



Idiomas
Páginas
Jurídico

Versio
Titl
Titl
ProIdeDatProResObj
CoMa
MaHo
Th
No use or on 3.0 (22 Apr 2
e Page
le
otocol Versioentifierte of Last Veotocol search Quesjectives
untry(-ies) oin Author
rketing Authlder(s)
his study w
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
on
ersion of
stion and
of Study
horization
will be cond
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
Real Wo– OmbitaChronic HObservat
P15-743
n.a.
What is tproductivinterferonDasabuvsetting acRussian
AbbVie
ucted in colocal reg
vir and dasab
nfidential Informermitted witho
06.2015
rld Evidencasvir, ± DasaHepatitis C tional, Multi
, version 1.0
the effectivevity and hean-free regimvir, ± Ribavircross clinicaFederation
e Ltd
ompliance gulatory req
buvir
mation ut prior written
e of the Effeabuvir, ± Riin the Russ-Center Stu
0 dated 26.0
eness, patiealthcare resomen of Paritarin in patienal practice p
with this pquirements
n authorization
ectiveness obavirin in P
sian Federatudy
06.2015
ent reported ource utilizaaprevir/r – Ots with CHC
patient popu
rotocol ands
from AbbVie Pag
of Paritapreatients withtion- An
outcomes, ation of the Ombitasvir, C in a real lifulations?
d all applic
ge 1 of 61
evir/r
work
± fe
cable
NCT02669940
Versio
1.01.02.03.04.05.06.07.07.17.28.08.18.28.2.18.2.29.09.19.29.2.19.2.29.2.39.2.49.39.3.19.3.29.49.4.19.4.19.4.19.4.19.4.19.4.1
No use or on 3.0 (22 Apr 2
12
1234
12
11.11.21.31.41.5
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Table Table of AbbreviaResponsiAbstractAmendmMilestonRationalBackgrounRationale .ResearchResearch QObjectivesPrimary ObSecondaryResearchStudy DesiSetting .....Target PopStudy DuraTerminatioInvestigatoVariables .Primary VSecondaryData SourcData to be Inclusion DDuring TrePost-TreatmHCV RNAConcomita
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
of ConteContents
ations .....ible Partit ..............
ments andnes ...........le and Bacnd .................................
h QuestionQuestion ....s .................bjective ..... Objectives h Methodign ...............................
pulation ......ation ..........on Criteria ..or Selection ..................ariable ....... Variables .ces .............Documente
Documentateatment Docment Docum
A Sample ....ant Medicati
vir and dasab
nfidential Informermitted witho
06.2015
entss ...............................ies ............................ Updates.................ckground....................................n and Ob........................................................................s ........................................................................................................Criteria ............................................................................ed ...............tion ............cumentationmentation ....................ion .............
buvir
mation ut prior written
................
................
................
................
................
................d .....................................................
bjectives ..................................................................................................................................................................................................................................................................................................................................n ..........................................................................
n authorization
................
................
................
................
................
................
..................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
from AbbVie Pag
................
................
................
................
................
................
................
...................
...................
................
...................
...................
...................
...................
................
...................
...................
...................
...................
...................
...................
...................
...................
...................
...................
...................
...................
...................
...................
...................
...................
ge 2 of 61
...... 2
...... 5
...... 8
...... 9
.... 13
.... 13
.... 13
...... 13
...... 19
.... 20
...... 20
...... 20
...... 20
...... 21
.... 21
...... 21
...... 22
...... 22
...... 23
...... 23
...... 23
...... 24
...... 24
...... 24
...... 24
...... 24
...... 25
...... 26
...... 26
...... 28
...... 29
Versio
9.4.19.59.69.6.19.6.29.79.7.1
9.7.29.7.39.7.39.7.39.7.39.7.49.7.59.7.69.7.79.7.89.89.910.011.0
11.111.211.311.411.511.612.0
13.0Ann
No use or on 3.0 (22 Apr 2
1.6
12
1
233.13.23.345678
00
4
0
0nex 1.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
StandardizStudy SizeData ManaElectronic AssignmenData AnalyAnalysis PData .........DemograpEffectivenePrimary EfSecondaryStatistical MClinical LaPatient QuPSP and PATolerabilitInterim AsQuality CoLimitationProtectioManagemEvents/AAdverse EvSeverity ...RelationshSerious AdSerious anPregnancyPlans forResults ..ReferencEQ5D-5L
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
zed Assessme .................agement .....Case Repor
nt of Preferrysis ............
Population, T..................hics and Diess Analysiffectiveness EffectiveneMethods foaboratory D
uestionnairesAM ...........ty Analysis .ssessments .ontrol .........ns of the Reson of Humment and
Adverse Rvent Definit..................
hip to Pharmdverse Evend non-seriou Reporting .r Dissemin................ces ...........L .............
vir and dasab
nfidential Informermitted witho
06.2015
ment Tools ......................................rt Forms ....red Terms ....................Time Windo..................sease Charas ................
s Endpoint .ess Endpoinr Analysis o
Data .............s ........................................................................................search Methman Subje
ReportinReactions .
tion and Ser..................
maceutical Prnt Collectionus Adverse ..................nating an................................................
buvir
mation ut prior written
...................
...................
...................
...................
...................
...................ows and Ha...................acteristics .........................................
nts ...............of Effectiven..................................................................................................................
hods ............ects .........ng of Adve................rious Adver...................roduct ........n Period ......Event Repo...................
nd Commu................................................
n authorization
...................
...................
...................
...................
...................
...................andling of M...............................................................................................ness Variab.....................................................................................................................................................erse ................rse Event Ca.........................................................orting ............................unicating ................................................
from AbbVie Pag
...................
...................
...................
...................
...................
...................Missing ...............................................................................................bles ..................................................................................................................................................................
................ategories ...................................................................................................Study
................
................
................
ge 3 of 61
...... 29
...... 31
...... 31
...... 31
...... 32
...... 32
...... 32
...... 34
...... 34
...... 35
...... 35
...... 35
...... 37
...... 37
...... 39
...... 40
...... 40
...... 40
...... 41
.... 41
.... 42
...... 42
...... 44
...... 44
...... 44
...... 45
...... 45
.... 45
.... 47
.... 52

Versio
2.0
No use or on 3.0 (22 Apr 2
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Abbrevi
AE
APRI
AFP
ALT
AST
ABBVIE
REGIME
ANCOVA
BMI
CA
CD4
CHC
CI
CNI
CP
CPFSU
CT
DAA
DDI
EC
EDC
eCRF
EMA
EoT
EQ-5D-5
FDA
FIB-4
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
iations
adv
AST
alfa
alan
asp
EN
Par
A ana
bod
com
clus
chro
con
Cal
core
core
com
dire
dru
eth
elec
elec
Eur
end
5L Eur
Foo
Fib
vir and dasab
nfidential Informermitted witho
06.2015
verse event
T to platelet
a fetoprotein
nine-aminot
partate-amin
ritaprevir/r –
alysis of cov
dy mass ind
mpetent auth
ster of differ
onic hepatit
nfidence inte
cineurin
e population
e population
mputer tomo
ect-acting an
g-drug inter
ics committe
ctronic data
ctronic case
ropean Med
d of treatme
roQol 5 dim
od and Drug
rosis-4 Sco
buvir
mation ut prior written
t ratio index
n
transferase
notransferas
– ombitasvir
variance
ex
hority
rentiation 4
tis C
erval
n
n with suffic
ography
ntiviral agen
raction
ee
a capture
e report form
dicines Agen
nt
ension 5 lev
g Administra
re/Index
n authorization
x
se
r ± dasabuvi
cient follow-
nt
m
ncy
vel
ation
from AbbVie Pag
ir
up data
ge 5 of 61
Versio
No use or on 3.0 (22 Apr 2
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
γ-GT
HCC
HCP
Hb
HbA1c
HBV
HCV
HDL
HIV
HOMA
HVPG
ICMJE
IEC/IRB
IgA
IgG
IgM
INN
INR
LDL
LLoD
LLoQ
MAH
MedDRA
MLR
MRI
NCP
NS3/NS4
NS5A
NS5B
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
gam
hep
hea
Hem
hem
hep
hep
high
hum
hom
hep
Inte
inde
Imm
Imm
Imm
inte
inte
low
low
low
Ma
A Med
mul
mag
non
4A non
non
non
vir and dasab
nfidential Informermitted witho
06.2015
mma-glutam
patocellular
alth care pro
moglobin
moglobin A1
patitis B viru
patitis C viru
h-density lip
man immuno
meostasis m
patic venous
ernational C
ependent et
munoglobuli
munoglobuli
munoglobuli
ernational no
ernational no
w-density lipo
wer limit of d
wer limit of q
rketing Auth
dical Diction
ltiple logistic
gnetic reson
n-core popu
nstructural p
nstructural p
nstructural p
buvir
mation ut prior written
myltransferas
carcinoma
ovider
1c
us
us
poprotein
odeficiency
model asses
s pressure g
Committee o
thics comm
in A
in G
in M
on-proprieta
ormalized ra
oprotein
etection
uantification
horization H
nary for Reg
c regression
nance imag
lation
protein 3/no
protein 5A
protein 5B
n authorization
se
virus
ssment
gradient
of Medical Jo
ittee/- review
ary name
atio
n
Holder
gulatory Act
n
ing
nstructural
from AbbVie Pag
ournal Edito
w board
tivities
protein 4A
ge 6 of 61
ors
Versio
No use or on 3.0 (22 Apr 2
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
OATP
OLT
PAM-13
PCR
pegIFN
PRO
PSP
PT
RBV
RF
RNA
SAE
SAP
SD
SDP
SNP
SOC
SP
SVR
SVR12
SVR24
TAI
TP
TWP
VAS
WHO
WPAI
WPAI-G
WPAI-SH
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
org
orth
Pat
poly
peg
pati
pati
pre
Rib
rhe
ribo
ser
stat
stan
stud
sing
sys
safe
sus
SVR
SVR
tota
targ
tota
visu
Wo
wor
H WP
HP WP
vir and dasab
nfidential Informermitted witho
06.2015
anic anion-t
hotopic liver
tient Activat
ymerase ch
gylated inter
ient reporte
ient support
ferred term
bavirin
umatoid fac
onucleic acid
ious advers
tistical analy
ndard devia
dy designat
gle nucleotid
stem organ c
ety populati
stained virol
R at 12 wee
R at 24 wee
al activity im
get populatio
al work prod
ual analogu
orld Health O
rk productiv
PAI as gene
PAI modified
buvir
mation ut prior written
transporting
r transplant
ion Measure
hain reaction
rferon
d outcome
t program
ctor
d
se event
ysis plan
ation
ted physicia
de polymorp
class
on
ogical respo
eks after Eo
eks after Eo
mpairment
on
ductivity imp
e scale
Organization
vity and activ
ral health m
d for specific
n authorization
g polypeptid
e 13
n
an
phism
onse
oT
oT
pairment
n
vity impairm
measure
c health con
from AbbVie Pag
de
ment
ndition
ge 7 of 61
Versio
3.0
Stud
Vend
No use or on 3.0 (22 Apr 2
dy Designa
dor:
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Respo
ated Physic
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
onsible P
cian (SDP):
vir and dasab
nfidential Informermitted witho
06.2015
Parties
buvir
mation ut prior writtenn authorization from AbbVie
Pagge 8 of 61

Versio
4.0
TitleReal in PaStudRatioThe (ABBshowexcluThe FedeThe ABBVsettinmeasenvirachieexcluper lowith EffectheremakeThis RBVclinicDurinstandrespopatiemostpegIFwereobsepredassisfutureThe genouse aof ad
No use or on 3.0 (22 Apr 2
: World Evideatients with Cy onale and Binterferon-fre
BVIE REGIMwn to be safeusion criteria ABBVIE RE
eration for therationale forVIE REGIMEngs, which msure of theronment, suceves its intenusion criteria ocal label whsignificant coctiveness resefore be morers. observationa, used accor
cal practice png the last ddard of careonse and th
ent care for Ct likely to resFN/RBV and
e not predictivervational stuictive factorsst in further oe. label of the
otype/subtypeand outcomedherence on
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Abstra
ence of the EChronic Hepa
ackground:ee combinatiEN) ± ribavie and effectiunder well cGIMEN is exe treatment or this observEN as demonmeans evalu capacity o
ch as in a rannded effect in
and will invohich might incomorbid condsearch allowsre relevant fo
al study is thrding to locapatient populadecade whene for the treahe subsequeCHC. As a pond. Interes first generatve of outcom
udy may plays of responseoptimizing tre
e ABBVIE Re and stage oe in daily clin
treatment o
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
act
Effectivenessatitis C in the
on regimen orin (RBV) forve in random
controlled conxpected to bof CHC in 20vational studynstrated in puating its efof a treatmendomized conn the usual clolve the broaclude patientditions and cos for externaor health-car
he first effectl label, undeation. n dual theraatment of CHent developmconsequencestingly, manytion direct ac
me in the devy an importae that are impeatment with
REGIMEN ± of liver disea
nical practiceutcomes in e
vir and dasab
nfidential Informermitted witho
06.2015
of Paritapreve Russian Fe
of Paritaprevr the treatmemized contronditions. be first availa15. y is to deter
pivotal trials tffectiveness. ent to prodntrolled trial, linical settingader patient pts with heteroould be used
al patient-, prre decisions
iveness reseer real world
py with pegyHC, the discment of treate, treatment y of the now cting anitviralsvelopment triant part in briportant in reah the interfer
RBV will vaase. It is there. In addition,everyday set
buvir
mation ut prior written
vir/r – Ombitaederation – A
vir/r – ombitaent of chronicolled clinical
able IFN-free
rmine how thtranslates intWhereas ef
uce the deeffectiveness
g. Effectivenepopulations iogenous comd to model anrovider-, and by both pro
earch examinconditions in
ylated interfecovery of pretment algoritcould be ef
well establiss (DAAs) in cals of the ABidging the daal world treatron-free ABB
ary accordingefore relevan this study wttings, which
n authorization
asvir, ± DasaAn Observat
asvir with or wc hepatitis C trials with st
e combinatio
he efficacy ato real world fficacy can
esired effect s is the exteness trials typiin routine clin
mpliance pattnd dissemina
system-leveviders in pra
ning the ABBn the Russia
eron (pegIFNedictive factothms markedffectively targ
shed predictocombination
BBVIE REGIMata gaps. It tment settingBVIE REGIM
g to hepatitint to understawill provide da
may help tre
from AbbVie Pag
abuvir, ± Ribational, Multice
without dasa(CHC) has
trict inclusion
on in the Rus
and safety oeveryday clbe defined
in a contrnt to which a cally have limnical practiceerns and pat
ate best practel factors andactice and po
BVIE REGIMn Federation
N) plus RBVors for virolod a milestongeted to pat
ors of responwith pegIFN/
MEN ± RBV.may help ides and thus, cEN ± RBV in
s C virus (Hand the patteata on the imeating physic
ge 9 of 61
avirin enter
abuvir been
n and
ssian
of the inical as a rolled drug
mited e and tients tices. d can olicy-
EN ± n in a
V was ogical ne in tients se to /RBV This
entify could n the
HCV) ern of mpact cians
Versio
to imThe outcoin a rReseWhautilizasettin Prim
Seco
StudThis ABBVThe local preceTargPatie
VariaPrim
No use or on 3.0 (22 Apr 2
mprove the maaim of this oome, work prreal world seearch Questt is the effecation of the ng across clin
ary Objective1. To d
ABBVvirolo
ondary Objec2. To pr3. To co
popu4. To de5. To d
produ6. To d
utilizady Design:
is a prospecVIE REGIMEprescription clinical praedes the dec
get Populatioents are eligib Treatmen
genotypeRBV acco
If RBV iswith the contraind
Patients study
Patient mtherapeu
ables: ary Variable The perc
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
anagement oobservationalroductivity antting across tion and Objctiveness, painterferon-fre
nical practice
e describe in VIE REGIMogical responctives rovide real wollect informa
ulation escribe the to
document theuctivity in theetermine theation
ctive, multi-cEN ± RBV. of a treatme
actice and lacision to offeron:ble for observnt-naïve or -e 1, receivingording to stas co-adminiscurrent loca
dication durinmust volunta
must not be ptic trial
centage of pa
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
of patients un study is to pnd healthcareclinical practjectives:
atient reporteee ABBVIE e patient pop
routine clinicEN ± RBV
nse at 12 wee
world evidencation on co-m
olerability of e effect of te Russian poe impact of th
center observ
ent regimen isabel, is madr the patient t
vation in this-experiencedg combinationndard of care
stered with thal label (withng pregnancyarily sign and
participating o
atients achiev
vir and dasab
nfidential Informermitted witho
06.2015
nder their carprovide evidee resource utice patient po
d outcome, wREGIMEN ±ulations?
cal practice in patients
eks after end
ce for predictimorbidities an
the ABBVIE the ABBVIE pulation he ABBVIE R
vational stud
s at the discde independthe opportun
s cohort if thed adult male n therapy wite and in line he ABBVIE R special atte
y) d date an in
or intending t
ving SVR12
buvir
mation ut prior written
re. ence of the etilization of thopulations.
work product± RBV in pat
the effectivwith CHC
d of treatmen
ve factors ofnd concomita
REGIMEN ±REGIMEN
REGIMEN ±
dy in patients
retion of the dently from tity to particip
e following apor female p
th the interferwith the currREGIMEN, itention to con
formed cons
to participate
(HCV RNA <
n authorization
effectivenesshe ABBVIE R
tivity and heatients with C
veness of thas evidencet (SVR12)
f virological reant medicatio
± RBV ± RBV on
RBV on hea
s receiving th
physician inthis observapate in this st
pplies: patients with ron-free ABBrent local labt has been pntraception r
sent prior to
in a concurr
<50 IU/mL 1
from AbbVie Page
s, patient repREGIMEN ±
althcare resoCHC in a rea
he interferoned by susta
esponse on in the Rus
PROs and
althcare reso
he interferon
n accordanceational study tudy.
confirmed CBVIE REGIMel prescribed inrequirements
inclusion into
rent intervent
2 weeks [i.e
e 10 of 61
orted RBV
ource al life
n-free ained
ssian
work
ource
n-free
e with y and
CHC, EN ±
n line s and
o the
tional
. ≥70
Versio
DataSourdata StudIn phat leaexpeREGpopu
As owidthleastenro
DataThe abovtheir labelsufficRNA≥50 but ndue tinform(eCRpopuREGDescbasegrouare rweekinto specThe
No use or on 3.0 (22 Apr 2
days] afte Secondar Co-morb Serious a Question
work proinitiation,
PAM-13, a Sources: rce documenin his/her ow
dy Size: hase III studiast 90% wer
erienced patieGIMEN ± RBulation of this
bvious from Th of the 95%t 95%, then 9lled during th
a Analysis: core populat
ve), who havedisease cha
will be summcient follow-u
A data ≥70 daIU/mL at theno HCV RNAto reasons remation (e.g.
RF) but dateulation (SP)
GIMEN. criptive and eeline and diseps (based onrelevant for sks). In additiosubgroups.
cified in the stprimary effe
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
er the last acry Variables idities and coand non-serionnaires on PRoductivity an at EoT as wPSP satisfac
nts are definewn patient file
es investigatre observed, ents). To deV in patients
s study should
Table 3, if th% confidence94 patients ahe inclusion p
tion (CP) is de started thearacteristics.marized in thup data (CPSays after the e last measurA measuremelated to safevirologic fail
e and valueis defined a
exploratory sease charactn genotype 1scheduled treon, baseline sFurther detatatistical anaectiveness a
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
ctual dose of
oncomitant mous adverse ROs: EuroQnd activity imwell as 12 andction and util
ed as origines which will
ting the intereven in difficscribe in rous with CHC,d be achieve
he SVR12 rate interval (CIare sufficient period of 8 m
defined as ae treatment co Patients no
he non-core pSFU) is defilast actual dorement or (iiient ≥70 daysety (e.g. dropure such as
e of the coras all patien
tatistical metteristics will b1 subtype, fieatment comsummaries wails of analylysis plan (SA
analysis will
vir and dasab
nfidential Informermitted witho
06.2015
the ABBVIE
medication events and pol 5 dimensimpairment (d 24 weeks alization quest
al documentserve as sou
rferon-free ABcult-to-treat Cutine clinical , a precise e
ed.
te is at least ) will not befor a width o
months.
ll patients ofombination rot receiving population (Nned as all Cose of the ABi) had HCV Rs after the lapped out duerelapse is re
rresponding nts who rece
thods will be be summarizebrosis status
mbination (± dwill be repeatysis populatioAP). be performe
buvir
mation ut prior written
REGIMEN)
pregnancy ocion 5 level (E(WPAI) quesafter EoT tionnaires
ts. The invesurce data for
BBVIE REGICHC patientspractice the estimate of t
90%, then wwider than
of 10%. Ther
f the target precommendethe treatmen
NCP). In addCP patients, BBVIE REGIRNA <50 IU/ast actual doe to adverse eported in thHCV RNA eived at lea
used to anaed for the CPs, treatment dasabuvir, ±ted for the SPons and the
ed for CP p
n authorization
ccurrences EQ-5D-5L) qstionnaire pr
stigator will dthe study.
IMEN ± RBVs (e.g. cirrhot
effectivenesthe SVR12
with 158 evalu10%. If the
refore, 158 p
population (Ted in the currnt recommen
dition, the corwho have (iMEN or (ii) a/mL at the la
ose of the Aevent) or inc
he electronic test is missst one dose
alyze the dataP stratified byexperiencedRBV) and d
P and TP wit CP analysi
patients, stra
from AbbVie Page
questionnairerior to treat
document pa
V, SVR12 rattic G1a treatss of the ABrates in the
uable patientSVR12 rate
patients shou
TP) (definitionrent local labnded in the re populationi) evaluable a HCV RNA vast measuremBBVIE REGIcomplete effcase report
sing). The se of the AB
a of the study the CP ana or naïve), w
duration (12 othout stratificis groups w
atified by the
e 11 of 61
e and tment
atient
tes of tment BVIE core
ts the is at ld be
n see el for local
n with HCV
value ment, MEN
ficacy form
safety BVIE
y. All alysis which or 24
cation ill be
e CP

