





Idiomas
Páginas
Jurídico


FISIOTERAPIA EN EL CONTROL DE ESFÍNTERES EN ESPINA BÍFIDA. AVANCES EN NEUROMODULACIÓN.
Rut Antón CorreasFisioterapeuta especializada en rehabilitación de suelo
pélvico en el paciente neurológico.
VII JORNADAS MÉDICAS AMEB. “Aspectos médicos y tratamientos actuales en Espina Bífida”.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
NEUROFISIOLOGÍA MICCIONAL

Rut A
ntó
n C
orre
as w
ww
.crene.e
s

Rut A
ntó
n C
orre
as w
ww
.crene.e
sNEUROFISIOLOGÍA MICCIONAL EN EB
DISINERGIA DETRUSOR Y ESFÍNTER
IU ESTRÉS Y/O
SOBREFLUJO (Sondaje)
RIESGO TUS
U. Jonasa, D. Castro-Diazb, B.L.H. Bemelmansc, H. Madersbacherd, A.A.B. Lycklama a` Nijeholte. Neurogenic voiding disfunction. Eur Urol 2003; 44/3 (Curric Urol I–XV)

Rut A
ntó
n C
orre
as w
ww
.crene.e
sPRUEBAS DIAGNÓSTICAS VESICALES
CISTOMANOMETRÍA ECOGRAFÍA abdominal y perineal VIDEOURODINAMIA ( No siempre)
POTENCIALES EVOCADOS SOMATOSENSORIALES Y MOTORES SIMPÁTICO (--- PUDENDO)
EMG DETRUSOR PARASIMPÁTICO SACRO?????
Podnar S. Neurophysiology of the neurogenic lower urinary tract
disorders.Clinical Neurophysiology , 2007; 118: 1423–1437.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
NEUROFISIOLOGÍA FECAL

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
DEFECACIÓN; MANOMETRÍA Y ECO la falta de control superior en la función decisoria de
la defecación y en el control voluntario de los músculos del suelo pélvico son la causa de la incontinencia fecal.
aprendizaje y la automatización de estas funciones.
la demostración de denervación del esfínter anal externo suele ser imprescindible para el diagnóstico de los trastornos neurológicos. En estos casos, el estudio electromiográfico de aguja coaxial puede ser suficiente.
Podnar S, Vodusëk DB. Protocol for clinical neurophysiologic
examination of the pelvic floor.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
PACIENTES CON EB
LESIÓN DINÁMICA
Mayoría de los casos se trata de una DISINERGIA; dos tipos de pacientes:
- OBSTRUCTIVOS- INCONTINENTES ( IU/ IF)
Rut A
ntó
n C
orre
as w
ww
.crene.e
sOBJETIVOS DE LA FISIOTERAPIA EN
PACIENTES CON ESPINA BÍFIDA
INTESTINO VACÍO
AUMENTAR LA MOTILIDAD INTESTINAL
MANTENER EL RESERVORIO NATURAL DE LA FLORA INTESTINAL
TTO ESFÍNTER ANAL EXTERNO
INCONTINENCIA URINARIA
INCONTINENCIA FECAL
PROTEGER EL TUS
EVITAR INFECCIONES
TTO INCONTINENCIA
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
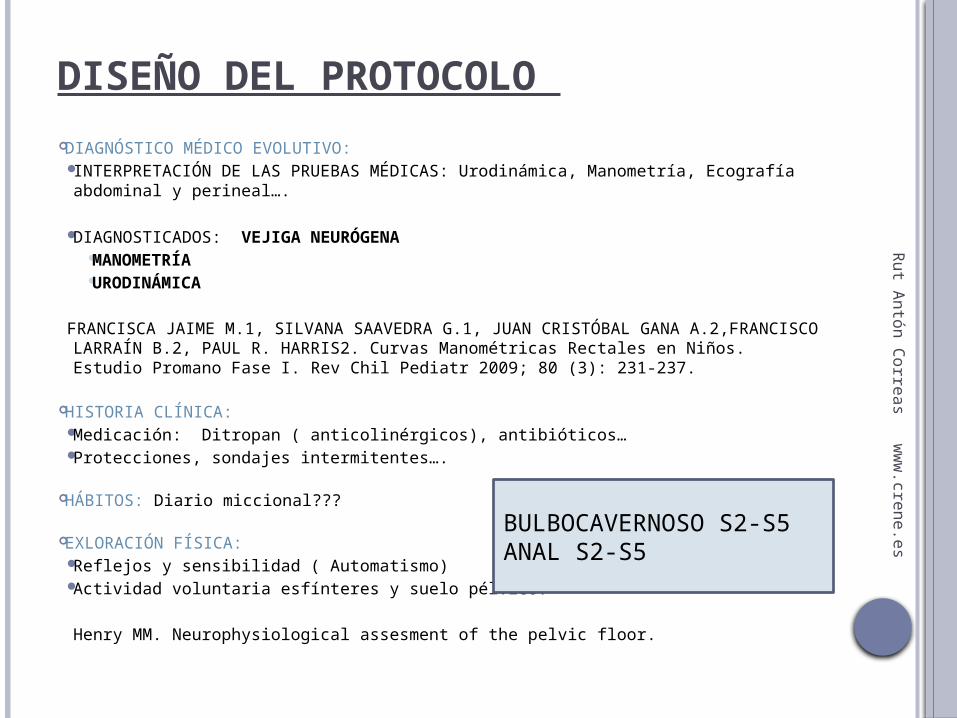
DISEÑO DEL PROTOCOLO
DIAGNÓSTICO MÉDICO EVOLUTIVO: INTERPRETACIÓN DE LAS PRUEBAS MÉDICAS: Urodinámica, Manometría,
Ecografía abdominal y perineal….
DIAGNOSTICADOS: VEJIGA NEURÓGENA MANOMETRÍA URODINÁMICA
FRANCISCA JAIME M.1, SILVANA SAAVEDRA G.1, JUAN CRISTÓBAL GANA A.2,FRANCISCO LARRAÍN B.2, PAUL R. HARRIS2. Curvas Manométricas Rectales en Niños. Estudio Promano Fase I. Rev Chil Pediatr 2009; 80 (3): 231-237.
HISTORIA CLÍNICA: Medicación: Ditropan ( anticolinérgicos), antibióticos… Protecciones, sondajes intermitentes….
HÁBITOS: Diario miccional???
EXLORACIÓN FÍSICA: Reflejos y sensibilidad ( Automatismo) Actividad voluntaria esfínteres y suelo pélvico.
Henry MM. Neurophysiological assesment of the pelvic floor.
BULBOCAVERNOSO S2-S5ANAL S2-S5

