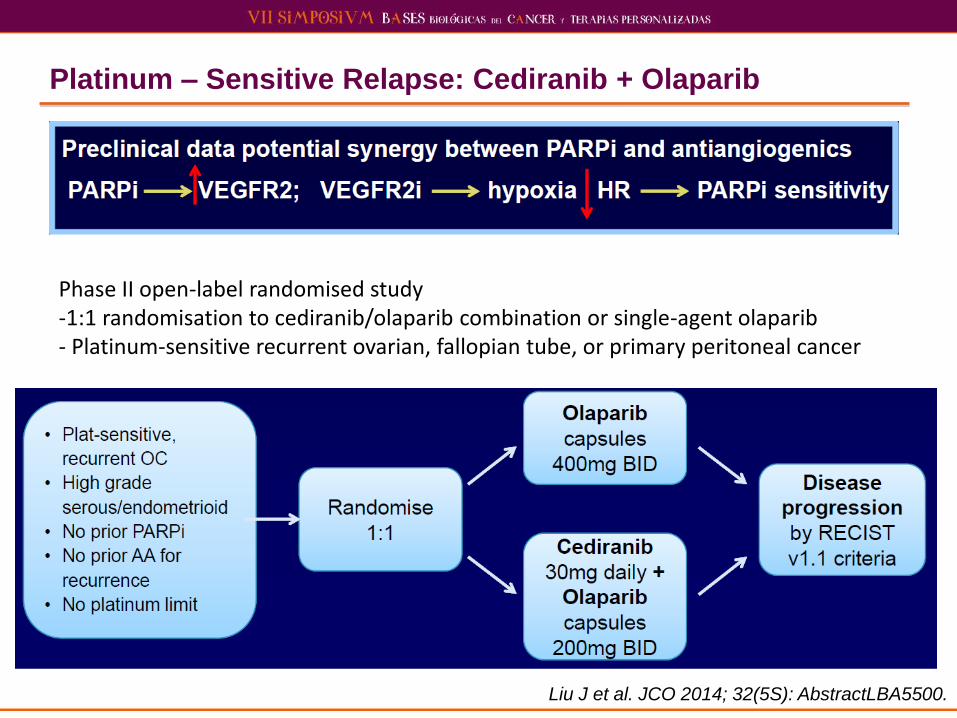
Platinum – Sensitive Relapse: Cediranib + Olaparib
Phase II open-label randomised study -1:1 randomisation to cediranib/olaparib combination or single-agent olaparib - Platinum-sensitive recurrent ovarian, fallopian tube, or primary peritoneal cancer
Liu J et al. JCO 2014; 32(5S): AbstractLBA5500.
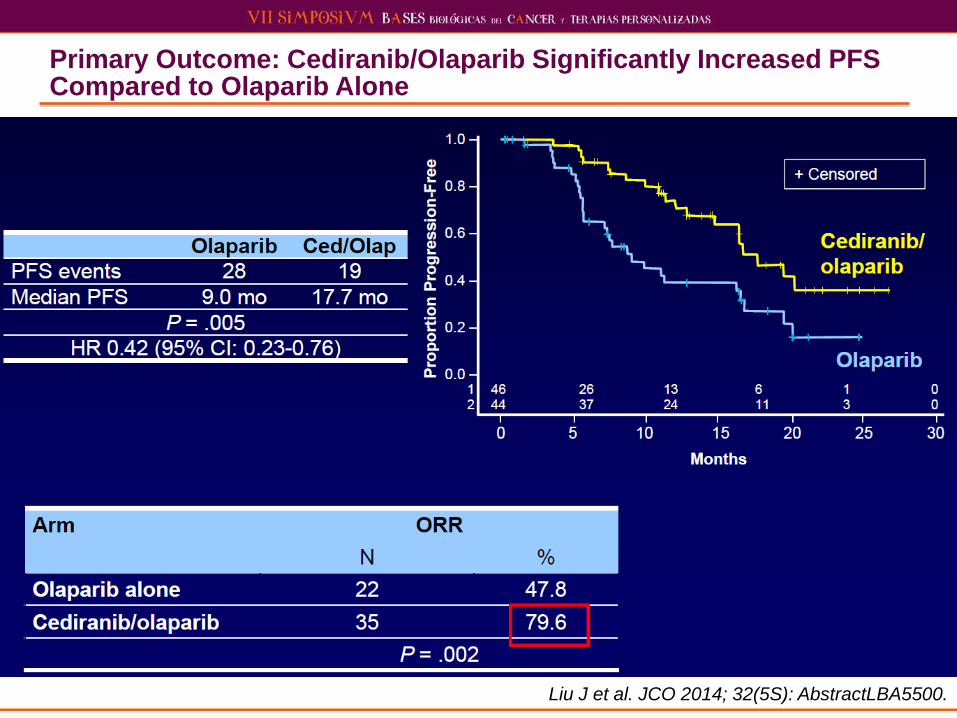
Primary Outcome: Cediranib/Olaparib Significantly Increased PFS Compared to Olaparib Alone
Liu J et al. JCO 2014; 32(5S): AbstractLBA5500.