Versio
analyrelaprelapsufficall pmeasall raPearUnivaof vatype expewill beachpatieanalywill correcovaalso All smethMilesStartEnd Final
No use or on 3.0 (22 Apr 2
ysis groups. pse rate, virapse rates wilcient HCV RNpatients of tsurement onates specifiedrson method.ariate and m
arious explanof treating
erienced patiebe performedh patient groent groups haysis. Backwaconsider on
esponding unariates to stay
be used to insafety variabhods stratifiedstones: t of Data Collof Data Collel Report of St
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Response al breakthroul be estimateNA measurehe CP ana treatment ad above 95%.
multiple logistinatory covariainstitution, aents) on SVRd for various Coup. Furthermas to be take
ard selection nly covariatenivariate logy in the modnvestigate thebles will be d by the type
lection: ection: tudy Results
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
rates (i.e. Sugh) will be ed in patientments post tlysis groups
and at least o%-confidence
ic regressionates (e.g. dend prior trea
R12. These aCP analysis more, the faen into accoprocedures wes in the sgistic regressel in a backwe impact of tsummarized
e of combinat
JA
: M
vir and dasab
nfidential Informermitted witho
06.2015
SVR12 rate, determined ts of the CPtreatment. Vis, who haveone on-treatme intervals (C
n (MLR) methmographic aatment for Canalyses will groups since
act that treatount, when sewill be applieselection prsion analysisward eliminatreatment adh
d for patientstion treatmen
an 2016 Aug 2017 May 2018
buvir
mation ut prior written
end of treafor the vario
P analysis groral breakthroe at least oment or EoT
CIs) will be d
hods will be und disease c
CHC and resbe of explor
e not each cotment regimeelecting the
ed to generatrocedure wits. A p-valuetion step. Loherence on Ss in the SP
nt and schedu
n authorization
atment [EoTous CP analoups with Eo
ough rates wione undetec
measuremeetermined us
used to invescharacteristicsponse outcoratory nature,ovariate mighens will diffepatient grou
te the final Mth a p-valu
e <0.05 will gistic regres
SVR12. P using desculed treatme
from AbbVie Page
T] response ysis groups.oT responseill be estimat
ctable HCV ent thereaftersing the Clop
stigate the imcs, co-morbidome in treat, data drivenht be predictier in the vaps for each
MLR models wue <0.25 in
be used fosion method
criptive statisnt duration.
e 12 of 61
rate, The
e and ted in RNA
r. For pper-
mpact dities, tment , and ive in
arious MLR
which n the r the s will
stical
Versio
5.0
6.0
7.0
7.1
Infecmortcarcmanand estimindivrangsom
HCVmajoglobmoreCentHCVinfec
HCVfrequinfeccan scre
No use or on 3.0 (22 Apr 2
None
Start of D End of D Final Re
ction with thtality [1] and
cinoma (HCy countriesgo on to
mated 2-3%viduals [5] [6ging from 0e regions o
V demonstraor genotypeally [11]. Gee restricted tral Africa, a
V genotypesctions world
V is primarilyuently by injction-controalso result iening proto
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Amend
Milest
Data CollecData Collecteport of Stud
Ration
Backgr
he hepatitisd is a leadin
CC), as wels [2]. Arounddevelop ch
% of the w6]. The prev.1-1% in Wf Eastern E
ates a high des (and a larenotypes 1 distribution
and Egypt; gs 1a and 1b wide [12] [1
y transmittejection drugl practices (in transmiss
ocols have b
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
dments a
ones
ction: tion: dy Results:
nale and
round
C virus (Hng cause ofl as the md 60-85% o
hronic diseaworld’s popvalence var
Western Eururope [7] [8
degree of grge number through 3 a, genotype 4genotype 5 are the mo
13] [14] [15]
d by parentg use, expos(tattoo, piercsion of HCVbeen introdu
vir and dasab
nfidential Informermitted witho
06.2015
and Upda
Jan 2016Aug 2017May 2018
Backgro
HCV) is assof chronic livost commoof subjects ase [3] [4]. ulation - eries markedrope to 1-28] [9] [10].
enetic variaof subtypes
are found wo4 is found pin South Afst common .
teral exposusures in heacing). Occu
V [16] [17]. Suced in mos
buvir
mation ut prior written
ates
6 78
ound
ociated wither disease,
on indicationexposed toChronic he
qualing apdly from one% in Latin
ability and hs) the distriborldwide; thpredominantfrica; and geforms, acco
ures to contalth-care sepational, pe
Since the east countries
n authorization
h consideracirrhosis, a
n for liver o HCV do nepatitis C (proximately
e geographiAmerica an
as been clabution of whe other gently in the Mienotype 6 mounting for 6
aminated bttings and in
erinatal and arly 1990’s rand as a co
from AbbVie Page
able morbidiand hepatoctransplanta
not clear the(CHC) affey 130-210 ic area to and up to 4
assified into hich varies notypes haveddle East,
mainly in Asi60% of HCV
lood, most nadequate sexual exp
routine blooonsequence
e 13 of 61
ity and cellular tion in e virus cts an million
another .9% in
seven
e a
ia. V
osure od e

Versio
transthrou
The cirrhindivdevehepadeveexpelineapatiewith (HIVCHC
The uponof inincreincrethanindiv
The seru(sus[27] afore
Achito papatiecausthe l(p<0rate SVRor wrelat
No use or on 3.0 (22 Apr 2
smission of ugh organ t
natural couhosis of the lviduals [18].elop hepaticatorenal synelop HCC [1ected to reqar process aent, durationother viruse
V) [4] but alsC treatment
burden of an several fafection) of tease in the iease. In per in other ag
viduals with
eradicationum (as showtained viroloand is geneementioned
ieving an SVatients who ents: 6.7% vse mortality iver-related
0.001), the rof patients
R [29]. Patiewithout RBV ted death in
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
the virus is ransplants.
urse of CHCliver over th Once patie
c decompenndrome, or h19]. Over theuire liver tra
and can be an of HCV infes such as
so by concoeligibility, s
advanced livctors includhose infecteincidence orsons 30–49ge groups. B
CHC are ex
of the viruswn by a sensogical respoerally accepd complicatio
VR was assdid not ach
vs 14.4%, rerate was 8. mortality o
rate of HCCexperiencinnts with SVhave also s several stu
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
rarely seen
C leads to prhe course ofents becomensation (aschepatic synte same timeansplantatioacceleratedfection, malhepatitis B vmitant steatafety, tolera
ver disease ding chronic ed [23]. Duef severe live
9 years of agBy 2020, thexpected to i
s, defined asitive test) aonse [SVR])pted as a virons [26] [27
sociated withhieve SVR (5espectively).9% in patier transplant was 5.1% w
ng liver failuVR following shown improudies [30] [3
vir and dasab
nfidential Informermitted witho
06.2015
n following r
rogressive fif 20-30 yeare cirrhotic, a
cites, encephthetic dysfue frame, beton or die [19d by a numble gender, avirus (HBV)tosis and obability and e
varies wideHCV preva
e to an aginer disease, ge, the prev
e rates of HCincrease by
s the absenat the end o), is the therrological cur7].
h significant5-year mort) [28]. In ano
ents with SVtation was 1with and 21re was 2.1%treatment w
ovement in 31] [32]. Mor
buvir
mation ut prior written
receipt of blo
ibrosis and rs in approxaround 6% phalopathy, vnction) andtween 4 and9] [20]. Progber of factorsalcohol cons) and humanbesity. Com
efficacy of th
ely across calence and ag cohort of the burden valence of thCC and live 81% and 1
nce of HCV f treatment rapeutic goare, thus, eve
t reduction itality rate in other study
VR and 26.0.9% with SV.8% withou
% with and 2with pegylatliver histoloreover, patie
n authorization
ood, blood p
can eventuximately 15-per year arevariceal hem around 3%d 5% of patgression is ns including tsumption ann immunode
morbid condiherapy [21] [
ountries andage distribupatients anof CHC willhe disease
er-related de80%, respe
ribonucleic (EoT) and 1al of CHC trentually prev
in all-causeHCV genotthe 10-year% without SVR and 27.4t SVR (p<029.9% (p<0ted interfero
ogy and a reents with co
from AbbVie Page
products or
ally lead to -30% of infee expected morrhage,
% per year wients can benot necessathe age of t
nd co-infectieficiency virtions can im[22].
d is dependtion (and dud an associl continue tois 3–fold hig
eaths amongectively [24]
acid (RNA)12-24 weekreatment [25venting the
death comtype 1-infecr cumulativeSVR (p<0.004% without .001), and t
0.001) withoon (pegIFN) eduction in lompensated
e 14 of 61
ected to
will e arily a the on
rus mpact
dent uration iated o gher g .
) in ks later 5] [26]
pared cted e all-01), SVR
the ut with iver-d

Versio
cirrhdecotwo-
In thHowwas [36] but sintro[i.e. beenvaryrequratesgeno
Treatoxic
In 20boce(FDAThesrepo[44].comspecTrearules
Sinceithesimesofo
Sime2013naïvwere[47]
No use or on 3.0 (22 Apr 2
hosis who acompensatiothirds [33] [
e 1980’s anwever, the ef
generally u[37]. Comb
still overall roduction of lopegIFNs]) in made in e
y substantialuiring longers up to arouotypes 2 an
atment with cities includi
011 the firsteprevir and A) and the Ese first gene
orted as high However, tbination thecific adverseatment regims and a resp
ce 2014 the er the nonsteprevir or thsbuvir [45]
eprevir is a 3 and by thee patients we eligible for[48]. Very s
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
chieve SVRn, may achi34] [35].
nd 1990’s inffectiveness
unsatisfactorination therrates acrossong-acting in combinati
efficacy with lly by HCV gr treatment pund 50% cand 3 cure rat
pegIFN anding cytopen
t direct-actintelaprevir, h
European Meration DAAh as 63-75%these DAAserapy and the effects sucmens with thponse guide
new standatructural proe nucleotide[46].
NS3/4A proe EMA in Mwith genotypr truncated tsimilar resul
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
R essentiallyieve histolog
nterferon alfs of interferory resulting rapy with ints genotypesinterferons ion with RBVoverall rate
genotype wperiods to on be achievtes of up to
d RBV is asias, neuro-p
ng antiviralshave been a
Medicines AgAs have sign% among tres must be ushe tolerabilitch as rash, hese DAAs ed therapy d
ard of care fotein 3/nonse nonstructu
otease inhibay 2014. In pe 1 yieldedtherapy of 2ts were rep
vir and dasab
nfidential Informermitted witho
06.2015
y eliminate thgic regressi
fa was the fion monothein an overa
terferon pluss remained (peginterferV more thanes of SVR u
with genotypeobtain SVR wved in patien80% can be
sociated wipsychiatric d
s (DAAs), spapproved bygency (EMAnificantly imeatment-naïsed in combty profile is fpruritus, dyare rather c
duration of u
for genotypestructural proural protein
bitor which wthe phase
d SVR rates24 weeks in orted for pa
buvir
mation ut prior written
heir subseqon, and dec
rst drug to serapy in the all SVR rate s ribavirin (Rbelow 50% ron alfa-2a an a decade p to 54-63%e 1 being thwith interfernts with gene achieved
th consideradisorders an
pecifically thy the US FoA) for treatmproved efficïve HCV gebination withfurther impa
ysgeusia ancomplicatedup to 48 we
e 1 is pegIFotein 4A (NS5B (NS5B)
was approveIII studies Q
s of 80%, aro a response
atients with p
n authorization
quent risk ofcrease their
show activittreatment oacross gen
RBV) improv[38] [39]. Fo
and peginteago, furthe
% [39] [40] [4he most diffiron-based d
notype 1 wh[41].
able, often tnd influenza
he protease ood and Drument of HCVcacy with ranotype 1 indh pegIFN anaired by addd anemia [4
d with the neeks in selec
FN and RBVS3/4A) prot polymerase
ed by the FDQUEST 1 anound 90% oe guided treprior relapse
from AbbVie Page
f r risk of HCC
ty against Hof CHC infecnotypes of <ved SVR raollowing the
erferon alfa-r advances 41]. SVR raicult-to-treatdual therapyereas for
treatment-lia-like sympt
inhibitors ug AdministrV genotype 1tes of SVR dividuals [42nd RBV as tditional DAA42] [43] [44]ecessity of fcted patients
V combined tease inhibite inhibitor
DA at the ennd 2 treatmeof these patatment sette in the
e 15 of 61
C by
HCV. ction
<20% ates e 2b have
ates t, thus y. SVR
miting toms.
ration 1.
2] [43] triple A .
futility s.
with tor
nd of ent-tients ing

Versio
PROresptelap54%with evenNotaQ80signwith pres
Sofopoly2014geno
In thgenoin geRBVjust
DatapatieincorepopegI
Thusand the lcom
Compoteincresafetreatwith disea
No use or on 3.0 (22 Apr 2
OMISE trial ponder patieprevir plus p
%, respectiveregards to
nts (SAEs) wably, amongK polymorpificantly redHCV genot
sent, conside
osbuvir acts merase. It w4 for treatmeotype 2 and
e NEUTRINotype 1, 4, 5enotype 1b; V. One furthe12 weeks [5
a on the inteents with gensistent. Wh
orted and thFN [45] [46
s, currently there is a cikelihood ofponents of
mbinations oential to signeasing SVRty and tolertment algoricombinatioase.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
[49]. In the Aents were rapegIFN and ely) the safeanemia (13were reporteg patients inphism (pre-euced respotype 1a are eration is gi
as an RNAwas approveent of geno 3 patients
NO phase II5 and 6 pati 80% in cirrer advantag52].
erferon-free enotype 1 arhen given fois regimen i
6] [53] [54].
available aplear unmet f successfulCHC therap
of multiple Dnificantly imp
R rates, elimrability of treithm. In add
on DAA regim
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
ATTAIN stuandomized t
RBV. Althoety profile of% vs. 37%)ed by 2% afected with
existing resisonse rates a
screened foiven to selec
A chain termed by the FDtype 1, 4, 5as an interf
I trial with sents, the ov
rhotic patienge of this trip
combinatiore only avaior a duratiois currently
pproved treaneed for effl treatment apy, ideally w
DAAs targetiprove CHC inating inter
eatment, shodition, wider mens could
vir and dasab
nfidential Informermitted witho
06.2015
udy 771 treato either simough efficacf simeprevir) and pruritund 9% of paHCV genotstance-assond thus, it isor this mutacting an alte
minator withiDA in Dece, and 6 alon
feron-free re
sofosbuvir pverall SVR wnts) with a tople treatme
on of sofosblable from sn of 24 weeonly recom
atment regifective anti-and/or decr
with shorter
ing differenttreatment c
rferon as a cortening durapplication
d significantl
buvir
mation ut prior written
atment-expemeprevir plus
y rates werer was signifius (31% vs.atients, resptype 1a the ociated varis recommen
ation, and if ernative the
n the catalymber 2013
ng with pegIegimen with
lus pegIFN/was 90% (9olerability prnt regimen
uvir plus RBsmall trials aeks SVR ratmended for
mens are nHCV compo
rease the netreatment d
t steps of vircompared tocomponent ration of the of DAA they reduce th
n authorization
erienced pas pegIFN ane similar (SVcantly impro43%), while
pectively [50presence oant or not) rnded that pathe respect
erapy [51].
ytic site of thand by the IFN plus RB RBV only.
/RBV in 3262% in genorofile similaris the treatm
BV in treatmand results aes of 50-68r patients wh
ot optimal foounds whicheed for pegIduration.
ral replicatioo current theof therapy,
erapy and sierapy and bee public hea
from AbbVie Page
rtial and nulnd RBV or VR was 55%oved, in pare serious ad0]. f a commonresults in atients infective variant i
he NS5B EMA in Jan
BV and in
6 treatment-otype 1a andr to pegIFN ment duratio
ment-naïve are somewh% have beeho cannot ta
or many pah can increaFN as
on have theerapies by increasing
implifying thetter responalth burden
e 16 of 61
ll-
% and rticular dverse
n
cted is
nuary
-naïve d 82% plus
on of
hat en ake
tients ase
e
the he nses of this

Versio
AbbVdiffewith inhibparitdrugnons(ABTvitro
The has (SAPTUR
Therfollow
Tabl
Poputreat
Non-treat(12 w
Non-treatexpe(12 w
Thesgeno
The tradigenoexpe
No use or on 3.0 (22 Apr 2
Vie's interferent steps inanomolar
bitor of the ctaprevir, ritog exposuresstructural prT-333) is a N.
3 DAA combeen initiallPPHIRE-I [5
RQUOISE-II
rapy for 12 wwing SVR r
le 1 - SVR1
ulation and tment durat
-cirrhotic, tment-naïveweeks)
-cirrhotic, tment-erienced weeks)
se results sotype 1a inf
TURQUOISitionally mosotype 1 infeerienced ind
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
eron-free regn HCV replipotency in
cytochrome onavir co-ads than adminrotein 5A (NNS5B non-n
mbination of y evaluated
56], SAPPH [60]).
weeks with rates 12 wee
2 rates in c
ion Geno
e 1a
1b
1a
1b
uggest that fected patien
SE-II [60] stst difficult-tocted patient
dividuals. Al
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
gimen for thication. Parivitro and is P-450 enzy
dministrationnistration of
NS5A) inhibinucleoside p
paritaprevird in 6 Phase
HIRE-II [57],
the above reks after Eo
clinical tria
otype SVAB
95-(SA
98-(SA
96%(SA
97%(SA
the ABBVIEnts, while p
tudy exploreo-treat cirrhots with cirrhl patients re
vir and dasab
nfidential Informermitted witho
06.2015
he treatmentitaprevir (ABco-adminis
yme CYP3An with paritaparitaprevitor with picopolymerase
r/r – ombitase III studies PEARL-II [5
regimen in noT (SVR12)
als:
R12 BVIE REGI
-97% APPHIRE-I,
-99.5% APPHIRE-I,
% APPHIRE-II
% APPHIRE-II
E REGIMENatients with
ed the efficaotic patientsosis, includ
eceived the
buvir
mation ut prior written
t of CHC incBT-450) is astered with lA4. As a phaaprevir (paritr alone [55]omolar potee inhibitor wi
svir plus dwith genoty58], PEARL
non-cirrhotic:
MEN + RBV
PEARL-IV)
PEARL-III)
)
, PEARL-II)
N with RBV genotype 1
acy of the ABs. This largeing treatmeABBVIE RE
n authorization
cludes 3 DAa NS3/4A prow-dose ritoarmacologictaprevir/r) re. Ombitasvi
ency in vitroith nanomol
asabuvir withype 1 infecteL-III [59], PE
c patients re
VSVR12 ABBVIE
) 90% (PEARL
) 99% (PEARL
n.a.
) 100% (PEARL
is the optim1b do not re
BBVIE REGe study enront-naïve an
EGIMEN wit
from AbbVie Page
AAs targetinrotease inhionavir, an c enhancer esults in higr (ABT-267), and dasablar potency
h or withoued patients
EARL-IV [59
esulted in th
E REGIMEN
L-IV)
L-III)
L-II)
mal regimenequire RBV.
GIMEN in tholled exclusind treatmentth RBV and
e 17 of 61
ng bitor
of gher ) is a buvir in
t RBV
9],
he
N alone
for
e ively t-
d were