Rut A
ntó
n C
orre
as w
ww
.crene.e
sFISIOTERAPIA DE SUELO PÉLVICO EN ESPINA BÍFIDA TTO DIAFRAGMÁTICO MASAJE INTESTINAL BIOFEEDBACK PROPIOCEPTIVO y/o
DEFECATORIO Ejercicios de PFM (Pelvic Floor Muscles)
ELECTROTERAPIA: NEUROMODULACIÓN Estimulación del Tibial Posterior. Estimulacion de raíces sacras s2-s3. Estimulación del nervio pudendo.
BIOFEEDBACK DEFECATORIO CON BALÓN???? SENSIBILIDAD ANAL

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
DIAFRAGMA TORÁCICO

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
MASAJE INTESTINAL
Bronfort G, Haas M, Evans R, Leininger B, Triano J. Effectiveness of manual therapies: the UK evidence report.
Chiropr Osteopat. 2010 Feb 25;18:3
Coggrave M. Neurogenic bowel management in chronic spinal cord
injury: evidence.King’s College, London, 2007
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
BIOFEEDBACK“ Permite controlar una actividad fisiológica sobre la que habitualmente no tenemos un
control consciente o voluntario a través de la observación de dicha actividad”
OBJETIVO: HACER CONSCIENTE UNA RESPUESTA FISIOLÓGICA RELACIONADA CON
UN PROBLEMA DE SALUD ESPECÍFICO
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
BIOFEEDBACK
Poco invasivo Reproducir situaciones
normales PROPIOCEPTIVO NO EFECTOS secundarios
Déficit cognitivo COMPLEMENTARIO PADRES???FISIO???? NÚM DE SESIONES????
INDICACIONES CONTRAINDICACIONES