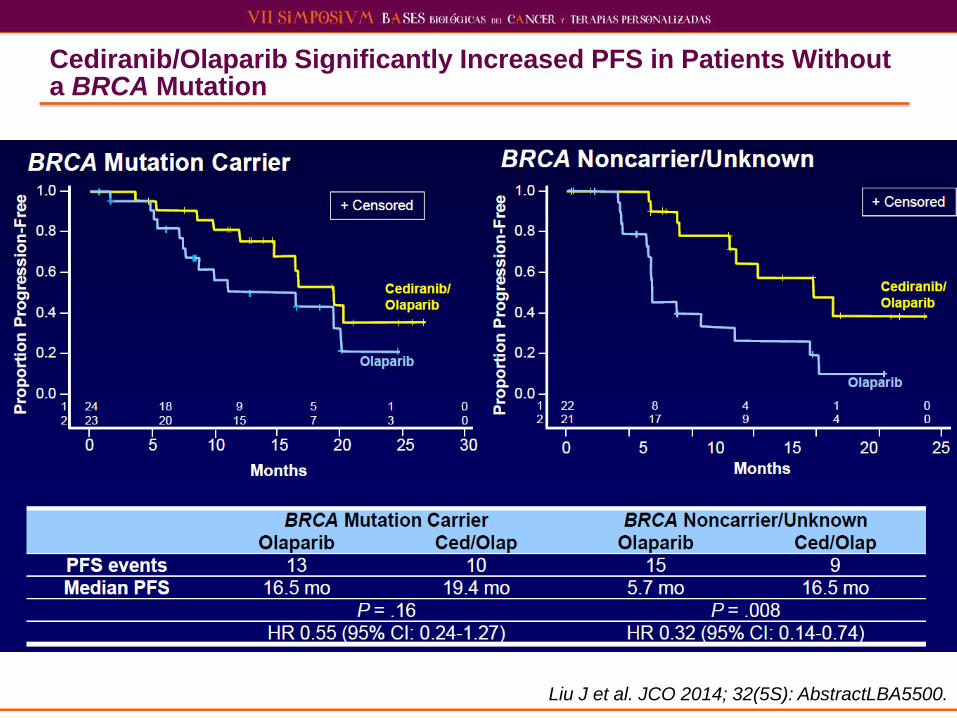
Cediranib/Olaparib Significantly Increased PFS in Patients Without a BRCA Mutation
Liu J et al. JCO 2014; 32(5S): AbstractLBA5500.
Response to Chemotherapy Post PARP Inhibitors in BRCA-Carrier Ovarian Cancer – Retrospective Study
78 patients (median 3 lines chemotherapy pre-olaparib) - Response rate RECIST 36%, PFS 17 weeks; OS 34 weeks
Responses to platinum post olaparib - Response rate RECIST 40%, PFS 22 weeks; OS 45 weeks
Responses observed regardless of pre-PARP
platinum-sensitivity
Platinum-to-platinum interval associated with response
to post-PARP platinum
In 6 cases tested, secondary mutations not observed
Ang JE et al. Clin Cancer Res 2013; 19(19): 5485-5493.