Versio
randSVRdemto th12 w93%resptreatrespweehighand
The Phascirrhtolermanof Rcom(ALTdysfthe ccontwith ALT obseof thby pof treBiliruof in
Resptreatombwitho
Thesmigh
No use or on 3.0 (22 Apr 2
domized to 1R following tmonstrated th
e subgroupweeks who a% when treatponders andtment group
ponders andks is require across all s24 weeks.
ABBVIE REse III trials a
hosis. Basedrated with a y of the AEBV. Howevebination wit
T) elevationsunction andcases were traceptives ocontinuatioelevation. T
erved in sube bilirubin taritaprevir aeatment, peubin elevatiodirect bilirub
ponse of CHtment-naīve
bitasvir with out RBV [61
se results frht provide p
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
12 or 24 wereatment fohat the smap of genotypachieved anted for 24 w
d relapsers hp, while simid relapsers ted only for csubgroups i
EGIMEN haacross a vard on Phase low disconts and laborer, these AEth interferons were obse
d generally rin women oor hormone
on or brief inTransient elbjects receivransportersand RBV-indeaked by stuons were nobin elevatio
HC genotype patients wvs. without
1]. No seriou
rom pivotal shysicians w
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
eeks of therar 12 or 24 w
all differencepe 1a treatmn SVR of 80
weeks. Amonhad higher Silar SVR rattreated for 2cirrhotic genn genotype
as been studriety of patieIII data, thetinuation ratratory abnorEs were mun. Transient,erved at a loresolved witon concurre replaceme
nterruption olevations in ving the ABBs, organic anduced hemoudy Week 1ot associatens was lowe
pe 4 was assere randomRBV for 12us SAEs or
studies are with the arma
vir and dasab
nfidential Informermitted witho
06.2015
apy. Overallweeks, respe in SVR be
ment-experie0%. This subng genotypeSVR rates ttes were see24 weeks, snotype 1a n 1b treatme
died with anent populatie ABBVIE Rte. Adverse rmalities repuch milder th, asymptomow rate, werth ongoing t
ent ethinyl esnt) and disc
of the ABBVserum biliruBVIE REGInion-transpoolysis. Biliru, and gener
ed with aminer among s
sessed in thmized to the
weeks. TheAEs leadin
encouraginamentarium
buvir
mation ut prior written
l 92% and 9ectively. An
etween treatenced prior bgroup of pae 1a infectehan null resen among tuggesting thull responde
ent-experien
nd without Rons includin
REGIMEN, wevents (AE
ported were han observe
matic serum re not assoctreatment. Astradiol-concontinuationVIE REGIMEubin (predomMEN with Rorting polypubin elevatiorally resolvenotransferasubjects who
he phase II 2 DAA come SVR was g to discont
ng and the nm to cure the
n authorization
96% of patienalysis of sutment arms null respondatients achid patients,
sponders in he null resphat the longers. SVR ra
nced patient
RBV in over ng those witwith or withoEs) were typ
attributableed when RBalanine amciated with A disproportntaining thern of the hormEN led to resminantly ind
RBV, relatedeptides (OAons occurreed with ongose elevationo did not rec
study PEARmbination of
100% with tinuation we
new interferoe vast major
from AbbVie Page
ents achieveubgroups was due larders treatedeved an SVpartial the 12 wee
ponders, pager durationates were vets treated fo
2,300 patieth compens
out RBV, wapically mild, e to the presBV was giveinotransferahepatic tionate numrapy (i.e., monal therasolution in sdirect) wered to the inhibATPs) 1B1/1d after initiaoing therapyns. The freqceive RBV.
RL-I in whicParitaprevirRBV vs. 91
ere reported
on-free regirity of patien
e 18 of 61
ed
rgely d for VR of
ek rtial of 24
ery or 12
ents in sated as well and sence en in ase
ber of
py serum bition 1B3, ation y. uency
h 86 r/r – %
d.
mens nts
Versio
infecthesthe fevertreat
7.2
The effecunde
The Russ
The the Aeveras aenviwhictrialspopupatiecondresetheremak
ThisREGRuss
Durithe tfollowstudlikelyvirolotreatfor th
No use or on 3.0 (22 Apr 2
cted with CHe results trafirst proteasryday life ant patient sub
ABBVIE REctive in rander well contr
ABBVIE REsian Federa
rationale foABBVIE REryday clinica measure oronment, su
ch a drug acs typically haulations in roents with heditions and cearch allowsefore be rele
kers [65].
observatioGIMEN ± RBsian Federa
ng the last dtreatment ofwing the disies with largy to respondogical cure.tment exposhe eradicati
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
HC. Howeveanslate into se inhibitors nd especiallybgroups tha
Rationa
EGIMEN ± Rdomized conrolled condi
EGIMEN is ation for the
or this obserEGIMEN as al settings, eof the capacuch as in a rchieves its inave limited outine clinic
eterogenouscould be uss for externaevant for he
nal study is BV, used acation in clinic
decade whef CHC, manscovery of pge data basd and futile . HCV genosure and onon of HCV
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
er, the mediroutine clinwhich werey the tolerab
an expected
ale
RBV for thentrolled clinitions.
expected totreatment o
rvational studemonstratevaluating itity of a treatrandomizedntended effeexclusion c
cal practice,s compliancsed to modeal patient-, pealth-care d
the first efccording to lcal practice
en dual thernagement ofpredictive fases [66]. Thutreatment s
otype and sun-treatment in everyday
vir and dasab
nfidential Informermitted witho
06.2015
ical commuical practice
e available tbility was fa from the de
e treatment oical trials wi
o be first IFNof CHC in 2
udy is to detted in pivotats effectiventment to pro
d controlled ect in the us
criteria and w treated pere patterns a
el and dissemprovider-, anecisions by
fectiveness ocal label, u patient pop
rapy with pef patients an
actors of virous treatmenstopped in pubtype, basevirological r
y clinical pra
buvir
mation ut prior written
nity is expee particularlto physicianar less favorevelopment
of CHC hasth strict incl
N-free comb015.
termine howal trials transness. Whereoduce the dtrial, effectivsual clinical will involve tr local labeland patientsminate bestnd system-le both provid
research exunder real wpulation.
egIFN plus Rnd clinical oological respnt could be tpatients witheline viral loresponse practice [27]. M
n authorization
cting data wy after the e
ns and wherrable in certat trials [62] [6
s been showlusion and e
bination ava
w the efficacslates into reas efficacyesired effecveness is ‘thsetting’ [64
the broader, which mig
s with signifit practices. evel factorsders in pract
xamining theworld condit
RBV was staoutcome weponse, oftentargeted to ph a low likelioad, fibrosisroved to be More recent
from AbbVie Page
which show experience wre the outcoain difficult-63].
wn to be safeexclusion cr
ailable in the
cy and safetreal world y can be defct in a controhe extent to
4]. Effectivenr patient ht include icant comorEffectivenes and can tice and pol
e ABBVIE tions in the
andard of cre improvedn in observapatients mohood of
s stage, ageuseful predtly the disco
e 19 of 61
how with me in
-to-
e and riteria
e
ty of
fined olled
o ness
rbid ss
licy-
are for d ational ost
e, ictors
overy
Versio
of a (SNPFor nresprespobseidennot dwith
The stagoutcadhephys
The repoREG
8.0
8.1
Wharesoin a
8.2
8.2
1
8.2
2. To
No use or on 3.0 (22 Apr 2
genetic dispP) contributnew interfer
ponse is extrponse were ervational sttify predictivdetected in the interfer
label of thee of liver dis
come in dailyerence on trsicians to im
aim of this orted outcomGIMEN ± RB
at is the effeource utilizatreal life sett
2.1
1. To descABBVIE
2.2
o provide re
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
position of ted further toron-free trearemely sparnot initially tudy may plve factors ointervention
ron-free ABB
e ABBVIE Rsease. It is ty clinical prareatment ou
mprove the m
observationme, work proBV in a real
Resea
Resear
ectiveness, ption of the inting across
Objecti
Prima
ribe in routi REGIMEN
Secon
eal world ev
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
the Interleuko our underatment regimrse and sevidentified thay an impo
of virologicalnal trials andBVIE REGIM
EGIMEN wtherefore reactice. In adutcomes in emanagemen
nal study is toductivity anworld settin
arch Que
rch Questi
patient reponterferon-freclinical prac
ives
ary Objecti
ne clinical p ± RBV in p
ndary Obje
idence for p
vir and dasab
nfidential Informermitted witho
06.2015
kin 28B (IL2rstanding of mens know
veral of the nhrough analyrtant part inl response id which couMEN in the
ill vary accoelevant to unddition, this everyday sent of patient
to provide end healthcang across cl
stion and
on
orted outcomee ABBVIE ctice patient
ive
practice the patients with
ectives
predictive fa
buvir
mation ut prior written
28B) single nvirological ledge of prenow well estyses of the bridging thn everyday
uld be used future.
ording to HCnderstand thstudy will p
ettings, whicts under the
evidence of are resourceinical practi
d Object
me, work proREGIMENt population
effectiveneh CHC as ev
actors of viro
n authorization
nucleotide presponses t
edictive facttablished prdevelopmee data gapsclinical settto further op
CV genotypehe pattern o
provide datach may helpeir care.
the effectivee utilization oice patient p
tives
oductivity a± RBV in pa
ns?
ss of the intvidenced by
ological resp
from AbbVie Page
polymorphisto treatmentors of viroloredictors of nt trials. Ths and could tings which ptimize trea
e/subtype aof use and on the imp
p treating
eness, patieof the ABBVpopulations.
nd healthcaatients with
terferon-freey SVR12
ponse
e 20 of 61
sm t [67].
ogical
is help were
atment
and
act of
ent VIE .
are CHC
e
Versio
3. Topopu4. To5. Toprod6. Toutiliz
9.0
9.1
Thisfree at thmadpatie
AdulREGclinic
Afterdatalabodocuwill bweeuniqonce
Thisprocobsedocu
Thistreat
No use or on 3.0 (22 Apr 2
o collect infoulation o describe to documentductivity in tho determinezation
is a prospeABBVIE REe discretione independ
ent the oppo
lt patients cGIMEN will bcal visit at th
r written infoa, HCV disearatory asse
umentation)be observedks after treaue patient n
e the investi
study is foccedures andervational stumented wil
12-week 24-week
schedule istment for CH
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
ormation on
the tolerabilt the effect ohe Russian e the impact
Resea
Study D
ective, multiEGIMEN witn of the physently from t
ortunity to p
hronically inbe offered thhe participa
ormed consase charactssments as
) will be docd for the duratment comnumber will igator or de
cusing on cod diagnostic tudy period ll be those c
k treatment k treatment
s based on HC.
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
n co-morbid
ity of the ABof the ABBVpopulation
t of the ABB
arch Meth
Design
-center obsth or withousician in accthis observaarticipate in
nfected withhe opportun
ating sites.
sent has beeteristics, co-s recorded incumented inration of thepletion. No be automatsignee crea
ollecting reamethods wentails the
closest to th
regimen: foregimen: fo
the anticipa
vir and dasab
nfidential Informermitted witho
06.2015
ities and co
BBVIE REGVIE REGIME
BVIE REGIM
hods
ervational sut RBV. Thecordance w
ational studyn this study.
h HCV, recenity to partic
en obtained-morbiditiesn the patien the electro
e ABBVIE Rpatient identically allocaates a new p
al-world datwill follow ph
following dahe time wind
our visits pluour visits plu
ated regular
buvir
mation ut prior written
oncomitant m
GIMEN ± RBEN ± RBV o
MEN ± RBV
study in patie prescriptiwith local cliny and prece
eiving the intcipate in this
, patient das, co-medicant's medical nic case rep
REGIMEN thntifiable infoated by the wpatient file.
a. Follow-upysicians’ roata collectiodows as ind
us two interimus three inte
r follow-up fo
n authorization
medication i
BV on PROs an
on healthca
ents receivion of a treatmnical practicdes the dec
terferon-frees study durin
ta includingation, treatmrecords (soport form (eherapy and formation willweb based
p visits, treautine clinica
on schemesicated in Fig
m data colleerim data co
or patients u
from AbbVie Page
in the Russi
nd work
are resourc
ing the interment regime
ce and labelcision to offe
e ABBVIE ng a routine
g demograpment details,ource eCRF). Patiefor up to 24l be captureeCRF syste
atment, al practice. T, data gure 1:
ection windoollection win
undergoing
e 21 of 61
ian
e
rferon-en is , is er the
e
hic , and
ents 4 ed, a em
The
ows dows
Versio
Figu
9.2
For o9.1 a
9.2
Patie
No use or on 3.0 (22 Apr 2
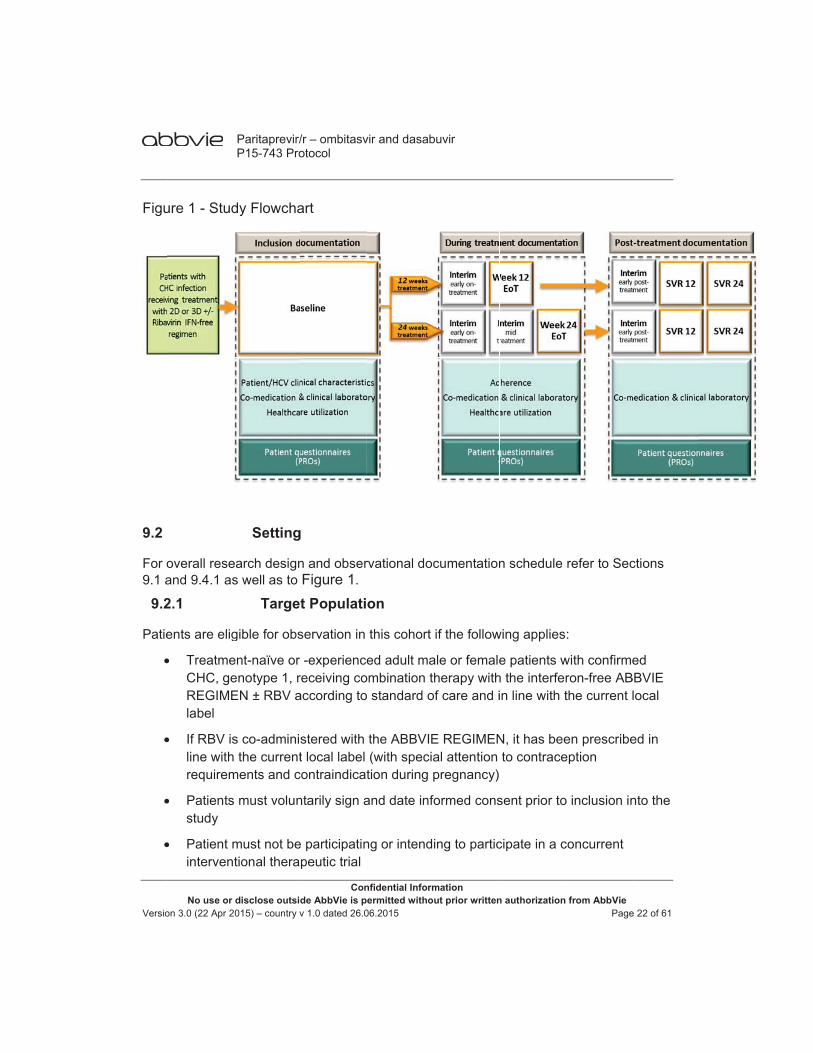
ure 1 - Stud
overall reseand 9.4.1 as
2.1
ents are elig
TreatmeCHC, geREGIMElabel
If RBV isline withrequirem
Patientsstudy
Patient minterven
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
dy Flowcha
Setting
earch designs well as to
Targe
gible for obs
ent-naïve or enotype 1, rEN ± RBV a
s co-admini the current
ments and c
s must volun
must not betional thera
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
art
g
n and obserFigure 1.
t Populati
servation in
-experiencereceiving coaccording to
stered with t local label
contraindicat
ntarily sign a
e participatinpeutic trial
vir and dasab
nfidential Informermitted witho
06.2015
rvational doc
on
this cohort
ed adult maombination to standard o
the ABBVIE(with speciation during p
and date inf
ng or intend
buvir
mation ut prior written
cumentation
if the follow
ale or femaleherapy with
of care and i
E REGIMENal attention pregnancy)
formed cons
ing to partic
n authorization
n schedule
wing applies
e patients wh the interferin line with t
N, it has beeto contrace
sent prior to
cipate in a c
from AbbVie Page
refer to Sec
:
with confirmeron-free ABthe current l
en prescribeeption
o inclusion in
concurrent
e 22 of 61
ctions
ed BBVIE local
ed in
nto the