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
BIOFEEDBACK
Desantis DJ, Leonard MP, Preston MA, Barrowman NJ, Guerra LA. Effectiveness of biofeedback for dysfunctional elimination syndrome in
pediatrics: a systematic review. J Pediatr Urol. 2011 Jun;7(3):342-8.
Kajbafzadeh AM, Sharifi-Rad L, Ghahestani SM, Ahmadi H, Kajbafzadeh M, Mahboubi AH. Animated biofeedback: an ideal
treatment for children with dysfunctional elimination syndrome. J Urol. 2011 Dec;186(6):2379-84.
GWald A. Use of biofeedback in treatment of fecal incontinence in patients with myelomeningocele-
Pediatrics, 1981; 68:1.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
PFM TRAINNING
Vesna ZD, Milica L, Stanković I, Marina V, Andjelka S. The evaluation of combined standard urotherapy, abdominal and pelvic floor retraining in children with dysfunctional voiding. J
Pediatr Urol. 2011 Jun;7(3):336-41.
Zivkovic V, Lazovic M, Vlajkovic M, Slavkovic A, Dimitrijevic L, Stankovic I, Vacic N. Diaphragmatic breathing exercises and pelvic floor retraining in children with dysfunctional voiding.
Eur J Phys Rehabil Med. 2012 Sep;48(3):413-21.
Xiao-bing Sun⁎, Li Zhang, Yan-hua Li, Jin-liang Li, Yu-li Chen.The effects of biofeedback training of pelvic floor muscleson fecal incontinence. Journal of Pediatric Surgery (2009) 44, 2384–2387
Rut A
ntó
n C
orre
as w
ww
.crene.e
sELECTROTERAPIA
POTENCIACIÓN SP CONTROL VEJIGA E INTESTINO MÚSC PARA REINERVACIÓN HIPERACTIVIDAD VESICAL IU/IF DISMORFISMOS ANALES MOTILIDAD INTESTINAL??? MUCOSA?????
NO CONTRAINDICAIONES NI EF. SECUNDARIOS
“Emplea tecnologías de dispositivos médicos avanzados para mejorar o suprimir la actividad del sistema nervioso para el tratamiento de la enfermedad. Estas tecnologías incluyen dispositivos no implantables e implantables, que mandan estímulos eléctricos, químicos u otros agentes para modificar de manera reversible la actividad de las células del cerebro y de los nervios”
“la estimulación del nervio sacro para los trastornos pélvicos y la incontinencia; estimulación gástrica y del colon para los trastornos gastrointestinales tales como la alteración de la motilidad”
MISMO QUE MEDICACIÓN REVERSIBLE Vía AFERENTE
IFESS International Functional Electrical Stimulation Society
INS Internatinal Neuromodulation Society (1960)
Rut A
ntó
n C
orre
as w
ww
.crene.e
sELECTROTERAPIA : ESTIMULACIÓN NERVIO PUDENDO
Sheuer M, Kuijpers HC, Bleijengerg G. Effect of electroestimulation on sphincter function in neurogenic fecal continence.
Baja Frecuencia 4-10Hz Estimulación pudenda ( Hipogástrico) produciendo inhibición directa del nervio
pélvico y relajación vesical
DEMUESTRA LA INFLUENCIA DE LOS MECANISMOS SUPRAESPINALES.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
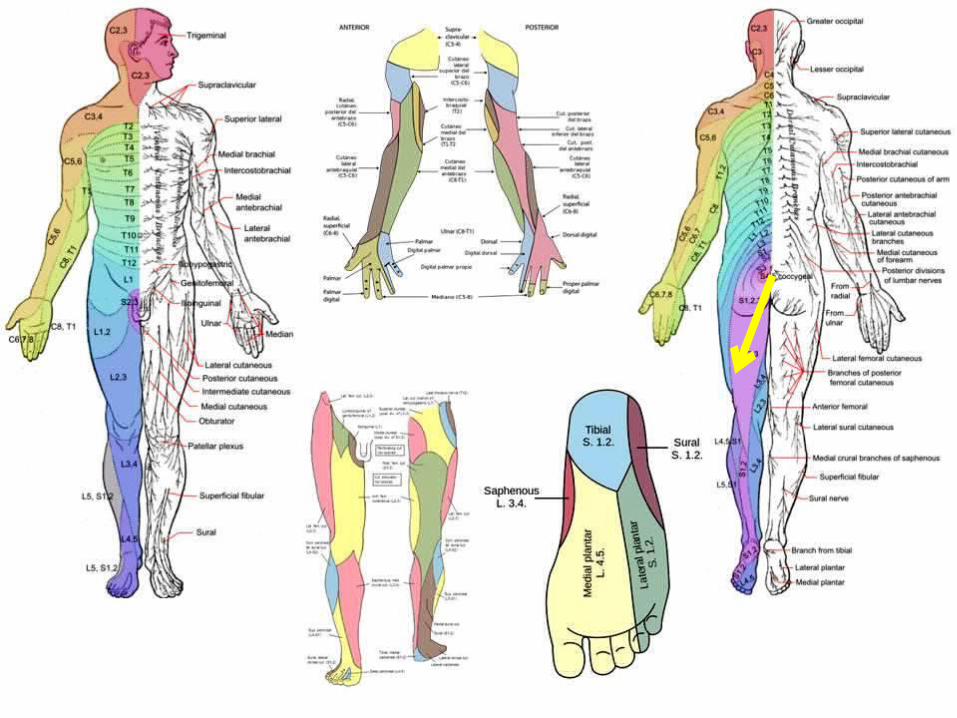
• TIBIAL POSTERIOR
(L4-S3)• •
• PUDENDO S2-S4

