




Idiomas
Páginas
Jurídico

Repercusión del control del peso en
pacientes con obesidad mórbida, diabetes
mellitus tipo 2 y otras comorbilidades
asociadas
PABLO NENCLARES PEÑA. Médico Residente de Oncología Radioterápica
DIANA PAREDES RUIZ. Médico Residente de Medicina Interna
COVADONGA GÓMEZ CUERVO. Médico Adjunto de Medicina Interna
II Taller de Casos Clínicos de Diabetes Mellitus de la SOMIMACA

Antecedentes personales
Mujer de 74 años
Factores de riesgo
cardiovascular
.-Hipertensión arterial
.-Diabetes Mellitus tipo 2
.-Dislipemia
.-Obesidad (IMC 56)
.-Síndrome de apnea-hipopnea del sueño en tratamiento con BiPAP.
.-Insuficiencia renal crónica secundaria a nefroangioesclerosis +/- nefropatía
diabética.
.-Anemia normocítica y normocrómica crónica multifactorial.
.-Osteoartrosis
Antecedentes cardiovasculares:
.-Cardiopatía hipertensiva-
isquémica.
.-IAM no Q Killip I inferolateral
.-Múltiples descompensaciones de
insuficiencia cardiaca.
.-FA paroxística no anticoagulada

Antecedentes personales
Furosemida 40 mg (1-1-0) Olmesartán 20 mg (2 -0-0) Aldactone 25 mg (0-1/2-0) Insulina NPH 34UI -0-24 UI Omeprazol 20 mg (0-0-1) Rasagilina 1 mg (1-0-0) AAS-Clopidogrel (0-1-0) Atorvastatina 40 mg (0-0-1) Bromazepam 1.5 mg (1-1-2) Gabapentina 300 mg (1-0-1) Escitalopam 15 mg 1/2-1/2-0 Zolpidem 10 mg (0-0-1) Agomelatina 25 mg (0-0-2)
SITUACIÓN FÍSICA
.-Dependiente para las ABVD.
.-Obesidad mórbida con deterioro de la
movilidad y algias osteomusculares
importantes.
.-Incontinencia urinaria mixta.
.-Disnea de mínimos esfuerzos.
.-Vida cama-sillón
.-Ayuda domiciliaria.
TRATAMIENTO HABITUAL

Historia actual
Mujer de 74 años con obesidad mórbida que limita las actividades básicas de
la vida diaria y condicionan su situación basal, agravando además sus
comorbilidades asociadas.
HIPERTENSIÓN
ARTERIAL OSTEOARTROSIS
ENFERMEDAD
CARDIOVASCULAR
SAHS
OBESIDAD
DIABETES MELLITUS
TIPO 2

Evaluación de la diabetes mellitus
EVALUACIÓN COMPLETA DE LA DIABETES MELLITUS
1. Edad 2. Tipo y tiempo de evolución 3. Patrón alimenticio, actividad física, hábito corporal 4. Educación en diabetes 5. Tratamientos previos y respuesta a). Adherencia al tratamiento. b). Glucemias. c). HbA1c 6. Complicaciones agudas a). Hipoglucemia. b). Cetoacidosis diabetica/ descompensaciones hiperosmolares 7. Enfermedad metadiabética a). Microvascular: Retinopatía, nefropatía, neuropatía b). Macrovasculares: Miocardiopatía, ACVA. 8. Exploración física 9. Laboratorio

Evaluación de la diabetes mellitus
EVALUACIÓN COMPLETA DE LA DIABETES MELLITUS
1. Mujer de 74 años. 2. Diabetes mellitus tipo 2 de 28 años de evolución. 3. Inadecuado patrón alimenticio con actividad física nula y obesidad mórbida. 4. Educación en diabetes poco adecuada, con apoyo limitado. 5. Tratamientos previos y respuesta: a). Insulina NPH a dosis de 34 UI en desayuno y 24 en la cena. b). Incorrecta adherencia al tratamiento. b). Glucemias preprandriales en torno a 150 mg/dL y posprandiales de 220 mg/dL. c). HbA1c; 7,5% 6. Complicaciones agudas a). Hipoglucemias: Ninguna. b). Descompensaciones hiperosmolares. 7. Enfermedad metadiabética a). Microvascular: Retinopatía y nefropatía. b). Macrovasculares: Miocardiopatía, IAM. 8. Exploración física 9. Laboratorio