Versio
9.2
Thismonwee
The maxpatie48 w
9.2
For pEoT be dthe eSect
If, inSVR
9.2
UnivmanAbbVrepreand instit
No use or on 3.0 (22 Apr 2
2.2
is a prospeths and theks post-trea
observationx. 36 weeks ents receivinweeks (24 w
2.3
patients wheCRF pageocumented
event must tion 11.5).
such patienR12 and SVR
2.4
versity centeagement ofVie Affiliate esentative otheir availatute will be d
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Study
ective, obsee observatioatment.
nal period fo(12 weeks tng 24 week
weeks treatm
Termi
o terminatee should be. If the reasbe reported
nts, there isR24 pages
Invest
ers and outpf patients wiMedical Dir
of the medicbility of the documented
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
y Duration
rvational stunal period o
or patients rtreatment as of ABBVIE
ment and 24
nation Cri
the ABBVIe filled in andson for ABBVd to AbbVie
s evidence oshould be c
tigator Sel
patient clinicith CHC willrector will ecal practice target patied in the eCR
vir and dasab
nfidential Informermitted witho
06.2015
udy. The incof the study
receiving 12and 24 weekE REGIMEN
4 weeks pos
iteria
E REGIMENd the reasonVIE REGIMwithin 24 ho
of virologicacompleted if
lection Cr
cs qualified l be selectensure that sin the coun
ent populatioRF.
buvir
mation ut prior written
clusion periwill be from
2 weeks of Aks post-treatN the observst-treatment
N prematuren for treatm
MEN discontours of phys
al response f respective
iteria
by training d to participsites participtry, have th
on. The type
n authorization
od will be am baseline v
ABBVIE REtment obsevational pert observatio
ely for whatent disconti
tinuation is dsician aware
during theradata is ava
and experiepate in this spating in thee ability to c
e of the part
from AbbVie Page
pproximatevisit until 24
GIMEN willrvation) andriod will be mn).
tever reasoninuation shodue to an Seness (see
apy or at Eoailable.
ence in the study. The e study are conduct theticipating tre
e 23 of 61
ly 8
be d for max.
n the ould AE,
oT, the
e study eating
Versio
9.3
9.3
9.3
• C
• S
• Qworkinitia
• P
9.4
Sourpatieare cmeddocu
The ethicdirec
9.4
Thison d
Afterthe erouti
No use or on 3.0 (22 Apr 2
3.1
The [i.e. ≥
3.2
Co-morbidit
Serious and
Questionnaik productivitation, at EoT
PAM-13, PS
rce documeent data in hcollected froical records
umentation
investigatorcs committect access to
4.1
observatioata to be co
r the patienteCRF, if avaine clinical p
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Variabl
Prima
percentage≥70 days] a
Secon
ies and con
d non-seriou
ires on PROty and activiT as well as
SP satisfacti
Data So
ents are defihis/her own om the sours containingand laborat
r(s)/institutioee/- review bo source dat
Data t
nal study coollected thro
t has signedailable frompractice.
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
es
ary Variabl
e of patientsafter the last
ndary Vari
ncomitant m
us adverse e
Os: EuroQolity impairme 12 and 24
ion and utili
ources
ined as origpatient files
rce documeg demographtory assessm
on(s) will peboard (IEC/ta documen
to be Docu
overs three oughout the
d informed c the patient
vir and dasab
nfidential Informermitted witho
06.2015
e
achieving St actual dos
ables
edication
events and
l 5 dimensioent (WPAI) weeks after
zation ques
ginal docums which will nts for eachhic data, mements.
ermit study-rIRB) review
nts.
umented
documenta study is su
consent, thet charts base
buvir
mation ut prior written
SVR12 (HCe of the AB
pregnancy
on 5 level (Equestionnair EoT
stionnaires
ents. The inserve as so
h patient in tedical, treat
related monw, and regula
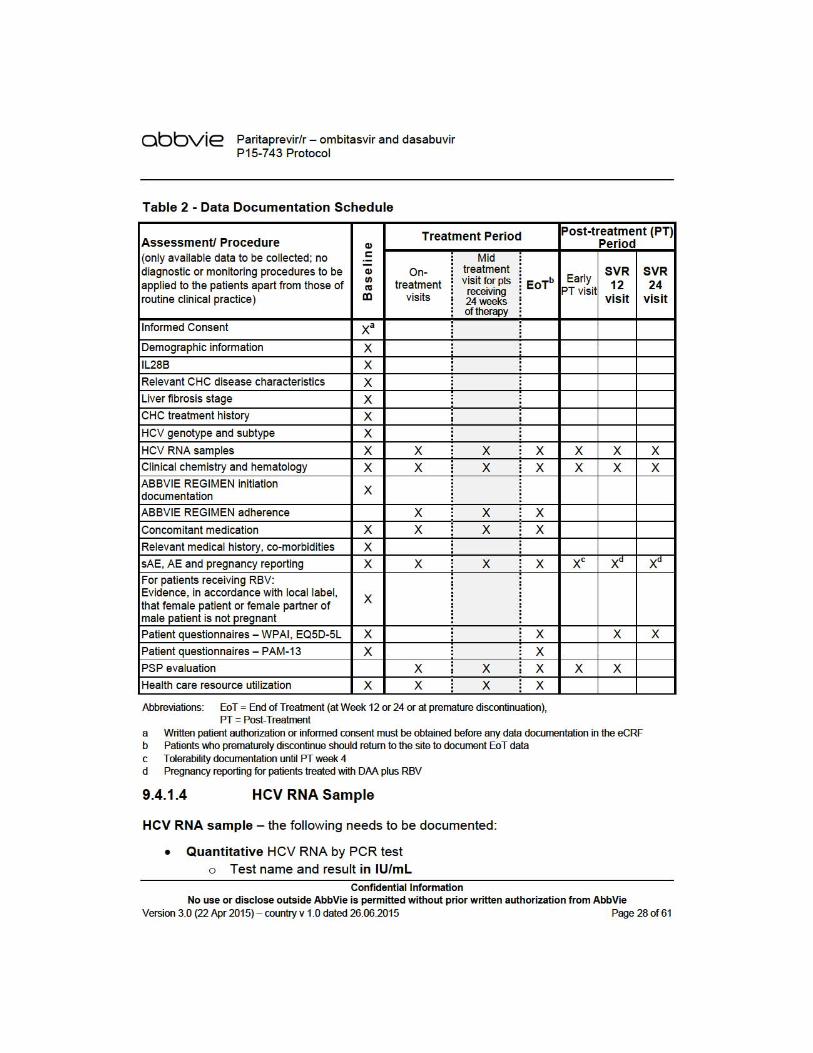
ation periodsmmarized i
e following ded on asses
n authorization
CV RNA <50BVIE REGI
occurrence
EQ-5D-5L) qire prior to t
nvestigator wource data fothe study, ctment and d
nitoring, audatory inspec
s, see Figurn Table 2.
data will be ssments do
from AbbVie Page
0 IU/mL 12 wMEN)
s
questionnaitreatment
will documeor the study
consisting ofdiagnostic
dits, indepenction(s), pro
re 1. An ove
documentene in physic
e 24 of 61
weeks
re and
ent y. Data f
ndent oviding
erview
ed in cians’
Versio
9.4.
The
No use or on 3.0 (22 Apr 2
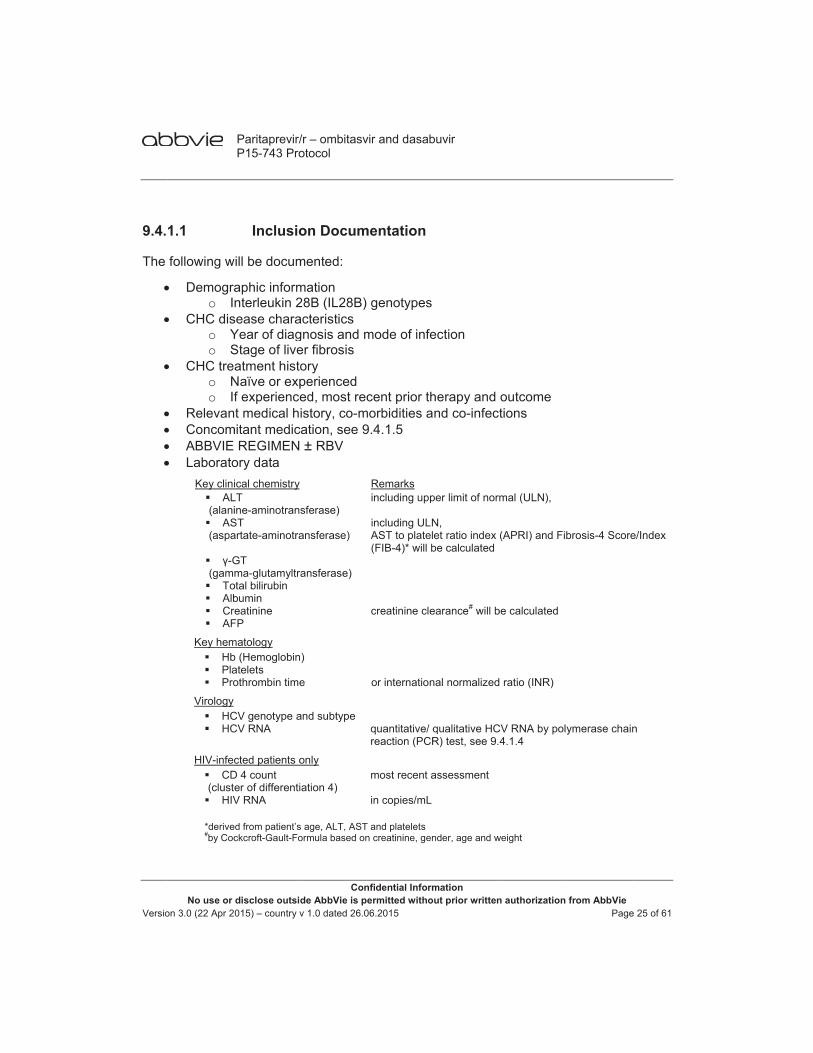
1.1
following w
Demograo I
CHC diso Yo S
CHC treo No If
Relevan Concom ABBVIE Laborato
Key clin AL(alani AS(aspa
γ-G(gam To Alb Cr AF
Key hem Hb Pla Pro
Virology HC HC
HIV-infe CD(clust HIV
*derive#by Coc
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Inclusio
will be docum
aphic informnterleukin 2
sease charaYear of diagStage of liveatment histo
Naïve or expf experience
nt medical hmitant medic
REGIMENory data ical chemistry
LT ine-aminotrans
ST artate-aminotra
GT ma-glutamyltra
otal bilirubin bumin reatinine FP
matology b (Hemoglobinatelets othrombin time
CV genotype aCV RNA
cted patients oD 4 count ter of differentiV RNA
ed from patient’sckcroft-Gault-Fo
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
on Docum
mented:
mation 28B (IL28B)acteristics gnosis and mer fibrosis ory perienced ed, most recistory, co-mation, see 9 ± RBV
sferase)
ansferase)
ansferase)
)
e
and subtype
only
ation 4)
s age, ALT, ASTormula based on
vir and dasab
nfidential Informermitted witho
06.2015
mentation
genotypes
mode of infe
cent prior thmorbidities a9.4.1.5
Remarks including upp
including ULNAST to platel(FIB-4)* will b
creatinine cle
or internation
quantitative/ qreaction (PCR
most recent a
in copies/mL
T and plateletsn creatinine, gen
buvir
mation ut prior written
ection
herapy and nd co-infect
per limit of norm
N, et ratio index be calculated
earance# will b
nal normalized
qualitative HCR) test, see 9.4
assessment
nder, age and w
n authorization
outcome tions
mal (ULN),
(APRI) and Fi
be calculated
ratio (INR)
CV RNA by pol4.1.4
weight
from AbbVie Page
brosis-4 Score
ymerase chain
e 25 of 61
e/Index
n
Versio
9.4.
Follotreatprac
The
9.4.
Follotreatprac
No use or on 3.0 (22 Apr 2
Patient q PAM-13 Treatme
1.2
ow-up visits tment, proce
ctice.
following w
LaboratoKey clin
AL AS
γ-G To Cr
Key hem Hb Pla
Virology HC
HIV-infe CD HIV
Concom Adheren
taken an Tolerabi Patient q PSP sat Treatme
1.3
ow-up visits tment, proce
ctice.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
questionnai
ent related h
During
are scheduedures and
will be docum
ory data ical chemistry
LT ST
GT otal bilirubin reatinine matology b atelets
CV RNA cted patients o
D 4 count V RNA
mitant medicnce to ABBVnd RBV Y/Nlity (sAEs aquestionnaitisfaction anent related h
Post-Tr
are scheduedures and
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
res, see tab
health care r
Treatmen
uled by the pdiagnostic
mented:
only
ation, see 9VIE REGIME
N) and AEs, seeres see 9.4
nd utilizationhealth care r
reatment D
uled by the pdiagnostic
vir and dasab
nfidential Informermitted witho
06.2015
ble 2 and 9.4
resource uti
nt Docume
physician pemethods wi
Remarks including ULNincluding ULNAPRI and FIB creatinine cle quantitative/ q most recent ain copies/mL
9.4.1.5 EN ± RBV (
e 11.5) and.1.6
n questionnaresource uti
Document
physician pemethods wi
buvir
mation ut prior written
4.1.6
ilization
entation
er routine cill follow phy
N N, B-4 will be calc
earance will be
qualitative HC
assessment
(ABBVIE RE
pregnancie
aires; PAM-ilization
tation
er routine cill follow phy
n authorization
linical practysicians’ rou
culated
e calculated
CV RNA PCR t
EGIMEN - %
es (see 11.6
-13
linical practysicians’ rou
from AbbVie Page
tice. Likewisutine clinica
test, see 9.4.1
% of target d
6)
tice. Likewisutine clinica
e 26 of 61
se al
.4
dose
se al
Versio
The
No use or on 3.0 (22 Apr 2
following w
LaboratoKey clin
AL AS
γ-G To Alb Cr
Key hem Hb Pla Pro
Virology HC
HIV-infe CD HIV
Tolerabi
Patient q PSP Sat
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
will be docum
ory data ical chemistry
LT ST
GT otal bilirubin bumin reatinine matology b atelets othrombin time
CV RNA
cted patients oD 4 count V RNA
lity (sAEs, s
questionnaitisfaction an
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
mented:
e
only
see 11.4) an
res see 9.4nd utilization
vir and dasab
nfidential Informermitted witho
06.2015
Remarks including ULNincluding ULNAPRI and FIB creatinine cle or INR quantitative/ q
most recent ain copies/mL
nd pregnanc
.1.6 n questionna
buvir
mation ut prior written
N N, B-4, will be cal
earance will be
qualitative HC
assessment
cies (see 11
aires
n authorization
lculated
e calculated
CV RNA PCR t
1.6)
from AbbVie Page
test, see 9.4.1
e 27 of 61
.4
Versio
9.4.
Con
It shadmmedpoterevievisit
9.4.
This5D-5adm
AsseThe statuusualevemapperc
The Anne
No use or on 3.0 (22 Apr 2
o L(
Qualitato To L
1.5
ncomitant m
Concomtreatmen
ould be verministered wi
ications maential for druew the concfor potentia
1.6
study will a5L and WPA
ministered.
essment of EQ-5D-5L i
us (utility). Tal activities, ls of severit
pped to a preception of th
EQ-5D-5L sex 1.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Lower limit o(LLoQ) in IU
tive HCV RTest name aLLoD in IU/m
Concom
medication
mitant medicnt with the A
rified by the ith the ABBV
ay be contraug-drug intercomitant meal DDIs.
Standa
assess qualAI Hep C. V
general quais a health s
The 5 items pain/discom
ty. Responseference (uteir overall h
should requ
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
of detectionU/mL
NA by PCRand result (pmL
mitant Med
- the follow
cation used fABBVIE RE
treating phyVIE REGIM
a-indicated, ractions (DD
edication(s)
rdized Ass
ity of life anValidated tra
ality of life -state utility iin the EQ-5
mfort, and ases to the 5 tility) specif
health on a s
uire approxim
vir and dasab
nfidential Informermitted witho
06.2015
(LLoD) in I
R test positive/n
dication
wing will be d
from the timGIMEN unt
ysician that MEN (includi
some may DIs). The inlabels and s
sessment
nd work prodnslations of
EQ-5D-5L instrument t5D-5L companxiety/depritems encod
fic for differeseparate vis
mately 5 mi
buvir
mation ut prior written
IU/mL and l
egative)
documented
me when theil after the la
concomitanng ritonavirrequire dosvestigator oscreen conc
t Tools
ductivity usif these patie
that evaluatprise 5 dimeression) eacde a discret
ent societiessual analog
nutes to co
n authorization
lower limit o
d:
e decision isast dose
nt medicatio) and RBV. e adjustme
or qualified dcomitant me
ng PRO insent question
tes preferenensions (moch of which te health stas. Patients aue scale (V
mplete and
from AbbVie Page
of quantifica
s made to in
on can be saSome nts due to designee shedications a
struments: Ennaires will
nce for healtbility, self-care rated onate which isalso rate the
VAS).
is presente
e 29 of 61
tion
nitiate
afely
hould at each
EQ-be
th are, n 5
s eir
ed in

Versio
AsseThe and quanWPAmodV2.0askeimpaimpaprod
The in An
PROparti(incldeteotheAbbV
Patie
PAMself-pres
Patie
The and
The pres
No use or on 3.0 (22 Apr 2
essment of wWPAI quesdaily activitntitative assAI has beenified for spe
0 is the HCVed about timaired in the airment fromductivity:
% Prese % Absen % Total
impairme % Total
impairme
WPAI Hep nnex 2.
O data are nicipating siteuding a sus
ermine wheter AbbVie auVie Pharma
ent Activatio
M 13 is a memanageme
sented in An
ent Support
PSP utilizapatient’s ov
PSP questisented in An
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
work produstionnaire wy impairmen
sessment ofn validated aecific healthV specific qume missed fr
past seven m 0 to 100, w
enteeism – pnteeism – pwork produent due to hactivity impent due to h
C should re
not consideres should respected advher the eveuthorized pracovigilance
on Measure
easure usedent. It shouldnnex 3.
t Program (P
tion and satverall satisfa
ionnaire shonnex 5-6.
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
ctivity and awill be used t
nt. The WPAf both reducas a genera condition, d
uestionnairerom work andays. Resu
with higher
percentage percentage o
ctivity impahealth problpairment (TAhealth probl
equire appro
red a potenteview the Pverse reactioent is relatedroduct) and e contact de
e – (PAM-13
d to assess d require ap
PSP) Quest
tisfaction asaction with t
ould require
vir and dasab
nfidential Informermitted witho
06.2015
activity impato measure AI question
ced productil health meadisease or pe that will bend time whilults of WPAIpercentage
of impairmeof work timeirment (TWem
AI) – percenem
oximately 5
tial source oRO data anon) is notedd to paritaprif so, it sho
etails are spe
3)
the patient pproximately
tionnaire
ssessment wtheir respec
e approxima
buvir
mation ut prior written
airment – Wwork absennaire was cvity at workasure (WPAproblem (We used in thile at work dI are expres
es indicating
ent while woe missed duP) – percen
ntage of gen
minutes to
of adverse rnd if a possib, the health
revir/r – ombuld be repoecified in Se
knowledge,y 7 minutes
will evaluatetive Patient
ately 2-5 min
n authorization
WPAI Hep C nteeism, wocreated as ak and non-wAI-GH) and
WPAI-SHP). Wis study). Ruring which
ssed as a peg greater imp
orking due tue to health ntage of ove
neral (non-w
complete a
eactions. Hble product-care provid
bitasvir ± darted to AbbVection 11.0.
, skill, and cto complete
e the frequeSupport Pr
nutes to com
from AbbVie Page
V2.0 ork presentea patient-repwork activitie
can be easWPAI Hep Cespondents
h productivitercentage opairment an
to health proproblem
erall work
work) activity
nd is prese
owever, -related eveder (HCP) masabuvir (or Vie. The rel
confidence fe and is
ency of utilizrogram.
mplete and
e 30 of 61
eeism, ported es. ily C s are y was
of nd less
oblem
y
nted
ent must r any evant
for
zation
is

Versio
9.5
In phratesG1aeffecof thErro
As opatieSVR158
Tabl
N
* exa
9.6
9.6
Dataelectdiagperfoinvesin thor deauto
A covaliddiscrbe c
No use or on 3.0 (22 Apr 2
hase III stus of at least treatment ctiveness ofhe SVR12 raor! Referenc
obvious froments the widR12 rate is a
patients sho
le 3 Widt
Number of patients
158 94
ct two-sided 9
6.1
a for this stronic datanostic meaormed in pstigator or d
he protocol wesignee will
omatically al
omprehensidate the drepancies n
completed.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Study S
udies investt 90% were
experiencf the ABBVates in the ce source n
m Table 3, dth of the 9at least 95%ould be enr
th of 95% C
SVR
95% confidenc
Data Ma
Electr
study will ba capture asures, labpatients witdesignee frowill be entel create a nelocated by t
ve data vadata. Automneed to be
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
Size
igating the observed,
ced patientsIE REGIMEcore populanot found.
if the SVR95% confide%, then 94 prolled during
Confidence
R12 rates
90% 95%
ce interval acco
anagemen
ronic Case
be recorded(EDC) sys
boratory asth CHC incom the sou
ered into theew patient fthe system.
alidation promated checsolved by t
vir and dasab
nfidential Informermitted witho
06.2015
interferon-feven in diffs). To des
EN ± RBV ination of thisfor the defin
R12 rate is ence intervapatients are g the inclusio
e Interval fo
Lower L84.288.4
ording Cloppe
nt
e Report F
d in Englisstem usingssessmentscluded in turce documee eCRF. Fofile in the eC
ogram utilizcks for dahe research
buvir
mation ut prior written
free ABBVIEficult-to-treascribe in rn patients w
s study shounition of the
at least 90al (CI) will n
sufficient foon period of
or SVR12
95% Conimit Upp
r-Pearson
Forms
h by each a web-ba, findings his cohort, ents into th
or each enroCRF and a u
zing front-enata consisteher in the e
n authorization
E REGIMENat CHC patieroutine clinwith CHC, auld be achiee core popul
0%, then wnot be wideror a width of 8 months.
nfidence Intper Limit 94.2 98.4
participatinased eCRand obserwill be tra
e eCRF. Oolled patienunique patie
nd checks ency will
eCRF before
from AbbVie Page
N ± RBV, Sents (e.g. ciical practic
a precise eseved (see Sation).
ith 158 evar than 10%
of 10%. The
terval* Width10.0%10.0%
ng center vF. Examinarvations roanscribed bnly data sp
nt, the invesent number
in the eCRbe impleme the modu
e 31 of 61
SVR12 irrhotic ce the stimate Section
aluable . If the refore,
h% %
via an ations, utinely by the ecified
stigator will be
RF will mented, ule can
Versio
Follotheirsite. necepersEDCcomand
Accepassinvessysteinves
Orig
9.6
AEs will bFor (INN
9.7
9.7
The Sectstartdisea
No use or on 3.0 (22 Apr 2
ow-up on er representa
The investessary datason performC system. Tpleteness adate to the
ess to the sword-protestigator siteem will be stigator as a
inal Questio
6.2
will be codbe tabulatedtreatments,
N) Drug Term
7.1
target poption 9.2.1. Tted the treaase charac
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
eCRF data fatives). Quetigator or an correctionsing the corr
The principaand accuraceCRFs as e
EDC systeected methoes at the enarchived ona durable re
onnaires wil
Assig
ded using thd by primary surgical anms and Proc
Data An
AnalyMissin
ulation (TPThe core poatment com
cteristics. Pa
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
for medicaleries will be n authorizes to the eCrections, wilal investigacy of availabevidence th
em will be od of internd of the sin appropriatecord of the
ll be sent fro
nment of
he Medical y MedDRA nd medical cedures Dic
nalysis
sis Populang Data
) is definedopulation (Cmbination ratients not
vir and dasab
nfidential Informermitted witho
06.2015
plausibility generatedd member RF. All chal be availab
ator of eachble data andereof.
provided fonet accessite's participte data med site's eCRF
om the parti
Preferred
Dictionary fsystem orgaprocedures
ctionary will
ation, Tim
d as all patCP) is definrecommendreceiving th
buvir
mation ut prior written
y will be doin the eCRof the inves
ange informable via the ah site will fd provide h
or the duras. Such accpation in thedia (e.g. CDF data.
icipating site
Terms
for Regulatan class (SOs the internabe used.
me Window
tients who fned as all ped in the he treatmen
n authorization
one by AbbVRF for onlinestigator's station, includ
audit trail, wfinally revieis or her ele
ation of the cess will be study. DaD-ROM) an
e to:
ory ActivitieOC) and preational non-
ws and Han
fulfill the crpatients of tcurrent loc
nt recomme
from AbbVie Page
Vie personne resolutiontaff will makding the da
which is partw the eCRectronic sig
study throbe removedata from thend provided
es (MedDRAeferred term-proprietary
ndling of
riteria specihe TP, who
cal label foended in the
e 32 of 61
nel (or at the ke any te and t of the
RFs for gnature
ough a d from e EDC to the
A) and m (PT). y name
ified in o have
or their e local
Versio
labepopuone
(
(
(
The the A
In ameameaassigtreatanal
No dof thpostregafor tha poor uprecundepatie
No use or on 3.0 (22 Apr 2
l will be sulation with of the follow
(1) evaluabREGIME
(2) a HCV virologictreatmen
(3) HCV RNmeasureto reasoinformatand valupatients measurereasons willing toexcluded
Safety PopABBVIE RE
accordanceasurements asurements gned to aptment visits)ysis plan (S
data will be he HCV RNt-baseline, ardless of thhe flanking
ost-baseline nquantifiab
ceding and etectable orent has an
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
summarizedsufficient fo
wing criteria
le HCV RNEN (i.e. data
RNA valuecal responsnt)
NA <50 IU/mement ≥70 ons related tion (e.g. virue of the cwho had v
ement, but not relatedo perform ad from this a
pulation (SPEGIMEN.
e with thewill be perfohave to be ppropriate ). The time
SAP).
imputed foNA endpoint
but prior the value chimputation visit prior t
le, but detesucceedin
r unquantifiaunquantifia
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
d in the noollow-up daa:
NA data ≥7a within the
e ≥50 IU/mse achieved
mL at the ladays after tto safety (e
rologic failurcorrespondiirological rehad no HCV
d to safety oan additionaanalysis.
P) is defined
non-intervormed at thentered inttime pointswindows fo
r any effectts. When thto EoT, thosen for thdescribed bo EoT but hectable HCVg measureable, respeable HCV R
vir and dasab
nfidential Informermitted witho
06.2015
on-core pota (CPSFU
0 days afteSVR12 time
L at the lad at the las
ast measurthe last actue.g. droppedre such as ring HCV Response at tV RNA meaor effectivenal HCV RNA
d as all pati
ventional nhe sole discrto the eCRFs (baselineor the assign
tiveness or here is no He closest e subseque
below. If a phas undetecV RNA leve
ements, thectively, at t
RNA level a
buvir
mation ut prior written
opulation (N) is defined
er the last e window)
ast measurest measure
rement postual dose ofd out due torelapse is re
RNA test is their last onasurementsness (e.g. loA test ≥70
ients who re
nature of retion of theF. All record, on-treatmnments will
safety analHCV RNA values befent and prepatient has actable HCV els (with LLe HCV RNthis visit for at the prec
n authorization
NCP). In aas all CP p
actual dos
ement postement on-tr
t-baseline, f the ABBVIo AE) or ineported in th
missing). n-treatment s ≥70 days post-to-followdays post-
eceived at
the study e physician ded HCV R
ment visits, be specifie
yses excepvalue in a fore and aeceding winda missing HRNA (with
LoQ ≤50 IUNA level wir this patienceding meas
from AbbVie Page
ddition, thepatients, wh
e of the A
t-baseline (reatment or
but no HCVIE REGIMEcomplete ehe eCRF buThis meanor post-trea
post-treatmw-up or patie
treatment) w
least one d
all HCV and all HCV
RNA values EoT visit,
ed in the sta
pt for the anvisit time w
after the wdow, will be
HCV RNA vaLLoD ≤50
U/mL) at boill be cons
nt. In additiosurement a
e 33 of 61
e core ho fulfil
BBVIE
i.e. no r post-
V RNA EN due efficacy ut date s only atment ent for ent not will be
dose of
RNA V RNA will be post-
atistical
alyses window
window, e used alue at IU/mL) oth the sidered on, if a and an