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
PERCUTANEOUS TIBIAL NERVE STIMULATION PTNS Andrews BJ et al. Transcutaneous posterior tibial nerve stimulation fortreatment of detrusor
hyperreflexia in spinal cord injury. J Urol, 2003;170: 926. Finazzi-Agró E. y cols. Percutaneous tibial nerve stimulation produces effects on brain
activity: study on the modifications of the long latency somatosensory evoked potentials. Neurourol Urodyn. 2009;28(4):320-4.
Scott AM et al. Long-Term Durability of Percutaneous Tibial Nerve Stimulation for the Treatment of Overactive Bladder. J Urol, 2010;183:234-240.
Amarenco G et al. Urodynamic effect of acute transcutaneous posterior tibial nerve stimulation in overactive bladder. J Urol, 2003; 169(6):2210-5.
Yoong W et al. Neuromodulative treatment with percutaneous tibial nerve stimulation for intractable detrusor instability: outcomes following a shortened 6-week protocol. BJU Int 2010 Dec;106(11):1673-6.
Finazzi Agró E et al. Posterior tibial nerve stimulation: is the once-a-week protocol the best option?. Minerva Urol Nefrol, 2005 Jun;57(2):119-23.
Kabay S. et al. The clinical and urodynamic results of a 3-month percutaneous posterior tibial nerve stimulation treatment in patients with multiple sclerosis-related neurogenic bladder dysfunction. Neurourol Urodyn. 2009;28(8):964-8.
Veloso V1, Velasquez J A1, Burti J1, Cassiano A C1, Almeida F1 Posterior tibial nerve stimulation for the treatment of overactive bladder in men: quality of life questionnaire (i-qol), overactive bladder symptoms questionnaires (oab-q), international prostatic symptoms score (ipss), and 3 days bladder diary evaluation.. 1. Universidade Federal de São Paulo. 2010.
Booth J, Hagen S, McClurg D, Norton C, Macinnes C, Collins B, Donaldson C, Tolson D. A feasibility study of transcutaneous posterior tibial nerve stimulation for bladder and bowel dysfunction in elderly adults in residential care. J Am Med Dir Assoc. 2013 Apr;14(4):270-4.
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
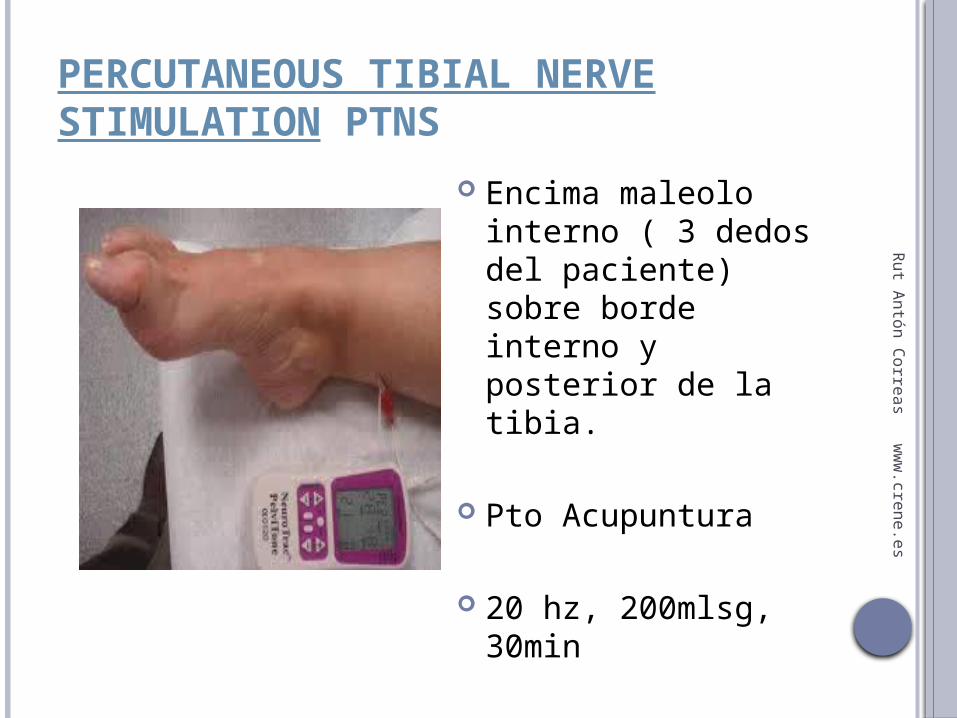
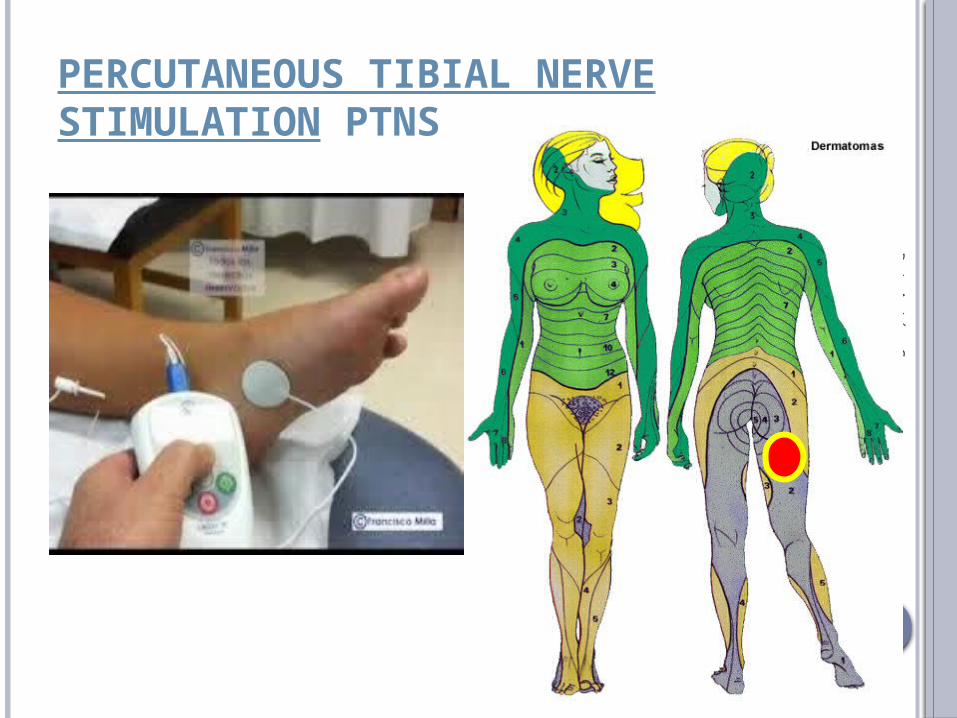
PERCUTANEOUS TIBIAL NERVE STIMULATION PTNS
Encima maleolo interno ( 3 dedos del paciente) sobre borde interno y posterior de la tibia.
Pto Acupuntura
20 hz, 200mlsg, 30min
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
PERCUTANEOUS TIBIAL NERVE STIMULATION PTNS