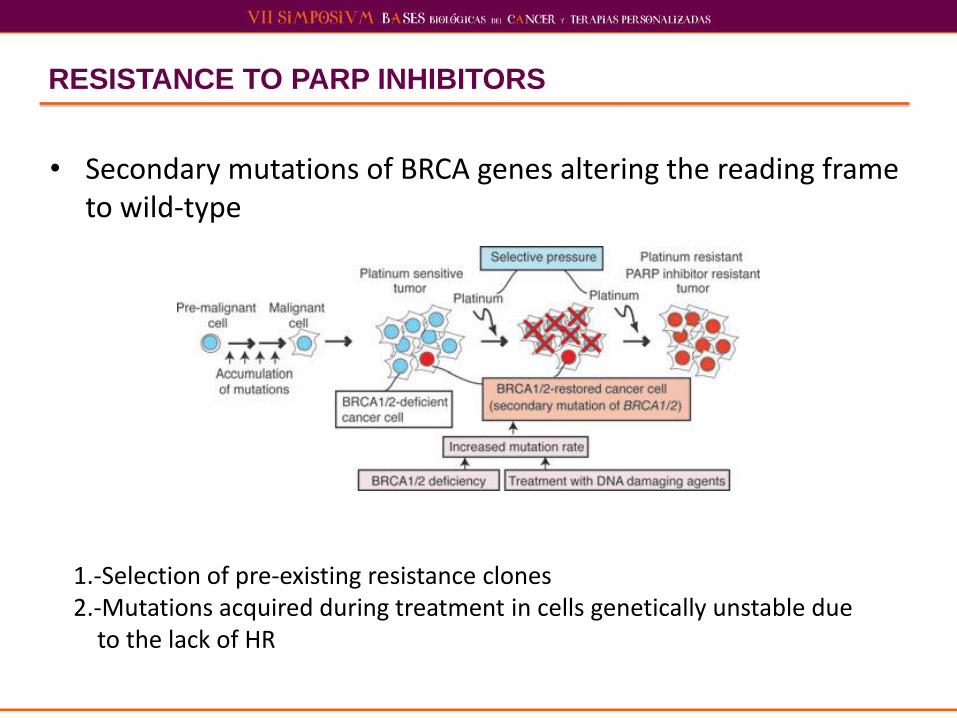
RESISTANCE TO PARP INHIBITORS
• Secondary mutations of BRCA genes altering the reading frame to wild-type
1.-Selection of pre-existing resistance clones 2.-Mutations acquired during treatment in cells genetically unstable due
to the lack of HR
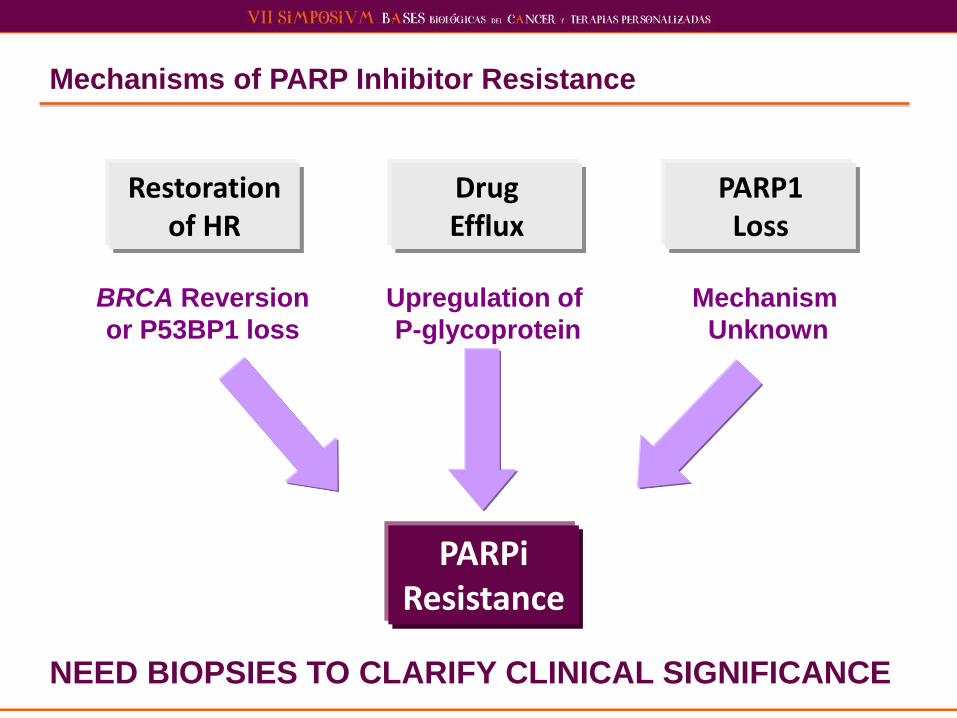
Mechanisms of PARP Inhibitor Resistance
Restoration of HR
Drug Efflux
PARP1 Loss
BRCA Reversion
or P53BP1 loss
Upregulation of
P-glycoprotein
Mechanism
Unknown
PARPi Resistance
NEED BIOPSIES TO CLARIFY CLINICAL SIGNIFICANCE

CONCLUSIONES
• BRCA es un biomarcador diferente (riesgo+predictivo)