Versio
undeRNArespmeaassuFor Sbe uremafailu
9.7
All bCP expeREGbe rstatiscontof pdetatakinvario
9.7
The in thstudFor tIU/m
No use or on 3.0 (22 Apr 2
etectable HA level will ponse at Eoans if HCV umed for EoSVR12 the used. Subseains missingre at this tim
7.2
baseline andanalysis g
erienced or GIMEN ± RBrepeated fostics (n, metinuous variaatients will
ails of analyng into accoous patient g
7.3
primary effe CP stratify several dthe purpose
mL,
• if a PCR
• and thetest res
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
CV RNA lebe imputed
oT a corresRNA is m
oT, if the susingle last aequent to thg at a spec
me point (i.e
Demo
d disease croups (i.e. naīve), whi
BV) and duror the SP ean, mediaables (e.g. abe presen
sis populatiount the ABgroups.
Effect
fectiveness fied by the Cifferent mete of the sta
R test was u
e test result ult is unqua
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
evel at the sd as unquansponding bamissing at ucceeding Havailable HChis flankingcific time poe. not undete
ographics a
characteristibased on
ich are relevration (12 aand the TP
an, standardage and boted for cateions and thBBVIE REG
tiveness A
analysis onCP analysis thods for de
atistical anal
used
is undetecantifiable an
vir and dasab
nfidential Informermitted witho
06.2015
succeedingntifiable at ackward imEoT, then HCV RNA vCV RNA me and backw
oint, then thectable or u
and Disea
ics will be s genotype vant for sch
and 24 weekP without sd deviation ody mass indegorical vare CP analy
GIMEN reco
Analysis
n clinical outgroups. Du
eterminationlysis, a HCV
table and thd the LLoQ
buvir
mation ut prior written
measuremthis visit foputation apunquantifiavalue is uneasurementward imputae patients w
unquantifiab
ase Charac
summarized1 subtype
heduled treaks). In additstratification[SD], and dex [BMI]).riables (e.g
ysis groups ommended
tcomes will ue to the nonn of the HCVV RNA mea
he LLoD of is ≤50 IU/m
n authorization
ment, or vicer this patie
pproach willable or unddetectable t ≥70 days pation, if the will conside
ble).
cteristics
d for the CPe, fibrosis atment comtion, baselinn into subgrange) will The numbe
g. gender awill be spein the curre
be performn-interventioV RNA valuasurement i
f the test is mL
from AbbVie Page
e versa, thent. For viro be applied
detectable wor unquant
post-treatme HCV RNA
ered as viro
P stratified status, trea
mbination (Ane summarigroups. Sumbe generat
er and percend race). Fcified in theent local la
med on all paonal nature
ue can be ais considere
≤50 IU/mL
e 34 of 61
e HCV ological d. This will be tifiable. ent will
A value ological
by the atment BBVIE ies will mmary ted for entage Further e SAP, bel for
atients of this
pplied. ed ≤50
or the
Versio
9.7.3
The [i.e. effec
9.7.3
The
9.7.3
The sidedClop
Corrrelapanal
No use or on 3.0 (22 Apr 2
3.1
percentageat least 70
ctiveness en
3.2
secondary
The EoT
The EoT
The docutreat
The SVR
o
o
o
o
3.3
simple percd 95% con
pper-Pearso
responding pse rate, virysis group
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Primary
e of patientsdays] after
ndpoint.
Second
effectivenes
percentage
percentagefollowed bypercentage
umented HCtment). number and
R12 non-reso On-treat
failure toIU/mL])
o Relapsetreatmenpost-trea
o Prematufailure
o Missing
Statisti
centage of pnfidence inteon method.
methods wral breakthros with EoT
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
y Effective
s achieving the last ac
dary Effect
ss endpoint
e of patients
e of patientsy HCV RNAe of patienCV RNA <5
d percentagponse categtment viroloo suppress
e (defined ant HCV RNAatment) ure study d
SVR12 data
cal Metho
patients acherval (CI) o
will be useough). The T response
vir and dasab
nfidential Informermitted witho
06.2015
eness End
SVR12 (sintual dose o
tiveness E
ts are:
s with virolog
s with relapA ≥50 IU/mLnts with br50 IU/mL fo
ge of patientgories: ogic failure [each meas
as HCV RNA measure
rug discont
a and/or no
ods for Ana
hieving SVRof the perce
ed for otherrelapse rate
e and suffi
buvir
mation ut prior written
dpoint
ngle last HCof the ABBV
Endpoints
gical respon
pse (defined) reakthrough
ollowed by H
ts meeting e
(breakthrosured on-tre
A <50 IU/mment follow
tinuation wi
ne of the ab
alysis of E
R12 will be entage will
r response es will be escient HCV
n authorization
CV RNA <50VIE REGIME
nse (HCV R
d as HCV R
h (defined HCV RNA ≥
each and an
ugh [defineeatment HC
mL at EoTwed by HCV
ith no on-tr
bove criteria
Effectivene
calculated abe comput
rates (Eostimated in p
RNA mea
from AbbVie Page
0 IU/mL 12 EN) is the p
RNA <50 IU/
RNA <50 IU
as at leas≥50 IU/mL
ny of the fo
ed as abovCV RNA valu
or at the laV RNA ≥50
reatment vi
a
ess Variab
and an exacted based o
T responsepatients of tasurements
e 35 of 61
weeks primary
/mL) at
/mL at
st one during
llowing
ve ] or ue ≥50
ast on-IU/mL
rologic
bles
ct two-on the
e rate, the CP post-

Versio
treatgrouleast
Univimpa
Furth
Thesperfoin eavarioeachMLR<0.2usedregreSVR
No use or on 3.0 (22 Apr 2
tment. Viralups, who hat one on-tre
variate and act of the fo
Key dem Mode of HCV RN Most rec HCV gen Type of Liver and Key clini In treatm
o Mo O
her details a
se analyseormed for vach patientous patient gh MLR analR models w25 in the cord for the coession meth
R12.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
l breakthrouve at least o
eatment or E
multiple logllowing exp
mographic inf CHC infectNA level at bcent stage onotype and treating instd/or CHC reical chemist
ment experieMost recent Outcome of
and addition
s will be various CP At group. Fugroups has ysis. Backw
which considrrespondingovariates tohods will als
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
ugh rates wone undetecEoT measur
gistic regreslanatory cov
nformation tion baseline of liver fibrossubtype (if titute elated co-mtry and hemenced patieprior treatmmost recen
nal covariate
of exploratAnalysis Grrthermore, to be taken
ward selectider only covg univariate o stay in thso be used t
vir and dasab
nfidential Informermitted witho
06.2015
will be estimctable HCVrement there
ssion (MLR)variates on
sis available)
orbidities matology lab
nts only: ment for CHnt prior CHC
es will be sp
tory natureroups, sincethe fact th
n into accouon proceduvariates in logistic regr
he model into investiga
buvir
mation ut prior written
mated in all V RNA meas
eafter.
methods wSVR12:
boratory vari
C C treatment
pecified in th
, data drive not each cat treatmennt, when se
ures will be the selectioression anan a backwaate the impa
n authorization
patients ofsurement on
will be used
iables at ba
he SAP.
ven, and wcovariate mnt regimenselecting the applied to
on procedualysis. A p-vard eliminatct of treatm
from AbbVie Page
f the CP ann-treatment
to investiga
seline
will be repemight be pres will differ patient grougenerate thre with a p
value <0.05 tion step. L
ment adheren
e 36 of 61
nalysis and at
ate the
eatedly edictive
in the ups for he final p-value will be
Logistic nce on
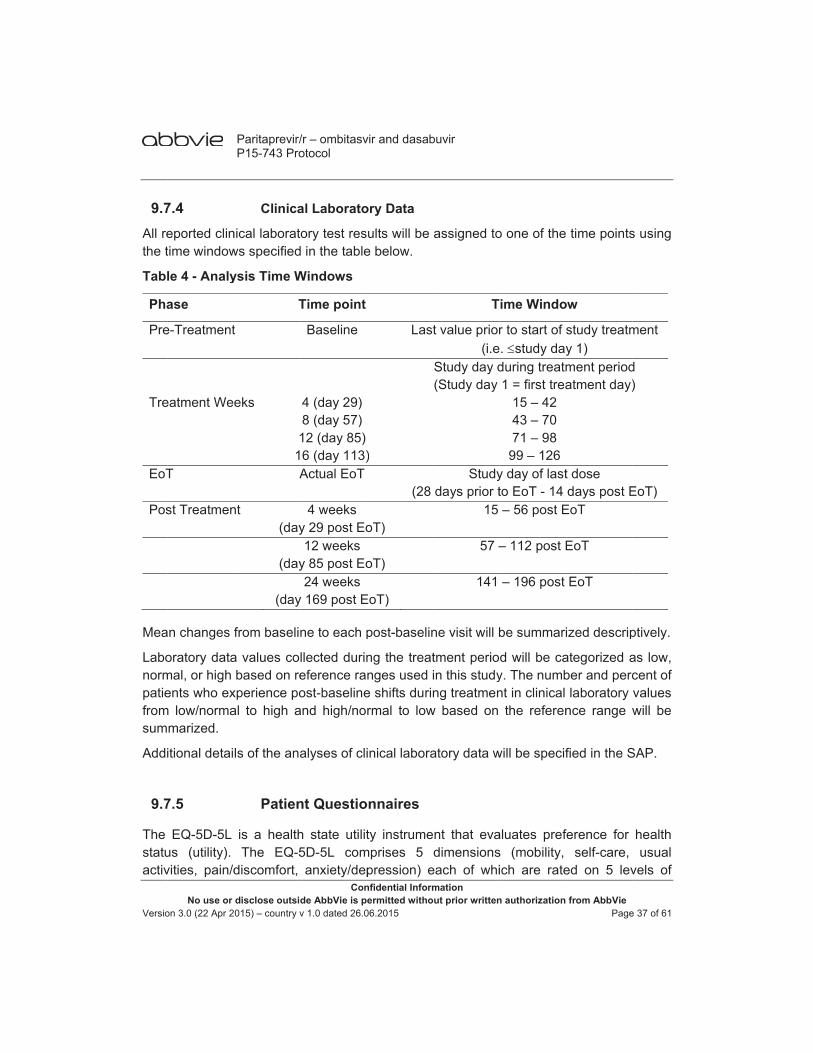
Versio
9.7All rethe t
Tabl
Pha
Pre
Tre EoT
Pos
Mea
Labonormpatiefromsum
Addi
9.7
The statuactiv
No use or on 3.0 (22 Apr 2
7.4 eported clintime window
le 4 - Analy
ase
e-Treatment
eatment We
T
st Treatmen
an changes
oratory datamal, or high ents who ex
m low/normamarized.
itional detai
7.5
EQ-5D-5L us (utility). vities, pain/d
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Clinica
nical laboratws specified
ysis Time W
T
t
eks
11A
nt (day
(day
(day
from baselin
a values cobased on re
xperience poal to high a
ls of the ana
Patien
is a healthThe EQ-5
discomfort,
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
al Laborato
ory test resd in the table
Windows
Time point
Baseline
4 (day 29)8 (day 57)12 (day 85)6 (day 113)Actual EoT
4 weeks y 29 post Eo12 weeks
y 85 post Eo24 weeks
y 169 post E
ne to each p
llected durineference raost-baseline
and high/no
alyses of cli
nt Questio
h state utilit5D-5L comanxiety/dep
vir and dasab
nfidential Informermitted witho
06.2015
ory Data
ults will be e below.
Last
)
(28
oT)
oT)
EoT)
post-baselin
ng the treatnges used ie shifts durinrmal to low
inical labora
onnaires
ty instrumemprises 5 pression) e
buvir
mation ut prior written
assigned to
T
t value prior(i.e
Study day d(Study day
Studydays prior t
15
57 –
141
ne visit will b
tment perioin this studyng treatmen
w based on
atory data w
nt that evadimensions
each of whi
n authorization
o one of the
ime Windo
r to start of s. study dayduring treatm1 = first trea
15 – 42 43 – 70 71 – 98
99 – 126y day of lastto EoT - 14 – 56 post E
– 112 post E
– 196 post
be summari
d will be cay. The numbnt in clinical
the referen
will be specif
aluates prefs (mobility, ich are rate
from AbbVie Page
time points
ow
study treatmy 1) ment periodatment day)
t dose days post E
EoT
EoT
EoT
ized descrip
ategorized aber and perclaboratory
nce range w
fied in the S
ference for self-care,
ed on 5 lev
e 37 of 61
s using
ment
d )
EoT)
ptively.
as low, cent of values will be
SAP.
health usual
vels of

Versio
seveprobVAS
Patie5-digseveheal(if no
No iscor
A sumaxbaseand inves5D-5
AsseC v2four from
1234
The
QQQQQQ
The
12
No use or on 3.0 (22 Apr 2
erity (1: indblems, 4: indS.
ents’ respongit code wierity. Theseth utility indot available)
mputation wre will be ca
ummary tabximum) of theline time pfor the VASstigate the 5L endpoint
essments of2.0 will be etypes of sc
m 0 to 100. H
1. % absen2. % prese3. % TWP:4. % TAI: p
WPAI Hep
Q1. currentlQ2. hours mQ3. hours mQ4. hours aQ5. degree Q6. degree
four scores
1. % absen2. % prese
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
icating no pdicating sev
nses to the ith one dige EQ-5D-5Ldex score by).
will be perfolculated.
ble will showhe index scpoints, as wS values. Ineffect of thes using the
f work prodevaluated acores, the reHigher perce
nteeism: peenteeism: pe
percentagepercentage
C v2.0 cons
y employedmissed due tmissed due tctually workhepatitis C hepatitis C
s will be deri
nteeism: 1enteeism: 1
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
problem, 2:vere problem
EQ-5D-5L it from eac
L states wily applying c
ormed for m
w descriptivore values
well as chann addition ae different Acorrespond
uctivity andaccording toesults of whentages ind
rcentage of ercentage oe of overall of general (
sists of 6 qu
d (yes, no) to hepatitis to other reaked in the laaffected proaffected reg
ived as follo
100*Q2/(Q2100*Q5/10
vir and dasab
nfidential Informermitted witho
06.2015
indicating ms, 5: indica
will be comch of the 5ll be convecountry-spe
issing items
ve statisticsand for the
nges from banalysis of cABBVIE REding EQ-5D-
d activity impo the WPAI-hich will be icate greate
f work time mof impairmen
work impair(non-work) a
uestions aim
C in the lassons in the
ast seven daoductivity wgular activit
ows:
2+Q4)
buvir
mation ut prior written
slight problating extrem
mbined into a5 dimensionerted into acific weight
s, and in ca
s (n, mean,e VAS valuebaseline botcovariance (EGIMENS (±-5L baseline
pairment as-SHP scorinpresented a
er impairme
missed duent while worrment due toactivity impa
med at the fo
st seven daylast seven
ays while working
ies
n authorization
lems, 3: indme problems
a unique hens represena single pres (if availab
ase of missin
, median, Ses for baselth for the in(ANCOVA) ± RBV and e values as
s assessed ng manual. as percentant:
to hepatitisrking due to o hepatitis Cairment due
ollowing targ
ys days
g
from AbbVie Page
dicating mos), and a se
ealth state unting the leeference-weble) or US w
ng items no
SD, minimuline and the
ndex score will be appduration) ocovariates.
by the WPAThe WPAI
age of impa
s C hepatitis C
C e to hepatitis
gets:
e 38 of 61
oderate eparate
using a evel of eighted weights
o index
m and e post-values
plied to on EQ-
AI Hep yields
airment
s C