Rut A
ntó
n C
orre
as w
ww
.crene.e
sPERCUTANEOUS TIBIAL NERVE STIMULATION PTNS
ECA 37 NIÑOS (7.6) Grupo tto 25. TENS S2-S3/10 Hz/ 20
min/ 700mlsg. Pautas de comportamiento 3 ss/sem.
Grupo control(12) tto en zona escapular. Pautas de comportamiento.
RESULTADOS:
Lordelo P et al. Transcutaneous electrical
nerve stimulation in children with overactive bladder: a randomized clinical trial. J
Urol.2010 Aug;184(2):683-9.
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
PERCUTANEOUS TIBIAL NERVE STIMULATION PTNS
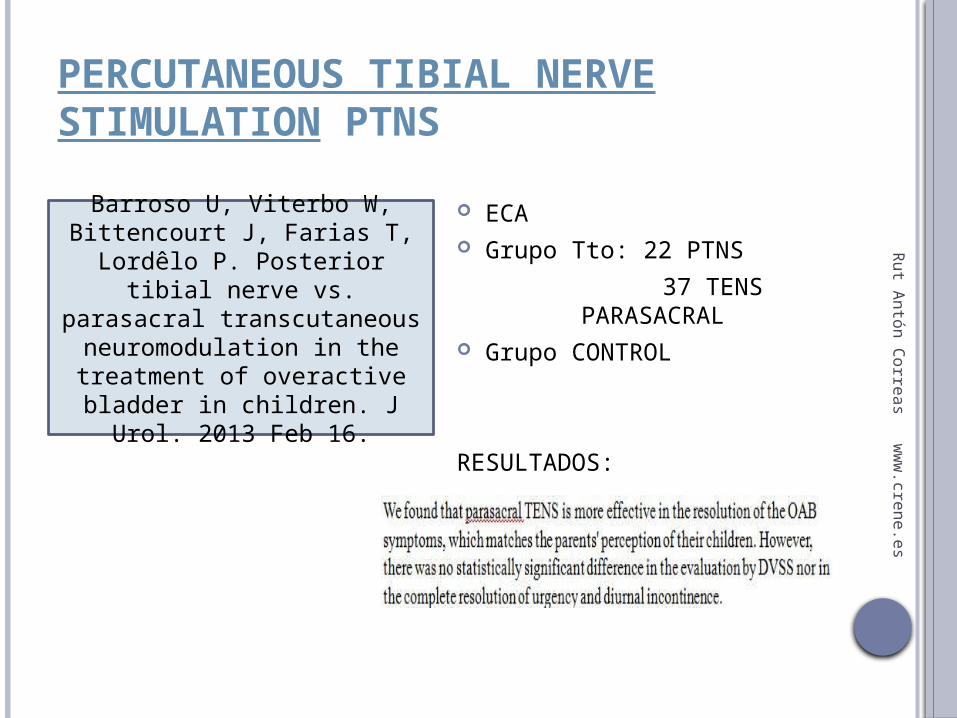
ECA Grupo Tto: 22 PTNS
37 TENS
PARASACRAL Grupo CONTROL
RESULTADOS:
Barroso U, Viterbo W, Bittencourt J, Farias T, Lordêlo
P. Posterior tibial nerve vs. parasacral transcutaneous
neuromodulation in the treatment of overactive
bladder in children. J Urol. 2013 Feb 16.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
PERCUTANEOUS TIBIAL NERVE STIMULATION PTNS
Veiga ML, Lordêlo P, Farias T, Barroso U Jr. Evaluation of constipation after parasacral transcutaneous electrical
nerve stimulation in children with lower urinary tract dysfunction - A pilot
study. J Pediatr Urol. 2012 Aug 1
Leong LC, Yik YI, Catto-Smith AG, Robertson VJ, Hutson JM, Southwell BR. Long-term effects of transabdominal
electrical stimulation in treating children with slow-transit constipation. Randomized controlled trial. J Pediatr
Surg. 2011 Dec;46(12):2309-12.
Collis B, Norton C, Maeda Y. Percutaneous
tibial nerve estimulation for slow transit
constipation. A pilot study. Colorectal Dis,
2012, Apr 14 (4): 165-170.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
ESTIMULACIÓN RAÍCES SACRAS SNS
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
ESTIMULACIÓN RAÍCES SACRAS SNS
DOLOR PÉLVICO CRÓNICO FRECUENCIA 10-20 PULSOS/ SG sobre raíces S3.
Tanagho EA, Schmidt RA, Orvis BR. Neural stimulation for control of voiding dysfunction: a preliminary report in 22 patients with serious neuropathic voiding disorders.
Thon WF, Baskin LS, Jonas U, Tanagho EA, Schmidt RA. Neuromodulation of voiding dysfunction and pelvic pain.
Bosch JL, Groen J. Sacral (S3) segmental nerve stimulation as a treatment for urge incontinence in patients with detrusor instability: results of chronic electrical stimulation using an implantable neural prothesis.
Janknegt RA, Weil EH.J, Eedermans PHA. Improving neuromodulation technique for refractory voiding dysfunctions: two-stage implant.
Weil EH, Ruiz Cerdá JL, Eerdmans PH.A, Janknegt RA, Van Kerrebroeck PE. Clinical results of sacral neuromodulation for chronic voiding dysfunction using unilateral sacral foramen electrodes
Gstaltner K, Rosen H, Hufgard J, et al. Sacral nerve stimulation as an option for the treatment of faecal incontinence in patients suffering from cauda equina syndrome. Spinal Cord 2008;46:644–7.
Krogh K, Christensen P. Best Practice & Research Clinical Gastroenterology , 2009; 23: 531–543.
MEJORA LA AFERENCIAMontero-Homs J, Muñoz-Duyos A, Del Río C. Transtornos de la función esfinteriana. Fisiopatología y estudio neurofisiológico.
Rut A
ntó
n C
orre
as w
ww
.crene.e
sRESULTADOS NEUROMODULACIÓN
RETO TODAVÍA DESCONOCIDO
TTO BAJA MORBILIDAD
VÍAS AFERENTES
NEUROMODULACIÓN IDEAL : nervio pene, clítoris y raíces sacras por su proximidad entre electrodos.
ALTERNATIVA AL TTO FARMACOLÓGICO A LARGO PLAZO (efectos secundarios, intolerancias, adiccón, toxicidad, efectos secundarios)