Exploración física
TA: 147/69 mmHg, FC: 68 lpm, SatO2 basal: 97%, Temperatura:36,1ºC.
Auscultación cardiaca: Arrítmica, sin soplos.
Auscultación pulmonar: Hipoventilación generalizada en ambos campos pulmonares.
Miembros inferiores: Linfedema crónico sin fóvea. No signos de TVP. Pulsos pedios
presentes. Cambios tróficos de insuficiencia venosa crónica. No úlceras.
Pruebas complementarias
HG: Hemoglobina 8.1 g/dl, VCM 86.6 fl, HCM 29.2 pg.
BQ: Glucosa 140 mg/dl, Creatinina 1.47 mg/dl, MDRM4 34 mL/min-1, Sodio 139 mEq/l, Potasio 3.88 mEq/l. Colesterol 127 mg/dl, TG 159 mg/dl, HDL 37.00 mg/dl, LDL 58 mg/dl, Acido Úrico 10.2 mg/dl.
Coagulación normal
Orina: Microalbuminuria: 16.92 mg/dl, Relación Albúmina/Creatinina (orina) 286.2944162 mg/g
OBJETIVOS
DISMINUCIÓN DEL PESO
.-Mejoría de la calidad de vida.
.-Disminución de la dependencia.
.-Mejor manejo de las comorbilidades.
.-Disminución del riesgo cardiovascular.
.-Disminución de la mortalidad.
CONTROL DE LOS OTROS
FRCV
.-Dislipemia. .-Hipertensión arterial.
CONTROL METABÓLICO Evitar la progresión del daño angiopático.

MANEJO TERAPÉUTICO Diabetes mellitus is a complex, chronic illnes requiring continuous medical care with multifactorial risk reduction strategies beyond glycemic control. Significant evidence exists that supports a range of interventions to imporve diabetes outcomes. The Satandards of care recommendations must be applied in the context of excellent clinical
care and with adjustments for individual preferences, comorbilities, and other patient factors.
-ERC
-ATR (IV)
-Hipoglucemia
-Aumento del RCV
-ERC
-Aumento de peso
-Descompensación de ICC
-Aumento de peso
-Mal control
-Hipoglucemias
-Aumento de peso

BASE DE LA TERAPIA CON INCRETINAS
Lee YS, Jun HS Anti-diabetic actions of glucagon-like peptide-1 on pancreatic beta-cells. Metabolism. 2014
Jan;63(1):9-19.
Extraído de 2014 UpToDate®
F.J. Ampudia-Blasco, Terapias basadas en el efecto incretina para el tratamiento de la diabetes tipo 2: revisión sistemática. Av Diabetol. 2008; 24(3): 193-203

BASE DE LA TERAPIA CON INCRETINAS BASE DE LA TERAPIA CON INCRETINAS
Ahrén B. Insulin plus incretin: A glucose-lowering strategy for type 2-diabetes. World J Diabetes 2014 February 15; 5(1): 40-51
Ahrén B. GLP-1 for type 2 diabetes. Ecperimental cell research. 317 (2011) 1239 – 1245
TRATAMIENTO COMBINADO INCRETINA E INSULINOTERAPIA
Conrad E, Carol Km Zinman B, Retnakaran R. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: a systematic review and Meta-analysis. Lancet. 2014: S0140-6736 (14) 61335-0. [Epub ahead of print]
Exenatide Liraglutide Lixisenatide Albiglutide Semaglutide Dulaglutide

ANÁLOGOS DE GLP-1: Lixisenatide
CONTROL METABÓLICO
1. Disminución de HbA1c: –0·44% (95% CI –0·60 to –0·29) 2. Alcance del objetivo de HbA1c de 7% o menor: RR 1·92; 95% (CI 1·43 - 2·56) 2. Control de la glucemia en ayunas (no diferencia entre grupos). 3. Disminución marcada de la glucemia posprandrial. 4. No incremento del riesgo de hipoglucemia. Datos contradictorios. 5. Disminución de necesidades de insulina.
Conrad E, Carol Km Zinman B, Retnakaran R. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: a systematic review and Meta-analysis. Lancet. 2014: S0140-6736 (14) 61335-0. [Epub ahead of print]
Riddle MC, Aronson R, Home P, Marre M, Niemoeller E, Miossec P, Ping L, Ye J, Rosenstock J. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled by established basal insulin: a 24-week, randomized, placebocontrolled comparison (GetGoal-L). Diabetes Care 2013; 36: 2489-2496