Versio
34
A sccalcu
The unemanal
9.7
The contdescsumover(MLRPSPtreatSect
The patiebe a(1), “
Baseraw indicscorthe presp
In careplabe c
A sumaxas cinves
No use or on 3.0 (22 Apr 2
3. % TWP:4. % TAI:
core will be ulation of th
summary tmployed paysis will be
7.6
contributiontinuation ovecriptive and marize all cr time stratifR) analysis
P and the patment comption 9.7.3.3.
Patient Actent knowledanswered wi“disagree” (
ed on resposcores (ran
cating strengre can be aspatient is likponsibility fo
ase of missiacement. Ho
calculated.
ummary tablximum) for thhanges fromstigate the e
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
11
set to misshe score are
table will pratients and d
specified in
PSP a
n of the patier time, patiexploratory
correspondinfied by ABBVwill be perfo
atient satisfapletion. Thes. Additional
ivation Meadge, skill, anith one of fo(2), “agree”
onses to thege of the sugth of agreessigned to okely to particor his or her
ng item valuowever, if th
le will show he summarym baseline. effect of the
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
100*{Q2/(Q2100*Q6/10
sing if one oe missing. N
resent the adescriptive
n the SAP.
and PAM
ent supportient satisfacy statistical mng variablesVIE REGIMormed to invaction variabse MLRs widetails will
asure (PAM)nd confidencour possible(3), “agree
e 13-item meum: 13 – 52ement with tone of the focipate more health.
ues, the mehere are les
descriptivey score at bIn addition
e different A
vir and dasab
nfidential Informermitted witho
06.2015
2+Q4) + [Q4
or more of thNo imputatio
absolute anstatistics fo
t program (Pction and PSmethods. As of the PSP
MEN arms. Investigate thbles of the Pll be performbe specified
) 13 item scce for self-m response ostrongly” (4
easure, the 2) and mappthe 13 itemsour levels of
actively in
ean value ofss than nine
e statistics (nbaseline and
analysis of ABBVIE REG
buvir
mation ut prior written
4/(Q2+Q4)]
he items Qon will be pe
d relative fror the four s
PSP) to diseSP utilizatioppropriate fP questionnn addition, m
he associatioPSP questiomed similar d in the SAP
cale is a memanagemenoptions, whi4).
score is caping up the vs (100 *(sumf activation. health care
f the availabe items answ
n, mean, med the post-bcovariance
GIMENS (±
n authorization
* Q5/10}
1-Q6 that aerformed for
requencies scores. Furt
ease controon will be anfrequency taaire (see ANmultiple logon betweenonnaire withto the MLR
P.
asure used nt. Each of thch are “disa
lculated by value onto am - 13) / (52A higher scprocesses
ble items wiwered, no su
edian, SD, maseline time(ANCOVA)RBV and d
from AbbVie Page
are needed r missing ite
of employether details
l, treatmentnalyzed usinables will NNEX 4 andistic regress the use of
h the probabRs for SVR1
to assess the 13 itemsagree strong
adding up ta scale of 0–2 - 13)).The core indicateand takes m
ll be used foummary sco
minimum ane points, as ) will be appuration) on
e 39 of 61
for the ems.
ed and of the
t ng
d 5) sion the
bility of 2 (see
the s can gly”
the –100 final
es that more
or ore will
nd well
plied to the
Versio
sumbe s
9.7
All toSP s
All SincluThe evenpostCorrThe relatgivefor thPatiefor th
Addi
9.7
Not a
9.8
The and Sect
A covaliddiscrbe cpers
No use or on 3.0 (22 Apr 2
mary score pecified in t
7.7
olerability vstratified by
SAEs, non-suded in the
number annt that begit-study druresponding tabulation
tionship to sn MedDRA he severity ents reportihat SOC.
itional detai
7.8
applicable f
sites will bthe require
tion 9.4).
omprehensidate the drepancies ncompleted. sonnel (or t
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
using the cthe SAP.
Tolera
variables wiltype of com
serious AEsstudy (see
nd percentagns or worsg dosing) summary taof the num
study drug wPT will be csummary t
ng more th
ls of the ana
Interim
for this study
Quality
be instructedement to m
ve data vadata. Automneed to be Follow-up otheir repres
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
correspondin
ability Ana
ll be summmbination tre
s and prege Section 11ge of patienens in seve
will be tables will be
mber of patiewill also be pcounted ontable and than one type
alysis of AE
m Assessm
y.
y Control
d in the proaintain sou
alidation promated checsolved by ton eCRF dasentatives).
vir and dasab
nfidential Informermitted witho
06.2015
ng baseline
alysis
arized usineatment and
nancy occu1.0 and 9.2nts with treaerity after intabulated be provided ents with trprovided. Ply once for t
he most relae of event w
Es will be sp
ments
otocol, the furce docume
ogram utilizcks for dahe researchata for medThe princip
buvir
mation ut prior written
e value as co
g descriptivd scheduled
urrences are2.3). AEs watment-emenitiation of by primaryfor all serioeatment-ematients repothat term usated for thewithin a SO
pecified in th
functionalityents for ea
zing front-enata consisteher in the edical plausibpal investig
n authorization
ovariates. F
ve statisticad treatment
e to be repill be coded
ergent AEs study drug
y MedDRA ous treatmemergent AEsorting more sing the mo
e relationshiOC will be c
he SAP.
y and handach patient
nd checks ency will
eCRF beforebility will begator of eac
from AbbVie Page
Further deta
al methods fduration.
ported for pad using Me(i.e. any rethrough 30SOC and
nt-emergens by severithan one A
ost severe inp summary
counted only
ling of the in the stud
in the eCRbe impleme the modu
e done by Ach site will
e 40 of 61
ails will
for the
atients dDRA.
eported 0 days d PT.
nt AEs. ty and E for a ncident y table. y once
eCRF, y (see
RF will mented, ule can AbbVie
finally
Versio
revieher e
ContAbbV
9.9
The randmissmeafollowsear
The followas cdiagstud“homset. LLoDcont
10.0
ThisNotifand/regu
The prior
To mbe cprotestud
No use or on 3.0 (22 Apr 2
ew the eCRelectronic s
tinuous moVie or a CR
limitations domization, sing data aasurements,w-up and brches for mi
most imporw-up HCV R
compared tonostic testsy each cen
me-brew” teThe challenD and the Ltrolled trials
0
observatiofication/sub/or Competulations.
investigator to patient i
maintain patcollected (e.ect patient y recording
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
RFs for comignature an
nitoring of tRO working o
Limitat
of observaand difficu
are well kn document
by activities ssing key d
rtant outcomRNA data co the SVR s are requireter will be usts – which
nge is to accLoQ to put with (usual
Protec
onal study mission to tent Author
or is responsnclusion
tient confideg. initials, didentity, a .
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
mpleteness d date to eC
the study anon behalf of
ions of the
ational studulties to cleown. Their ation of theto obtain c
ata.
me measurean in particrate of inte
ed to measusing its owh might chacurately andthe results ly) central la
ction of H
will be runthe responsrities (CAs
sible to ens
entiality, nodate of birthunique num
vir and dasab
nfidential Informermitted witho
06.2015
and accuraCRFs as ev
nd frequent f AbbVie.
e Researc
ies, such aearly interprr validity cae most comcomplete re
e in this stuular lead to erventionalsure HCV Rwn test – eitnge from ond consisteninto perspecaboratory as
Human S
n in complisible regula) will be d
sure that wr
demograph) - only the
mber will be
buvir
mation ut prior written
acy of availaidence ther
site teleph
ch Methods
as uncontroret treatmean be incremmon confoecording of
udy is HCV an underestrials. High
RNA levels ither commene visit to ttly documenctive of priossessments
Subjects
iance with atory authordone as re
ritten inform
hic data thapatient age
e assigned
n authorization
able data aeof.
one contact
s
olled confouent effects eased by aounders, suavailable d
RNA. Missistimation of hly sensitivein blood. Inercially avaihe next witnt test prop
or outcomess for all trial
local laws rities, Ethicsequired by
med consen
at can idente will be col
to each pa
from AbbVie Page
and provide
ts will be do
unding by lin the cont
accurate ouufficient lenata as well
ing or unrecthe real SV
e and quan an observilable or so-hin a patienerties such
s from randoparticipants
and regulas Committeey local law
nt will be ob
tify the patielected. In oatient and r
e 41 of 61
his or
one by
ack of text of
utcome ngth of as by
corded VR rate titative ational -called nt data as the
omized s.
ations. e (EC)
ws and
btained
ent will rder to related
Versio
11.0
PROparti(inclevenprod
Medadmshou The
11.1
An adoesbe asymor no
Suchfromof a
No use or on 3.0 (22 Apr 2
0
O data areicipating situding a susnt is relatedduct) and if s
ication erroministration ould be repor
relevant Ab
1
adverse eves not necesany unfavoptom, or disot the event
h an event m accidental
pre-existing
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
ManagEvents
e not conses should rspected advd to the Aso, it should
ors (this refeof a medicinrted by the H
bbVie Pharm
AdversCatego
ent (AE) is dsarily have rable and sease tempt is consider
can result or intention
g condition o
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
gement as/Advers
idered a preview the verse reacti
ABBVIE REd be reporte
ers to any unal product HCP to Abb
macovigilanc
se Event Dories
defined as aa causal reunintended
porally assocred causally
from use onal overdosor illness is
vir and dasab
nfidential Informermitted witho
06.2015
and Repose Reacti
potential soPRO data on) is notedGIMEN ±
ed to AbbVie
unintentionawhile in co
bVie.
ce contact d
Definition a
any untowarelationship w sign (incluciated with y related to
of the drug se, drug abuconsidered
buvir
mation ut prior written
orting of ions
ource of adand if a pod, the HCP RBV (or ae.
al error in thontrol of the
details are s
and Seriou
d medical owith their treuding an athe use of athe use of t
as stipulateuse, or drug an AE.
n authorization
Adverse
dverse reaossible prod
must deterny other A
he prescribine HCP, pati
specified be
us Advers
occurrence ieatment. Anabnormal laa medicinalhe product.
ed in the labg withdrawa
from AbbVie Page
e
actions. Howduct-relatedrmine wheth
AbbVie auth
ng, dispensient or cons
elow:
e Event
in a patient, AE can the
aboratory fin product, w
beling, as wal. Any wors
e 42 of 61
wever, event
her the horized
sing, or sumer)
which erefore nding),
whether
well as sening
Versio
If an(SAE
De
Life
Ho
ProHo
Co
PeDis
ImpReSuPre
No use or on 3.0 (22 Apr 2
n AE meetsE):
ath of Patie
e-Threaten
ospitalizatio
olongation ospitalizatio
ongenital A
rsistent osability/Inca
portant Mquiring rgical Inevent Serio
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
s any of the
ent:
ning:
on:
on:
nomaly:
or Signifapacity:
Medical EMedical
tervention ous Outcom
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
e following
An e
An ehaveinterincluoccu
An efor emefacil
of An hosp
An athat
icant An einterpatieexpesuchinfluankl
Eventor to
me:
An immhospjeopsurglistehospcongdisasponimpoinclu
vir and dasab
nfidential Informermitted witho
06.2015
criteria, it
event that re
event that, ie resultedrvention haude an eveurred in a m
event that rany length
ergency rooity.
event thatpitalized an
anomaly deresults in fe
event that rrferes with ent. Disaberiences ofh as head
uenza, andle).
important mediately lif
pitalization, pardize the gical interveed above (ipitalization, genital ano
ability/incapantaneous aortant medude allergic
buvir
mation ut prior written
is consider
esults in the
n the opinio in immead not beent that wou
more severe
results in an of time.
om visit or
t occurs wd prolongs t
etected at oretal loss.
results in a the activitie
bility is nf relatively dache, na
d accidenta
medical fe-threateninbut based patient an
ention to prei.e. death o
prolongaomaly, or acity). Addabortion or ical event.c bronchos
n authorization
red a seriou
e death of a
on of the invediate fataen taken.
uld have beform.
n admissionThis does admission
while the sthe patient's
r after birth,
condition tes of daily not intendeminor medusea, vomal trauma
event thatng or resuon medica
nd may reqevent any oof patient, ation of
persistentditionally, a
stillbirth isExamples
spasm req
from AbbVie Page
us adverse
patient.
vestigator, wality if me
This doesen fatal if it
n to the hosnot includ
to an outpa
study paties hospital st
or any ano
hat substanliving of a sed to incical signific
miting, diar(e.g. spra
t may notult in deatal judgment quire medicof the outcolife threatehospitaliza
t or signifany electivs considere
of such evquiring inte
e 43 of 61
event
would edical s not t had
spital e an atient
nt is tay.
omaly
ntially study clude cance rrhea, ained
t be th or
may cal or omes ening, ation, ficant e or d an vents nsive

Versio
11.2
The endp
Mil
Mo
Sev
11.3
The prod
Re
NoPo
If nobe p
11.4
SAEuntil treat
No use or on 3.0 (22 Apr 2
2
following depoint/data p
ld:
oderate:
vere:
3
following dduct:
asonable P
ossibility
o reasonableprovided for
4
Es will be rep30 days or
tment.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Severit
efinitions wipoint in the s
The A
The Ausua
The Aactiv
Relatio
definitions w
Possibility
Reasonab
e possibilitythe AE.
Serious
ported to Abr 5 half-live
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
treadyscinpadepe
ty
ill be used tstudy and fo
AE is transi
AE causes al activities.
AE causes ities and ma
nship to P
will be used
An AErelation
ble An AErelation
y of being re
s Adverse
bbVie from ts following
vir and dasab
nfidential Informermitted witho
06.2015
tment in ancrasias or atient hospitendency or
to rate the sor all SAEs.
ent and eas
the patient
considerabay be incapa
Pharmaceu
to assess
E where thenship betwe
E where thenship betwe
elated to pro
Event Co
the time thethe intake
buvir
mation ut prior written
n emergencconvulsion
talization, odrug abuse
severity for a
sily tolerated
discomfort
ble interfereacitating or
utical Prod
the relation
ere is evideen the prod
re is no eveen the prod
oduct is give
ollection P
e physician of the last d
n authorization
cy room or ns that door the devee.
any AE bein
d by the pat
and interru
nce with thelife threaten
duct
nship of the
ence to suduct and the
idence to sduct and the
en, an altern
eriod
obtains the dose of phy
from AbbVie Page
at home, bo not resulopment of
ng collected
tient.
upts the pat
e patient's uning.
AE to the
uggest a cae AE.
uggest a cae AE.
nate etiology
informed coysician-pres
e 44 of 61
blood ult in
drug
d as an
ient's
usual
use of
ausal
ausal
y must
onsent scribed
Versio
11.5
In th
In th
11.6
Patiedonatreatlabe
In thwithisyste
The Preg
12.0
At thworkfollowmethques
No use or on 3.0 (22 Apr 2
5
e event of a
● For AbbVbecoAbbV
● For Authbeco
e event of a
● For eby us
6
ents and thation througtment with Dl) and/or co
he event of ain 24 hoursem or notify
investigatognancy Reg
0
he end of king on bewed. This hodology astionnaires,
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Serious
an SAE, the
events fromVie authorizoming awarVie contact
events fromhorization Homing aware
a non-serio
events fromsing the eC
Pregna
heir partneghout the coDAAs only,
onsistent wit
a pregnancs of the phyying the Abb
r is encouraistry, if RBV
PlansResult
this observehalf of Ab
report will and its re
the final s
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
s and non-
e physician w
m patients uzed productre of the eperson iden
m patients uHolder (MAHe of the eve
ous AE, the
m patients usCRF system.
ancy Repo
rs should aourse of theor for 7 mo
th local treat
cy occurrencysician becobVie contact
aged to repV is included
for Dissts
vational studbVie. The
contain a esults and tudy output
vir and dasab
nfidential Informermitted witho
06.2015
-serious A
will:
using the At) report to Aevent by usntified in Se
using a nonH) of the prent.
physician w
sing the ABB.
rting
avoid pregne HCV treaonths after tment guide
ce in the paoming awart person ide
ort the pregd within the
eminatin
dy, a reporrequired sdescriptionconclusio
t and study
buvir
mation ut prior written
Adverse Ev
ABBVIE REGAbbVie withsing the eCection 11.0.
n-AbbVie prroduct withi
will:
BVIE REGI
nancy and atment and the last dos
elines for RB
atient, the phre of the prentified in Se
gnancy inforregimen.
ng and C
rt will be wtandard stun of the o
ons. The y report are
n authorization
vent Repo
GIMEN ± Rhin 24 hoursCRF system
roduct - notin 24 hours
MEN ± RBV
males shofor 30 daysse of RBV BV.
hysician wilregnancy byection 11.0.
rmation to t
Communi
written by Audy report objectives ocompleted
e the confid
from AbbVie Page
orting
RBV (or anys of the phy
m or notifyin
tify the Mars of the phy
V report to A
ould avoid s after the (or per loca
l report to Ay using the .
he voluntar
icating S
AbbVie or atemplate w
of the studeCRFs, p
dential prop
e 45 of 61
y other ysician ng the
rketing ysician
AbbVie
sperm end of
al RBV
AbbVie eCRF
ry RBV
Study
a CRO will be dy, the patient erty of

Versio
AbbVpressubm
The the Wthe publ
No use or on 3.0 (22 Apr 2
Vie and masentations) wmitted to loc
results of thWorld HealtICMJE (Inteications. Au
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
ay not be rwithout expcal authoritie
his study with Organizaernational Cuthorship wi
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
released to press writtenes by the pa
ll be made ation (WHO)Committee ll be in line
vir and dasab
nfidential Informermitted witho
06.2015
unauthorizn approval articipating c
publicly ava) Registry Nof Medical with ICMJE
buvir
mation ut prior written
zed people from AbbV
countries pe
ailable on onNetwork wh
Journal EdE’ authorship
n authorization
in any formVie. The stuer local laws
ne of the prich meet thditors) and p requireme
from AbbVie Page
m (publicatioudy results ws and regula
rimary registe requiremethrough sc
ents [68].
e 46 of 61
ons or will be ations.
tries in ents of cientific