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
HÁBITOS
80 MMC ( De 5 a 18) Dieta. Entrenamiento defecatorio con evacuación digital. Si etto no posible enemas retrógados y/o anterógrados.
RESULTADOS: 8 DE 80 CONTINENTES
50 DE 72 (69%) PSEUDO-CONTINENCIA
Fecal pseudo-continence was achieved in 58 of 80 patients (72.5%) with myelomeningocele.
S. Vande Velde, S. Van Biervliet, K. Van Renterghem, E. Van Laecke, P. Hoebeke and M. Van Winckel. Achieving fecal continence in patients with spina bifida: A descriptive cohort study. Journal of Urology, 2007; 178: 2640-2644.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
HÁBITOS
REFLEJO GASTROCÓLICO: Más fuerte en la mañana
Aaronson MJ, Freed MM, Burakoff R. Colonic myoelectric activity in persons with spinal cord injury. Dig Dis Sci 1985; 30: 287-294.
Malone P, Wheeler R and Williams J: Continence in patients with spina bifida: long term results. Arch Dis Child 1994;70: 107.
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
FISIOTERAPIA IU
TTO DIAFRAGMÁTICO BIOFEEDBACK EJERCICIOS PFM ELECTROESTIMULACIÓN ( Baja Frecuencia) NEUROMODULACIÓN
ESTIMULACIÓN EXTEROCEPTIVA
DIETA/ HÁBITOS posturales y evacuatorios