ANÁLOGOS DE GLP-1: Lixisenatide
DISMINUCIÓN DEL PESO
DISMINUCIÓN DE PESO
Conrad E, Carol Km Zinman B, Retnakaran R. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: a systematic review and Meta-analysis. Lancet. 2014: S0140-6736 (14) 61335-0. [Epub ahead of print]
Riddle MC, Aronson R, Home P, Marre M, Niemoeller E, Miossec P, Ping L, Ye J, Rosenstock J. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled by established basal insulin: a 24-week, randomized, placebocontrolled comparison (GetGoal-L). Diabetes Care 2013; 36: 2489-2496
–3·22 kg (IC –4·90 a -1·54).
-1.8 kg ± 0.2
ANÁLOGOS DE GLP-1: Lixisenatide
DISMINUCIÓN DEL PESO
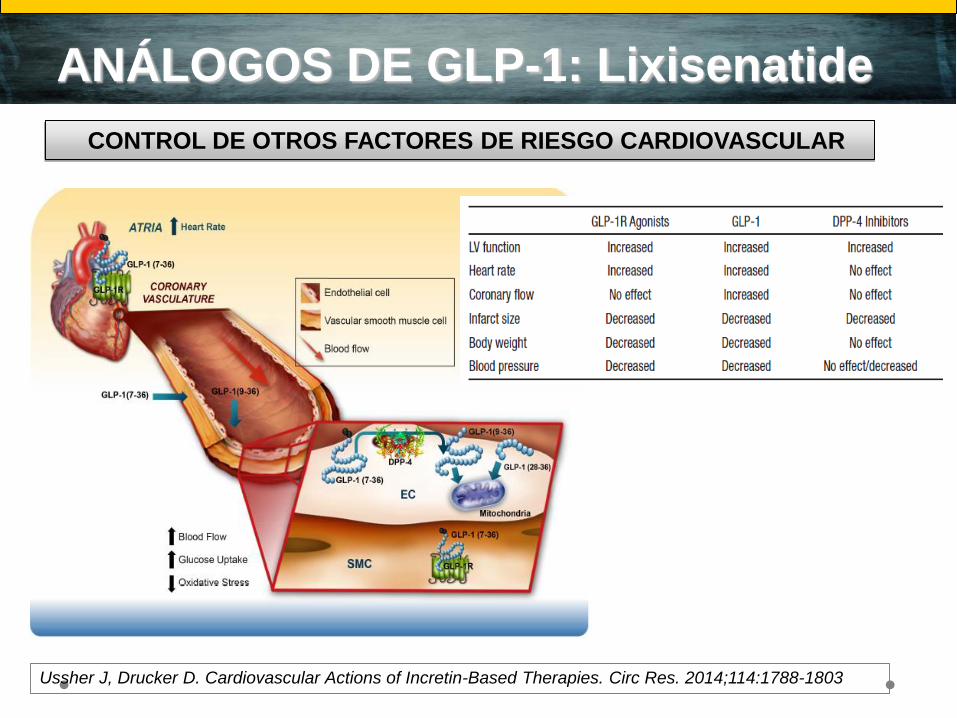
CONTROL DE OTROS FACTORES DE RIESGO CARDIOVASCULAR
Ussher J, Drucker D. Cardiovascular Actions of Incretin-Based Therapies. Circ Res. 2014;114:1788-1803

ANÁLOGOS DE GLP-1: Lixisenatide
DISMINUCIÓN DEL PESO
CONTROL DE OTROS FACTORES DE RIESGO CARDIOVASCULAR
Ussher J, Drucker D. Cardiovascular Actions of Incretin-Based Therapies. Circ Res. 2014;114:1788-1803
Bunck MC, Diamant M, Eliasson B et al.
Exenatide affects circulating
cardiovascular risk biomarkers
independently of changes in body
composition. Diabetes Care 2010; 33:
1734-1737.
Mejora el perfil lipidico.
Disminuye grasa visceral.
Disminuye circunferencia
abdominal (2,4-2,6 cm)
Posible efecto sobre los
marcadores de riesgo
cardiovascular y estrés
oxidativo (colesterol-LDL,
PCR, leptina, TNF-alfa, IL-6)
independiente a la pérdida de
masa grasa.