Versio
13.0
[
[
[
[
[
[
[
[
[
[1[1
[1
[1
[1
[1
[1
No use or on 3.0 (22 Apr 2
0
[1] LozancauseGloba
[2] Chen Med S
[3] HoofnS21-9
[4] Di BisHepat
[5] PawloMicro
[6] Lavan107-1
[7] WHOhttp://w
[8] Szaboinfecti
[9] PereirC viru2013;
0] Euros1] Smith
genotHepat
2] US DPreveinfecti
3] HoughVirolo
4] GlobaorganJ Vira
5] WHOhttp://wacces
6] Prati proce
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Refere
no R, Naghaes of death fal Burden of D
SL, MorganSci 2006; 3: 4nagle JH. Co9. sceglie AM. tology 2000; otsky JM. Hbiol Infect 20nchy D. Evolv5. . Weekly www.who.into SM, Bibbyion in Latin Ara LMMB, Maus infection in 13: 1-12.
surveillance 2 DB, Bukh Jypes and 67tology 2014;
Department oention. Recomion and HCVhton M. Hep
ogy (3rd ed). al surveillancized in collab
al Hepat 1999. www.who.int
ssed July 07, D. Transmisdures: a glob
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
ences
avi M, Foremfor 20 age gDisease Studn TR. The na47-52. ourse and ou
Natural hist31: 1014-8.epatitis C v
011; 17: 105-ving epidemi
epidemiolot/docstore/wey M, Yuan YAmerica. Annartelli CMT, Mn Brazil, 200
2003; 8 (5): 9J, Kuiken C,7 subtypes: u
59: 318-27.of Health anmmendations
V related chropatitis C virusPhiladelphiace and conboration with9; 6: 35-47.
HCV t/csr/disease2014.
ssion of hepbal review. J
vir and dasab
nfidential Informermitted witho
06.2015
man K, et agroups in 199dy 2010. Lanatural history
utcome of h
tory of hepa
virus: from d6. iology of hep
ogical recoer/pdf/2000/wY et al. The n Hepatol 201Moreira RC e5 through 20
99-118. et al. Expan
updated criter
d Human Ses for prevenonic disease. ses. In: Field: Lippincott -
ntrol of hepah the Viral He
geno/hepatitis/wh
atitis C virusHepatol 200
buvir
mation ut prior written
al. Global an90 and 2010
ncet 2012; 38y of hepatitis
epatitis C. H
titis C: its im
discovery to
patitis C virus
rd. 2000;wer7503.pdf.
epidemiolog12; 11: 623-3et al. Prevale009: a cross-
nded classificria and geno
ervices - Cetion and con CDC Repords BN, KnipRaven, 1996atitis C. Re
epatitis Preve
otypes. hocdscsrlyo20
s by blood t06; 45: 607-16
n authorization
nd regional 0: a systema80: 2095-128s C virus (H
Hepatology 2
mpact on cli
eradication
s. Clin Microb
75, 17-2 gic burden o35. ence and risk-sectional stu
cation of hepotype assignm
enters for Dintrol of hepart1998; 47: 1-e DM, Howl6: 1035-58.eport of a ention Board
Avail003/en/index
transfusions 6.
from AbbVie Page
mortality froatic analysis . CV) Infection
2002; 36 (Su
nical manag
in 40 years
biol Infect 20
28. Availab
of hepatitis C
k factors of hudy. BMC Inf
patitis C virusment web res
isease Contratitis C virus -39 ey PM, eds,
WHO Cons, Antwerp, B
able x2.html#geno
and other m
e 47 of 61
om 235 for the
n. Int J
uppl 1):
gement.
s? Clin
011; 17:
ble at
C virus
epatitis fect Dis
s into 7 source.
rol and (HCV)
, Fields
ultation elgium.
at ome;
medical
Versio
[1
[1
[1
[2[2
[2
[2
[2
[2
[2
[2
[2
[2
[3
[3
[3
No use or on 3.0 (22 Apr 2
7] CentraamonRecomhttp://wnew-e
8] Albert(Supp
9] Alazacompe2010;
20] Brown21] Villano
impor29: 90
22] Thominfecti
23] Dore burde2014;
24] Davis chron
25] Strademana
26] Diensreview
27] Ghanymana
28] Backurisk of9: 509
29] Van drespoadvan
30] Everspegintcompe
31] Poynaand r2002;
32] ShiffmvirologHepat
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
al and Eastg drug usmmendationswww.aidsact
eu-member-sti A, Chemelpl 1): 17-24. wi W, Cunnensated cirrh 32: 344-55. n RS. Hepatito SA, Vlahovrtance of long08-14. as DL, Asteion: host, viraGJ, Ward J,
en (Guest Ed 21 (Suppl 1GL, Albrigh
ic hepatitis Cer DB, Wrighgement, and
stag LJ, McHw on the many MG, Stradegement, and
us LI, Boothrf all-cause m9-16. der Meer AJ,nse and al
nced hepatic son GT, Balaterferon alfa-ensated cirrhard T, McHuribavirin on l 122: 1303-1
man M, Hofmgic and histotology 1997;
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
tern Europeasers in ths for actiotioneurope.ostates-and. lo L, Benveg
ingham M, Dhosis due to
tis C and livev D, Nelson g-term follow
emborski J, al, and enviroThursz M. H
ditors Mark ): 1-4.
ht JE, Cook C in the Uniteht T, Thoma
d treatment ofHutchison JGnagement of er DB, Thom
d treatment ofroyd DB, Ph
mortality in pa
, Veldt BJ, Fl-cause morfibrosis. JAM
art L, Lee SS-2a monothehosis. Alimenutchison JG, iver fibrosis 3.
mann CM, Thologic respo26: 780-5.
vir and dasab
nfidential Informermitted witho
06.2015
an Harm Rehe new Eon. CEEHRrg/clearingho
gnù L. Natura
Dearden J, o chronic hep
er transplantaKE, Cohn S
w-up after ac
Rai RM, et onmental facHepatitis C diThursz, Gre
SF, Rosenbed States. Livas DL, Seeff f hepatitis C.G. Americanhepatitis C. G
mas DL, Seeff hepatitis C:illips BR, et
atients with h
Feld JJ, et alrtality amon
MA 2012; 308S, et al. Hisrapy in patie
nt PharmacolManns M, ein patients
hompson EBnse during i
buvir
mation ut prior written
eduction NeU member
RN brochurouse/topics/h
al history of
Foster GR.patitis C infe
ation. Nature, Thomas DLcute hepatitis
al. The natuctors. JAMA 2isease burde
egory Dore a
berg DM. Prover Transpl 2
LB. AASLD Hepatology n gastroenteGastroenteroff LB. AASLD an update. Hal. A sustain
hepatitis C. C
l. Associationng patients 8: 2584-93. tological bennts with hepa Ther 2008;
et al. Impact with chronic
B, et al. Relainterferon tre
n authorization
etwork (CEEr states are/leaflet 20hepatitis-c-am
hepatitis C.
Systematic rection. Alime
e 2005; 436: 9L. Persistencs C infection
ural history o2000; 284: 45en and strateand John Wa
ojecting futu2003; 9: 331-8D practice gu
2004; 39: 11erological asology 2006; 1D practice guHepatology 2ned virologic
Clin Gastroen
n between swith chronic
nefits of viroatitis C and a27: 542-51. of pegylate
c hepatitis C
ationship beeatment of c
from AbbVie Page
EHRN). Hepaand neighbo006. Availamong-drug-us
J Hepatol 19
review: outcoent Pharmaco
973-78. c of viremia a. Hepatology
of hepatitis C50-6.
egies to manaard). J Viral
re complicat8. idelines: dia
147-70. ssociation te130: 231-64. uidelines: dia2009; 49: 133c response rnterol Hepato
sustained viroc hepatitis
logical respoadvanced fibr
d interferon C. Gastroente
tween biochchronic hepa
e 48 of 61
atitis C orhood: ble at sers-
999; 31
ome of ol Ther
and the y 1999;
C virus
age the Hepat
tions of
gnosis,
echnical
gnosis, 35-74. reduces ol 2011;
ological C and
onse to rosis or
alfa-2b erology
emical, atitis C.
Versio
[3
[3
[3
[3
[3
[3
[3
[4
[4
[4
[4
[4
[4
[4
No use or on 3.0 (22 Apr 2
33] Brunoalpha study.
34] Di Bispeginthepat(HALT
35] Cammhistolo2004;
36] McHucombInterv
37] Zeuzehepat
38] Poynacombin pat
39] Fried GroupNEJM
40] ManncompaC: a ra
41] Hadzicomband ri
42] Jacobpegintphase
43] Shermalfa2bwho astudy.
44] Poordalfa-2SPRIN
45] EASL10.10
46] AASL50. Av
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
o S, Stroffolinis associate
. Hepatologysceglie AM, terferon to itis C: resultT-C) trial. Hema C, Di Boogy in chron 39: 333-42.
utchison JG,ination with entional The
em S, Feinmitis C. NEJMard T, McHuination interfeients with chMW, Shiffm
p). PeginterfM 2002; 347:
s M, McHutared with intandomized tryannis SJ, Sination therabavirin dose
bson IM, Mcterferon and
e 3 ADVANCman KE, Flamb and ribavirachieved an . Hepatologydad F, McConb/ribavirin (PNT-2 final res
L Recommen16/j.jhep.201
LD. Recommevailable at htt
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
ni T, Colombed with improy 2007; 45: 57
Shiffman Mprevent comts of the hepatology 200ona D, Scheic hepatitis C
, Gordon Sribavirin as
erapy Group. an SV, Rase 2000; 343: 1
utchison JG,eron alfa-2b ronic hepatit
man M, Redferon alfa-2a975-82. tchison JG, terferon alfa-rial. Lancet 2Sette H Jr,
apy in chronic. Ann Intern M
cHutchison Jribavirin in gE study. Hep
mm SL, Afdhrin for 24 or extended rap
y 2010; 52 (Sne J, Bacon
P/R) for treatsults. Hepatondations on 14.05.001 (Eendations fotp://www.hcv
vir and dasab
nfidential Informermitted witho
06.2015
bo M, et al. Soved outcom79-87.
M, Everson Gmplications opatitis C ant07; 46 (Suppepis F, et a
C: a meta-an
SC, Schiff Es initial treaNEJM 1998;
enack J, et al1666-72. Goodman Zplus ribavirinis C? Hepatody KR, et a
a plus ribavi
Gordon SC -2b plus riba2001; 358: 95Morgan TRc hepatitis CMed 2004; 1G, Dusheiko
genotype 1 Hpatology 201hal NH et al.
48 weeks inpid viral respuppl S1): 40BR et al. Bo
tment-naive pology 2010; 5Treatment opub ahead or Testing, M
vguidelines.o
buvir
mation ut prior written
Sustained virme in HCV-re
GT, et al. Pof advanced tiviral long-tel S1): 290A.al. Effect of nalysis of ind
ER, et al. Iatment for ; 339: 1485-9l. Peginterfer
Z, Ling MH,n regimen poology 2000; 3al (for the Pirin for chro
et al. PegIvirin for initia
58-65. et al. Pegin
C: a randomiz40: 346-55.
o GM et al. HCV treatmen0; 52 (Suppl Telaprevir in
n treatment-nponse: final r1A. ceprevir (BOpatients with52 (Suppl S1of Hepatitis
of print). anaging, and
org/sites/defa
n authorization
rological respelated cirrho
Prolonged anliver diseas
erm treatmen
peginterferoividual patien
nterferon alchronic hep
92. ron α-2a in p
Albrecht J.ossible for the31: 211-8. PEGASYS®
nic hepatitis
Interferon alfal treatment
nterferon-alphzed study of
Telaprevir int-naive patieS1): 427A.
n combinationnaive genotyresults of Pha
OC) combinedh hepatitis C ): 402A. C 2014. J
d Treating Hault/files/full_r
from AbbVie Page
ponse to intesis: a retros
ntiviral therapse associatent against c
on alfa-2a ont data. Hep
lfa-2b alonepatitis C. H
patients with
Is an “à lae first line tre
Internationals C virus inf
fa-2b plus rof chronic h
ha 2a and rf treatment d
n combinatioents: final re
n with pegintype 1 HCV pase 3 ILLUM
d with pegint(HCV) geno
Hepatol 201
epatitis C. 2report.pdf.
e 49 of 61
erferon-pective
py with ed with irrhosis
on liver atology
e or in epatitis
chronic
a carte” eatment
l Study fection.
ribavirin epatitis
ribavirin duration
on with sults of
terferon patients MINATE
terferon otype 1:
14; doi:
014: 1-
Versio
[4
[4
[4
[5
[5
[5
[5
[5
[5
[5
[5
[5
[5
[6
No use or on 3.0 (22 Apr 2
47] Jacobribavir(QUE2014;
48] Mann2b pluinfectiLance
49] Fornsto higtherap
50] Reddyevaluawith treatmAustra
51] Full http://wFebru
52] Lawitzhepat
53] Lalezaweeks2013;
54] Osinugenottrial. J
55] MenoproteavoluntHawa
56] Feld Jand d
57] Zeuzeombita
58] AndredasabribavirGastro
59] Ferenwithou
60] Poordfor he
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
bson IM, Dorerin in treatmeST-1): a ph doi: 10.1016s M, Marcellus ribavirin inion (QUESTet 2014; doi: s X, Lawitz Egh rates of Spy: a phase 3y KR, Zeuzeate the efficapegylated in
ment-experienalia. Availabl
prescrwww.olysio.c
uary 09, 2014z E, Mangiaitis C infectioari L, Nelsons in treatmen 58 (Suppl 1)
usi A, Meissype 1 in patie
JAMA 2013; 3n RM, Klein ase inhibitorteers with a
aii, USA. AvaiJJ, Kowdley asabuvir with
em S, Jacobasvir and das
eone P, Colobuvir achieverin in treatoenterology
nci P, Bernstut ribavirin fodad F, Hezodepatitis C with
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
e G, Foster Gent-naive pathase 3, rand6/S0140-673in P, Poordan treatment-n
T-2): a rando10.1016/S01
E, Zeuzem S,SVR in patie3 trial. Gastroem S, Zoulimacy, safety anterferon annced patiente at http://wwribing com/shared/p4. a A, Wyles on. NEJM 20 D, Hyland R
nt-naive patie): S346.
sner EG, Leents with unf310: 804-11.CE, Lawal A
r ABT-450 and without ilable at http:KV, Coakley
h ribavirin. Nbson IM, Basabuvir with ombo MG, Ees 97% andtment-experi2014; doi: 10ein D, Lalez
or HCV. NEJMde C, Trinh Rh cirrhosis. N
vir and dasab
nfidential Informermitted witho
06.2015
G et al. Simetients with chdomised, do6(14)60494-
ad F, et al. Sinaive patientomised, dou140-6736(14), et al. Sime
ents with HCoenterology.
m F, et al. A Pand tolerabilitnd ribavirin ts: the ATTAww.natap.org
informationproduct/olysi
D, et al. S13; 368: 187
R, et al. Onceents with HCV
ee YJ, et alfavorable trea. AA, et al. Phfollowing sritonavir. Ab://www.natapy E, et al. TrEJM 2014; 3aykal T, et ribavirin. NEEnejosa JV, d 100% susenced patie
0.1053/j.gastzari J, et al. AM 2014; 370:
R, et al. ABT-4EJM 2014; 3
buvir
mation ut prior written
eprevir with phronic hepat
ouble-blind, p3 (Epub ahemeprevir withts with chronble-blind, pla)60538-9 (Epprevir with P
CV genotype 2014; 146: 1Phase III ranty of simeprein chronic
AIN study. Ag/2014/APASn Olyo/prescribing
Sofosbuvir fo78-87. e daily sofosbV infection: t
l. Sofosbuviatment chara
harmacokinesingle ascenbstract of Hp.org/2009/hereatment of
370: 1594-60al. Retreatm
JM 2014; 37et al. ABT-
stained viroloents with tro.2014.04.0ABT-450/r-om: 1983-92. 450/r-ombita
370: 1973-82
n authorization
pegylated intitis C virus gplacebo-contad of print). h pegylated nic hepatitis acebo-contropub ahead ofPeginterferon
1 who relap669-79.
ndomised, doevir vs telaprhepatitis C
Abstract APASL/APASL_20ysio. Ag-information
or previously
buvir plus ribthe QUANTU
r and ribaviacteristics: a
etics and tolending dosesepDART 20epDART/hepHCV with AB3. ment of HC
70: 1604-14. -450, ritonavogic responsHCV genot
045 (Epub ahmbitasvir and
asvir and das2.
from AbbVie Page
erferon alfa 2genotype 1 introlled trial.
interferon alfC virus genoolled phase f print). and ribavirinpsed after p
ouble-blind srevir in comb
virus genoASL 2014 Br0.htm. Available
n.pdf; ac
y untreated
bavirin for 12 UM study. J H
irin for heparandomized
erability of ths in healthy009, Kohala pDART_03.htBT-450/r om
CV with ABT
vir, ombitasvse with or type 1b infhead of print)d dasabuvir
sabuvir with r
e 50 of 61
2a plus nfection Lancet
fa 2a or otype 1 3 trial.
n leads revious
study to bination otype 1 risbane,
at ccessed
chronic
and 24 Hepatol
atitis C clinical
he HCV y adult
Coast, tm. bitasvir
T-450/r-
vir, and without fection. ). with or
ribavirin
Versio
[6
[6
[6
[6[6
[6
[6
[6
No use or on 3.0 (22 Apr 2
61] Hezodinterfewith H
62] HezodtreatmGastro
63] Colomtelapr2014;
64] Marle65] Singa
Trans66] Marce
rapid results
67] ThomkineticGastro
68] Internhttp://wrole-
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
de C, Marceeron-free regHCV genotypde C, Fonta
ment-experienoenterology
mbo M, Fernárevir: the ear 63: 1150-8. y J. Efficacy,
al AG, Higgins Gastroenterellin P, Cheinvirologic ress from randopson AJ, Mcs and is thoenterology ational Cwww.icmje.o
of-authors-an
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
ellin P, Polgimens of ABe 4 infectionine H, Dorivnced patien2014; 147: 1ández I, Abdrly access p
, effectiveness PDR, Waljerol 2014; 5 (enquer H, Cursponse patienomized clinicaMuir AJ, Sulk
he stronges2010; 139: 1ommittee
org/recommed-contributor
vir and dasab
nfidential Informermitted witho
06.2015
S, et al. RBT-450/R + A. J Hepatol 2
val C et al. nts with HC32-42. urakhmanov
programme fo
ss, efficiencyee AK. A prime45): 1-4. rescu M, et ants in the laral trials. Hepakowski MS, st pre-treatm20-9. of Medic
ndations/brors.html; acce
buvir
mation ut prior written
Results from ABT-267 with2014; 60 (SupEffectivenessCV genotyp
D, et al. Safor patients w
y. Aust Prescmer on effec
al. High sustarge real-worlatology 2012et al. IL28B
ment predicto
cal Journaowse/roles-anssed July 07
n authorization
the phase h or without ppl 1): S24.s of telaprev
pe 1 infecti
fety and on-trwith advance
r 2000; 23: 1ctiveness and
ained virologild PROPHES
2; 56: 2039-5B polymorphor of SVR i
al Editorsnd-responsib7, 2014.
from AbbVie Page
2 PEARL-I ribavirin in p
vir or bocepion and cir
reatment effied hepatitis
14-5. d efficacy tria
ic response rSYS cohort c0.
hism improvein HCV-1 p
. Availablilities/definin
e 51 of 61
study: patients
revir in rrhosis.
cacy of C. Gut
als. Clin
rates in confirm
es viral atients.
e at g-the-
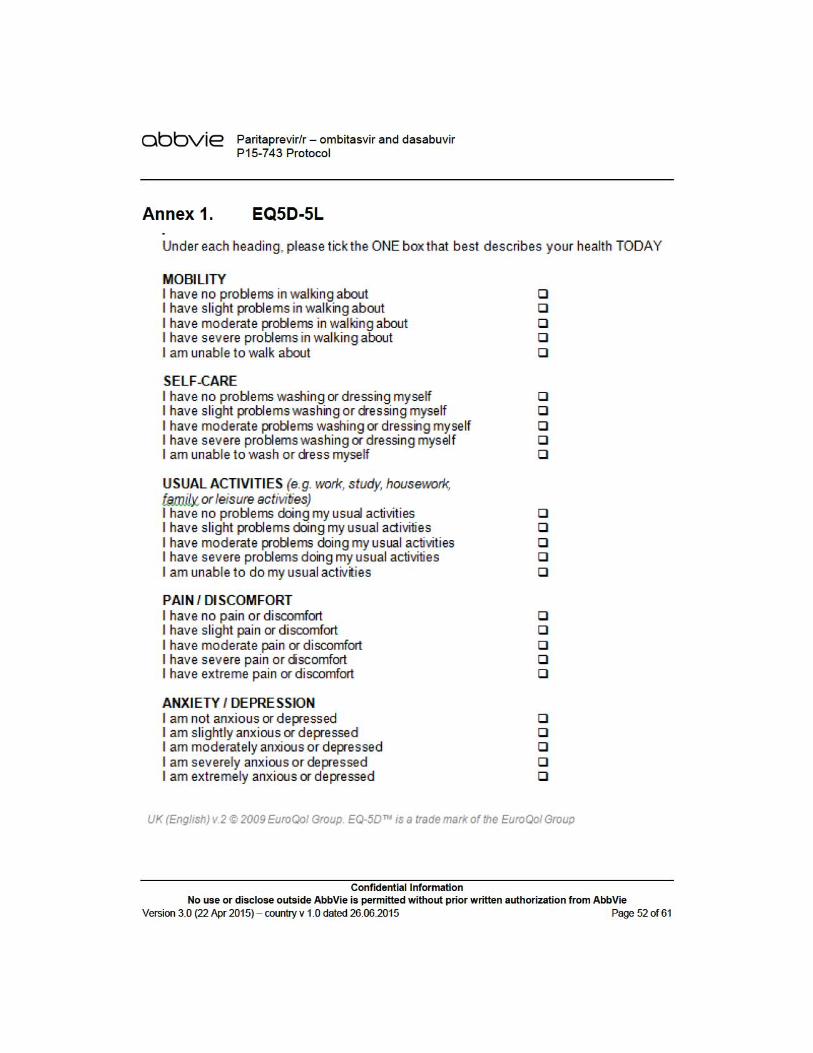
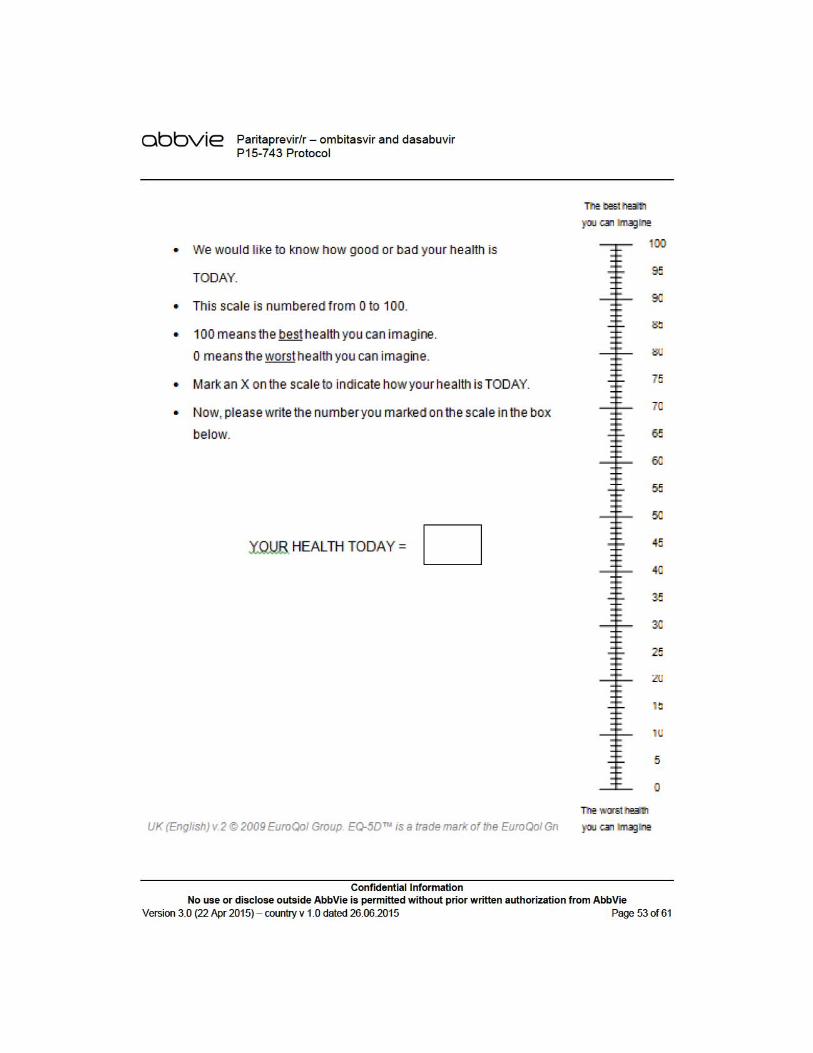
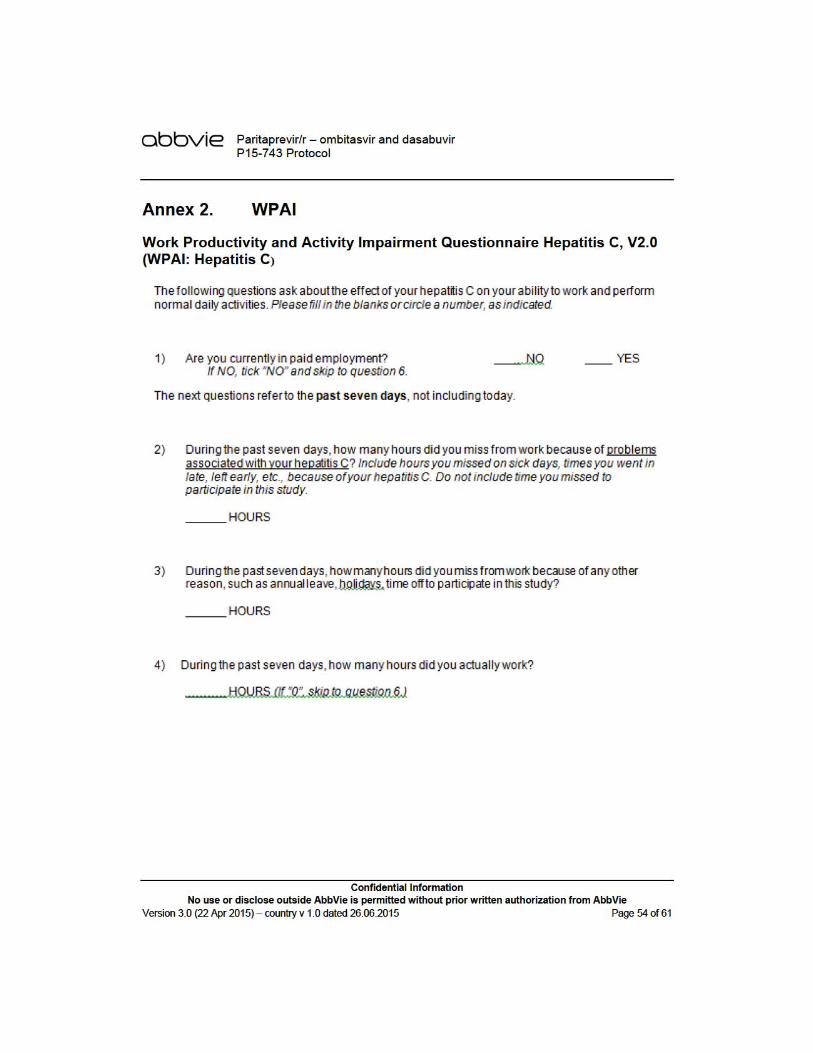
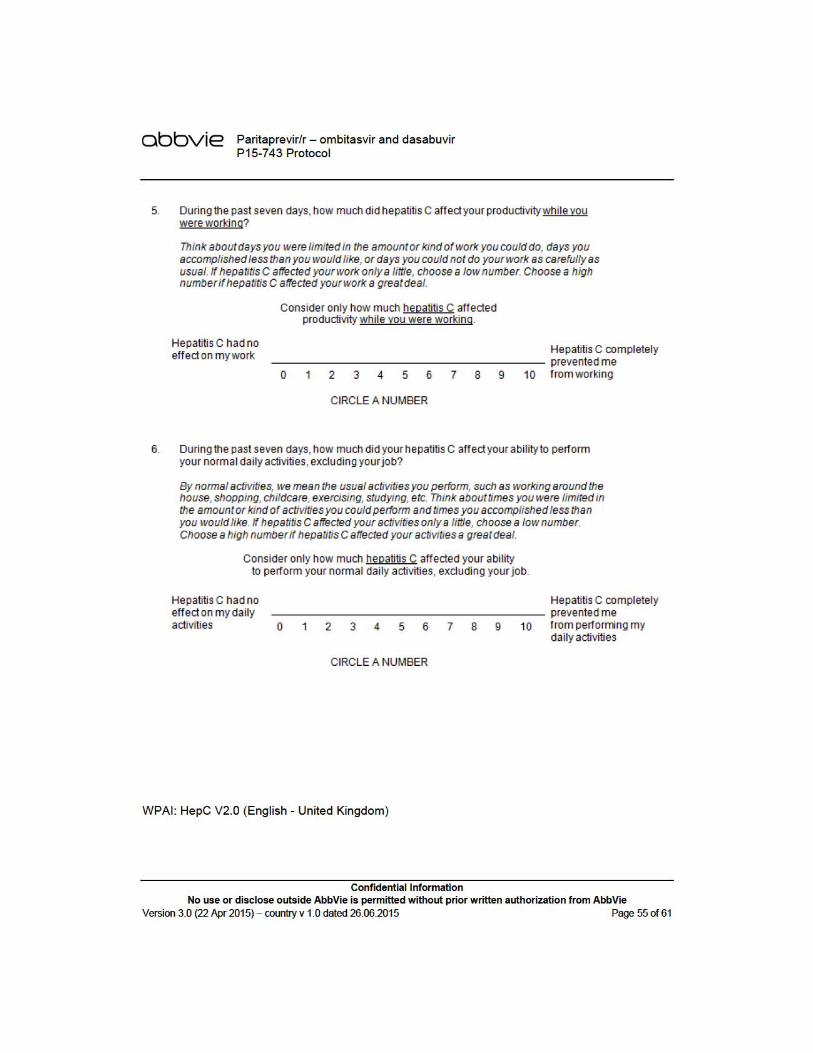
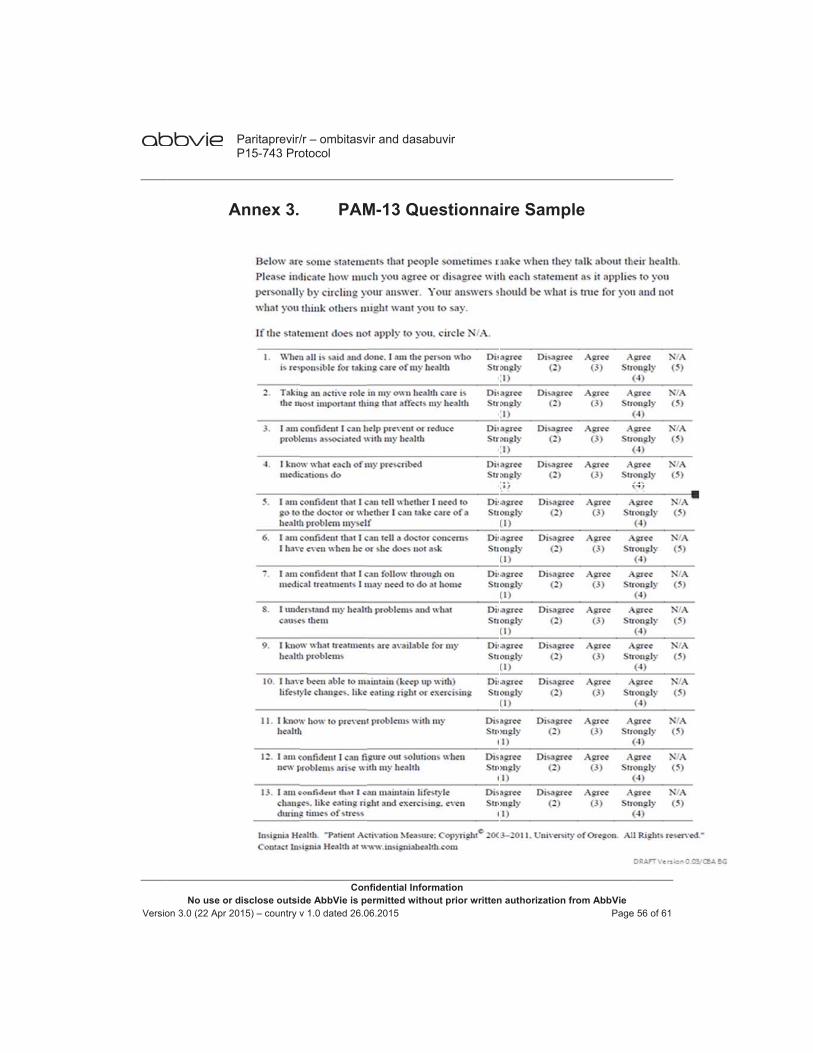
Versio
No use or on 3.0 (22 Apr 2
A
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Annex 3.
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
PAM
vir and dasab
nfidential Informermitted witho
06.2015
M-13 Que
buvir
mation ut prior written
estionna
n authorization
ire Samp
from AbbVie Page
ple
e 56 of 61
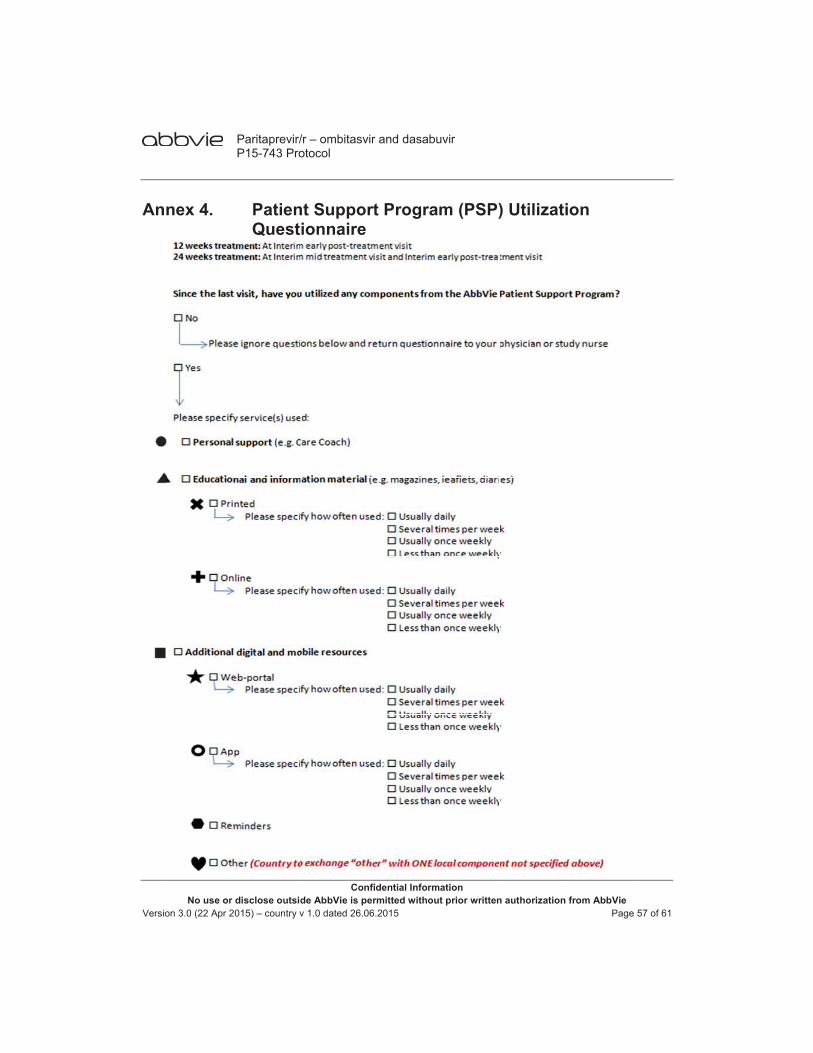
Versio
Ann
No use or on 3.0 (22 Apr 2
nex 4.
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
PatienQuest
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
nt Suppoionnaire
vir and dasab
nfidential Informermitted witho
06.2015
rt Progra
buvir
mation ut prior written
am (PSP)
n authorization
) Utilizati
from AbbVie Page
ion
e 57 of 61
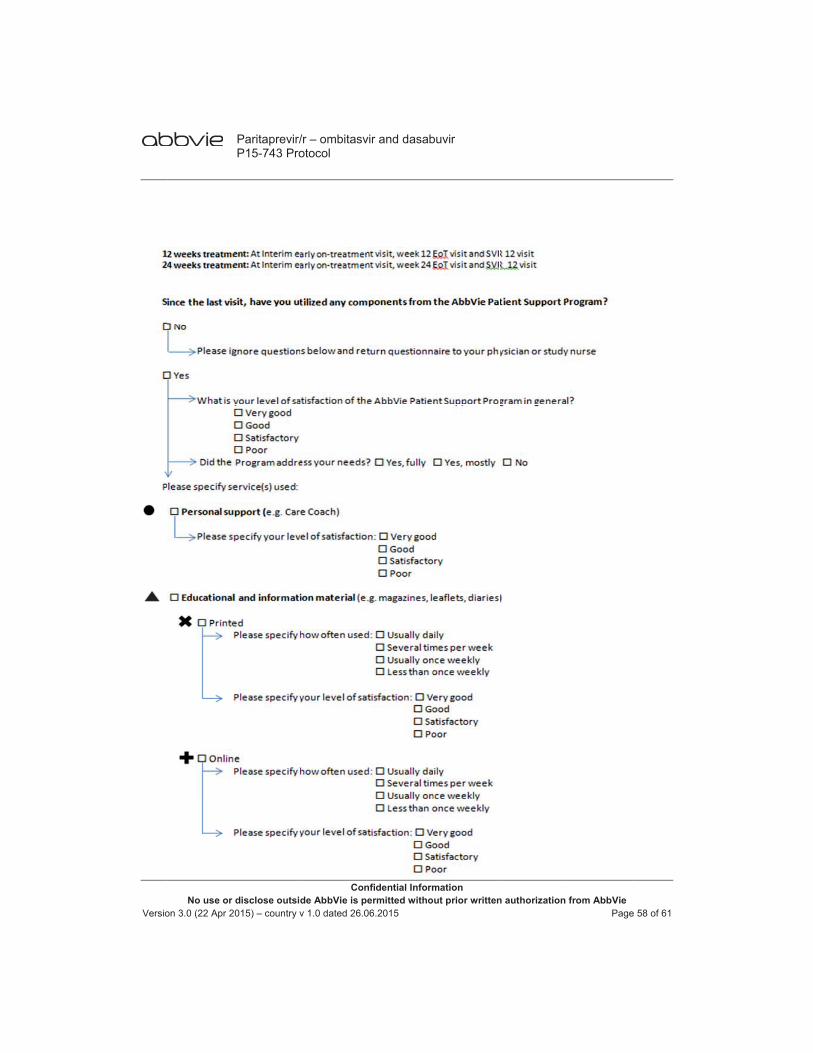
Versio
No use or on 3.0 (22 Apr 2
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
vir and dasab
nfidential Informermitted witho
06.2015
buvir
mation ut prior writtenn authorization from AbbVie
Pagee 58 of 61