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
FISIOTERAPIA IF
A) DISFUNCIÓN RECTO-ANAL BIOFEEDBACK SENSIBILIDAD RECTAL MANIOBRA DE DEFECAR NEUROMODULACIÓN
B) TRÁNSITO INTESTINAL TTO DIAFRAGMÁTICO MASAJE INTESTINAL NEUROMODULACIÓN
ESTIMULACIÓN EXTEROCEPTIVA
DIETA/ HÁBITOS posturales y evacuatorios
Rut A
ntó
n C
orre
as w
ww
.crene.e
sTRATAMIENTO DE FISIOTERAPIA EN EB
URODINÁMICA ACTUAL
HISTORIA CLÍNICA EXPLORACIÓN
TRATAMIENTO????
MANOMETRÍA ANORECTAL ACTUAL
HISTORIA CLÍNICA EXPLORACIÓN
TRATAMIENTO???
VEJIGA-URETRA RECTO-ANO
Killam PE, Jeffries JS, Varni JW. Urodynamic biofeedback treatment of urinary incontinence
in children with myelomeningocele. Biofeedback Self LRegul. 1985
Jun;10(2):161-71.
Kajbafzadeh AM, Sharifi-Rad L, Baradaran N, Nejat F. Effect of pelvic floor interferential
electrostimulation on urodynamic parameters and incontinency of children with myelomeningocele and detrusor
overactivity.Urology. 2009 Aug;74(2):324-9.
Kajbafzadeh AM et al. Efficacy of transcutaneous functional electrical
stimulation on urinary incontinence in myelomeningocele: results of a pilot study. Int Braz J Urol. 2010 Sep-Oct;36(5):614-20.
Blanco Fernández G, Blesa Sierra I, Núñez Núñez R, Martínez Quintana R, Vargas
Muñoz I, Blesa Sánchez E. Re-education of the anal sphincter in patients with
myelomeningocele An Esp Pediatr. 2002 Feb;56(2):111-5.
Wald A. Biofeedback for neurogenic fecal incontinence: rectal sensation is a determinant of outcome.J Pediatr Gastroenterol Nutr. 1983
May;2(2):302-6.
Leong LC, Yik YI, Catto-Smith AG, Robertson VJ, Hutson JM, Southwell BR. Long-term effects of transabdominal
electrical stimulation in treating children with slow-transit constipation. Randomized
controlled trial. J Pediatr Surg. 2011 Dec;46(12):2309-12.