RESULTADOS
NPH 32-0-24 UI NPH 24-0-6 UI
+
Lixisenatide 10 ug
Glargina 10 UI
+
Lixisenatide 20 ug
Glargina 10 UI
+
Lixisenatide 20 ug
HbA1c (%) 7,5 5,7
Glucemia
preprandial
(mg/dL)
140
115 – 140
135
120
Glucemia
posprandrial
(mg/dL)
220
146
Peso (Kg) 133 129 118 117
LDL (mg/dL) 58 42
HDL (mg/dL) 37 45
TG (mg/dL) 157 135
Hipoglucemia NO NO NO NO
CONCLUSIONES
El manejo de la diabetes mellitus tipo 2 basado en
incretinas de tipo agonistas de receptores de GLP-1
logra conseguir los siguientes efectos beneficiosos:
a) Control metabólico adecuado al objetivo marcado
para esta paciente y “desescalada insulínica”.
a) Reducción del peso corporal y mejora de la calidad
de vida de la paciente.
a) Posible efecto pleiotrópico beneficioso sobre
marcadores de enfermedad cardiovascular.

Bibliografía Moretto TJ, Milton DR, Ridge TD et al. Efficacy and tolerability of exenatide monotherapy over 24 weeks in antidiabetic drug-naive patients with type 2 diabetes: a
randomized, double-blind, placbo-controlled, parallel-group study. Clin Ther 2008; 30:1448-1460.
Holst JJ. The physiology of the glucagon-like peptide 1. Physiol rev 2007; 87:1409-1439.
Diamant M, Van Gaal L, Stranks S et al. Once weekly exenatide compared with insulin glargine titrated to target in patients with type 2 diabetes (DURATION-3): an open-
label randomised trial. Lancet 2010;375: 2234-2243.
Bunck MC, Diamant M, Eliasson B et al. Exenatide affects circulating cardiovascular risk biomarkers independently of changes in body composition. Diabetes Care 2010; 33:
1734-1737.
American Diabetes Association. Standards of Medical Care in Diabetes 2014. Diabetes Care 2014. 37: 14-80
Lee YS, Jun HS Anti-diabetic actions of glucagon-like peptide-1 on pancreatic beta-cells. Metabolism. 2014 Jan;63(1):9-19 F.J. Ampudia-Blasco, Terapias basadas en el efecto incretina para el tratamiento de la diabetes tipo 2: revisión sistemática. Av Diabetol. 2008; 24(3): 193-203 Riddle MC, Aronson R, Home P, Marre M, Niemoeller E, Miossec P, Ping L, Ye J, Rosenstock J. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled by established basal insulin: a 24-week, randomized, placebocontrolled comparison (GetGoal-L). Diabetes Care 2013; 36: 2489-2496 Conrad E, Carol Km Zinman B, Retnakaran R. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: a systematic review and Meta-analysis. Lancet. 2014: S0140-6736 (14) 61335-0. [Epub ahead of print] Ussher J, Drucker D. Cardiovascular Actions of Incretin-Based Therapies. Circ Res. 2014;114:1788-1803
Bunck MC, Corner A, Eliasson B et al. One year-later treatment with exenatide vs Insuline Glargine:effects on pospandrial glycemia, lipid profiles, anda oxidative stress.
Atherosclerosis 2010; 212: 223-229.
Genugten RE, Moller-Goede DL, et al. Extra-pancreatic effects of incretin-based therapies: potential benefit for cardiovascular-risk management in type 2 diabetes. Diabetes,
Obesity and Methabolism. 2013; 15:593-606.
Nikolaidis LA, Mankad S, Sokos GG et al. Effects of glucagon-like peptide-1 in patients with acute myocardial infarction and left ventricular dysfunction after successful
reperfusion. Circulation 2004; 109:962-965.
Charbonnel B, et al. Lixisenatide plus basal insulin in patients with type 2 diabetes mellitus:a meta-analysis. Journal of Diabetes and its Complications. 2014: S1056-
8727(14)00207-4 [Epubahead of print].

GRACIAS POR SU
ATENCIÓN