Versio
No use or on 3.0 (22 Apr 2
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
vir and dasab
nfidential Informermitted witho
06.2015
buvir
mation ut prior writtenn authorization from AbbVie
Pagee 59 of 61
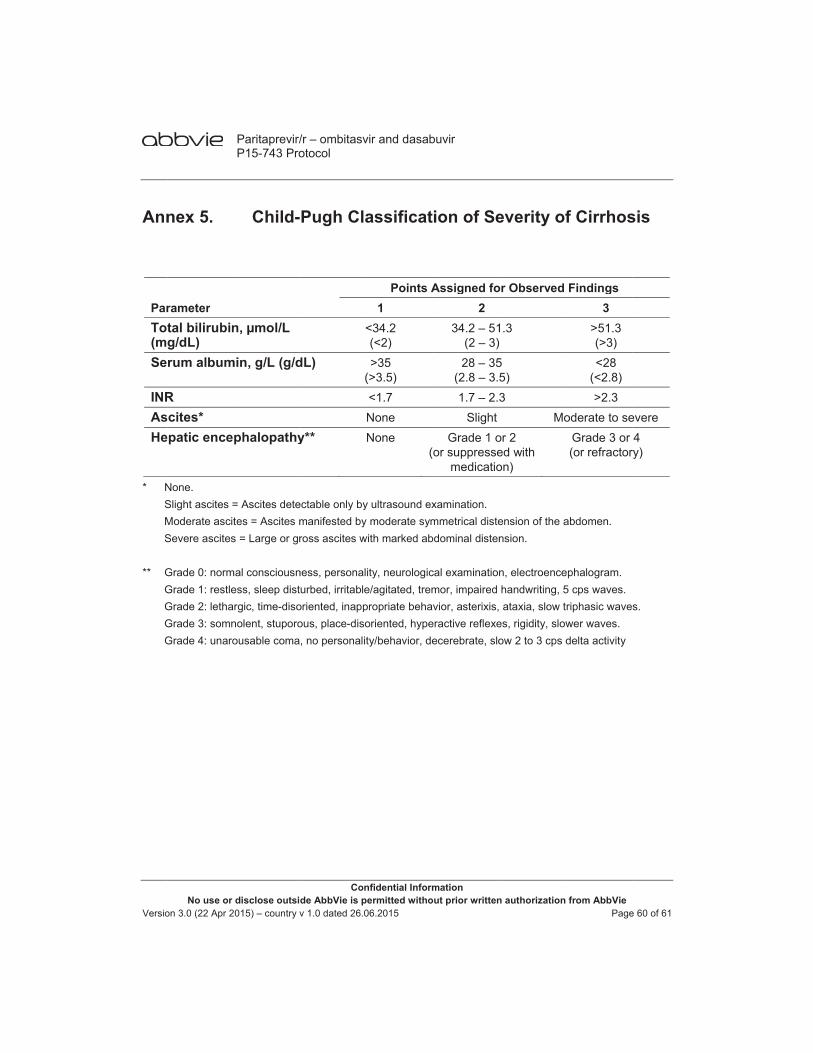
Versio
Ann
ParTot(mSe
INRAsHe
* N S M S ** G G G G G
No use or on 3.0 (22 Apr 2
nex 5.
rametertal bilirubing/dL) rum album
Rcites* patic ence
None. Slight ascites =Moderate ascitSevere ascites
Grade 0: normGrade 1: restleGrade 2: lethaGrade 3: somnGrade 4: unaro
Paritaprevir/P15-743 Pro
disclose outsid015) – country v
Child-
n, μmol/L
min, g/L (g/d
phalopathy
= Ascites detetes = Ascites ms = Large or gr
mal consciousness, sleep distrgic, time-diso
nolent, stuporoousable coma
/r – ombitasvotocol
Conde AbbVie is pv 1.0 dated 26.0
Pugh Cla
<
dL)(
y**
ectable only bymanifested by ross ascites w
ness, personalurbed, irritable
oriented, inappous, place-diso, no personalit
vir and dasab
nfidential Informermitted witho
06.2015
assificat
Points A1
<34.2 (<2) >35
(>3.5) <1.7 None None
(o
y ultrasound exmoderate sym
with marked ab
ity, neurologice/agitated, trempropriate behavoriented, hypety/behavior, de
buvir
mation ut prior written
ion of Se
Assigned fo2
34.2 – 51(2 – 3)28 – 35
(2.8 – 3.51.7 – 2.3
SlightGrade 1 o
or suppressemedicatio
xamination. mmetrical distedominal disten
cal examinationmor, impaired vior, asterixis,
eractive reflexeecerebrate, slo
n authorization
everity of
or Observed
1.3
5 5) 3
Moor 2 ed with on)
ension of the ansion.
n, electroencehandwriting, 5ataxia, slow t
es, rigidity, slowow 2 to 3 cps d
from AbbVie Page
f Cirrhos
Findings3
>51.3 (>3) <28
(<2.8) >2.3
oderate to seGrade 3 or (or refractor
abdomen.
ephalogram. 5 cps waves. riphasic waveswer waves. delta activity
e 60 of 61
sis
evere 4
ry)
s.