• Es necesario una mejor definición del significado de la mutación germinal versus somática
• Las sales de platino (alquilantes?) parecen ser mas efectivas en presencia de mutación de BRCA
• Los inhibidores de PARP son eficaces en presencia de mutaciones de BRCA
• No es conocido si la eficacia es organodependiente
• Inhibidores de PARP+ QT+ farmacos antidiana +RT
• Adyuvancia/neoadyuvancia
• Toxicidad tardía

Might Platinum Response Be Predictor of Germline BRCA Mutation?
Alsop K, et al. JCO 2012; 30 (21): 2654-63
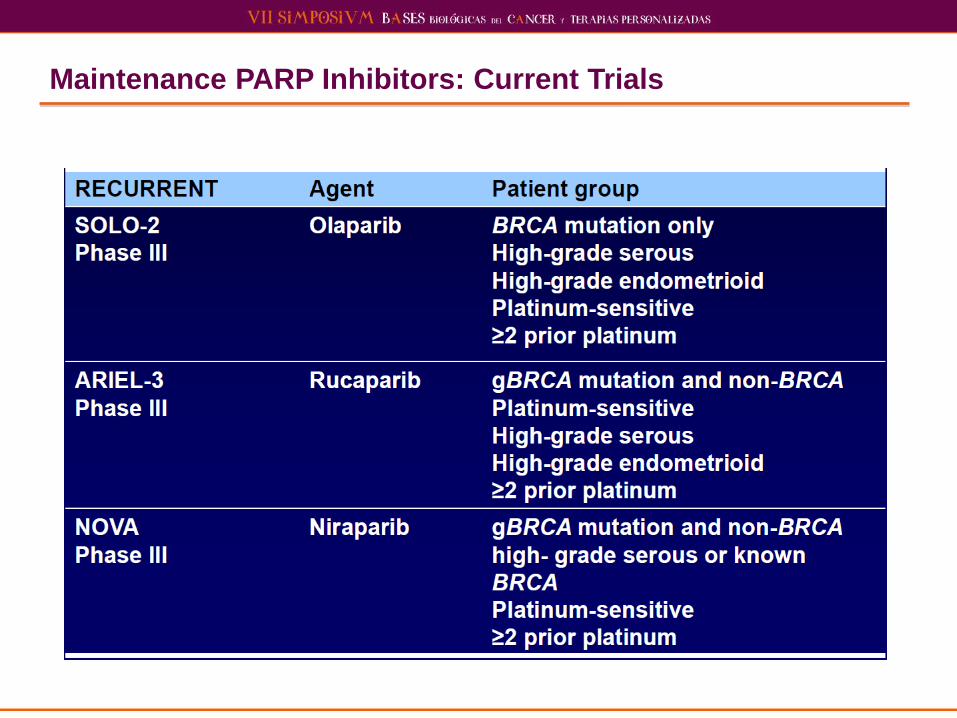
Maintenance PARP Inhibitors: Current Trials
Top Related