Rut A
ntó
n C
orre
as w
ww
.crene.e
sTRATAMIENTO DE FISIOTERAPIA EN EB
Chang HS, Myung SJ, Yang SK, Jung HY, Kim TH, Yoon IJ, Kwon OR, Hong WS, Kim JH, Min YI. Effect of electrical stimulation in constipated patients with impaired rectal sensation. Int J Colorectal Dis. 2003 Sep;18(5):433-8.
Veiga ML, Lordêlo P, Farias T, Barroso U Jr. Evaluation of constipation after parasacral
transcutaneous electrical nerve stimulation in children with lower urinary tract dysfunction - A
pilot study. J Pediatr Urol. 2012 Aug 1.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
EXPERIENCIA EN CLÍNICA…….
Consistencia de las heces. Aumento de sensibilidad
rectal. Mejora de evacuación
activa. Disminución de infecciones. Reducción de prolapsos
esfinterianos. Preparación del sistema
para futuras intervenciones.
PTNS Y SNS alternas. NO EXISTE LA TÉCNICA
PERFECTA. Combinación de todas.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
LÍNEAS DE INVESTIGACIÓN ECAs con mayor muestra de pacientes y
grupo control. Diseño metodología más rigurosa y valoraciones después del tto.
Electroestimulación a frecuencias más bajas.
MAYOR EXPERIENCIA CLÍNICA
Hallazgos de gran influencia de la PTNS y SNS en la incontinencia fecal respecto al TRÁNSITO Y MUCOSA INTESTINAL. (SISTEMA ENTÉRICO AUTÓNOMO)

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
PACIENTES DE ESPINA BÍFIDA…..
Mejores resultados en pacientes que caminan FISIOTERAPIA mejorará la HIPERACTIVIDAD
VESICAL E IF ( PSEUDO-CONTINENCIA) INDICADA CUANDO NO ES POSIBLE CIRUGÍA COMPLEMENTARIA A CUALQUIER TTO NO EXISTE UNA TÉCNICA AISLADA PARA
TRATAMIENTO DE ESFÍNTERES EN EB ( Multidisciplinar)
Rut A
ntó
n C
orre
as w
ww
.crene.e
s
BIBLIOGRAFÍA I Campbell Urología. 8ª Edición. Tomo 3. Walsh, Retik,
Vaughan, Wein. Editorial Panamericana, 2005. Patología funcional urológica y urodinámica
pediátricas. Carlos Gutiérrez Segura. Editorial siglo S.L. 2008.
Pelvic Floor Re-education. Principles and Practice.2ª Edición. Kaven Bessler, Bernhard Schüssler, Kathryn L. Burgio, Kate H. Moore, Peggy A. Norton, Stuart L. Stanton. Editorial Springer, 2008.
Incontinence.4ª Edición. Paul Abrams, Linda Cardozo, Saad Khoury, Alan Wein. 2009.
Pelvic Organ Disfunction in neurological diseases. Clinical management and rehabilitation. 1ª Edición. Clare J. Fowler, Jalesh N. Panicker, Anton Emmanuel. Cambridge Medicine. 2010.

Rut A
ntó
n C
orre
as w
ww
.crene.e
s
BIBLIOGRAFÍA II Lewis JM, Cheng EY. Non-traditional management of the neurogenic bladder: tissue
engineering and neuromodulation. ScientificWorldJournal 2007;7:1230–41. Keppene V, Mozer P, Chartier-Kastler E, Ruffion A. Neuromodulation in the management of
neurogenic lower urinary tract dysfunction. Prog Urol 2007;17:609–15. Ishigooka M, Hashimoto T, Izumiya K, Katoh T, Yaguchi H, Nakada T, et al. Electrical pelvic
floor stimulation in the management of urinary incontinence due to neuropathic overactive bladder. Front Med Biol Eng 1993;5:1–10.
Jean-Jacques Wyndaele. Conservative treatment of patients with neurogenic bladder. European Urology. 2008; 7: 557-565.
Manfred Stöhrer, Bertil Blok; David Castro-Díaz, et al. Guidelines on neurogeniclower urinary tract dysfunction. Review Article. European Urology, 2009;56: 81-88.
Abdol-Mohammad Kajbafzadeh, Lida Sharifi-Rad, Nima Baradaran, and Farideh Nejat. Effects of pelvic floor interferencial stimulation on urodynamics parametres and incontinence of children with myelomeningocele and detrusor overactivity.Urology. 2009; 74: 324–331.
McGuire EJ et al. Treatment of motor and sensory detrusor instability by electrical stimulation.J Urol, 1983; 129.
Stoller ML. Afferent nerve stimulation for pelvic floor dysfunction. Eur Urol1999;35 (supp2l ):1 – 196.
Finazzi-Agró E. y cols. Percutaneous tibial nerve stimulation produces effects on brain activity: study on the modifications of the long latency somatosensory evoked potentials. Neurourol Urodyn. 2009;28(4):320-4.
Kenneth MP et al. Randomized Trial of Percutaneous Tibial Nerve StimulationVersus Extended-Release Tolterodine: Results From the Overactive Bladder Innovative Therapy Trial. J Urol, 2009; 182:1055-1061.
GRACIAS POR SU ATENCIÓN
Top Related