


Idiomas
Páginas
Jurídico


Estratificación de riesgo en Estratificación de riesgo en FA: Sangrado vs. Embolismo FA: Sangrado vs. Embolismo
Nuevos aspectosNuevos aspectos
Adrian Baranchuk MD FACCAdrian Baranchuk MD FACCAssociate Professor of MedicineAssociate Professor of Medicine
Heart Rhythm ServiceHeart Rhythm ServiceQueen’s UniversityQueen’s University
CES, Medellín, ColombiaCES, Medellín, ColombiaAgosto 2011Agosto 2011

2
EMBOLIA SANGRADO

EMBOLIA
SANGRADO
Excesiva anticoagulación
Cómo determianr el riesgo de embolia Cómo determianr el riesgo de embolia en pacientes con FA?en pacientes con FA?

CHADS 2 SCORECHADS 2 SCORE
Parámetros clínicos sencillos y fáciles de recordar
Cuándo anticoagular?Cuándo anticoagular?

VIEJAS GUIAS
CHADS2 CHADS2 ≥ 2≥ 2(Warfarina)(Warfarina)
NUEVAS GUIAS
CHADS2 CHADS2 ≥ 1≥ 1(Dabigatran)(Dabigatran)
Pero el CHADS2 Score no analiza Pero el CHADS2 Score no analiza todas las variables…todas las variables…
CHADS2 =CHADS2 = 1 1(Aspirina)(Aspirina)

CHACHA22DSDS2 2 VASVASC C ScoreScore
Y hay mas…Y hay mas…

Apnea del Sueño y FA:Apnea del Sueño y FA:Accidente CerebrovascularAccidente Cerebrovascular CHADCHADSSS2 score?S2 score?

Todo muy lindo…debemos anticoagular a los pacientes de riesgo,Todo muy lindo…debemos anticoagular a los pacientes de riesgo,Pero como evaluamos el riesgo de sangrado?Pero como evaluamos el riesgo de sangrado?
SCORE > 3 = RIESGO AUMENTADO
Veamos un poco la evidencia (solo un poco…)

Relative Risk Reduction of Stroke in Atrial Relative Risk Reduction of Stroke in Atrial Fibrillation: Fibrillation:
Warfarin Compared with PlaceboWarfarin Compared with Placebo
Lip GYH et al. BMJ 2002; 325: 1022–1025.

Uso Uso REALREAL de la Warfarina de la WarfarinaYear Survey Population % Warfarin
1999 ATRIA Study
N = 11,082 USA HMO; no CI
60% high risk patients
2005 NABOR Study
N = 945 USA
hospital/community
55% high risk patients
2006 EuroHeart Survey
N = 2706; outpatients 35 European countries
64%
2006 Hylek et al
N = 402; age 65 USA, teaching hospital
51% ondischarge
2006 Birman-Deych et al
N = 16,007USA Medicare
49%

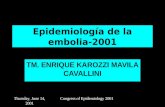
Uso de Warfarina en la práctica Uso de Warfarina en la práctica diaria:diaria:
IniciaciónIniciación
Gallagher AM, et al. Gallagher AM, et al. J Thromb HaemostJ Thromb Haemost. 2008;6:1500-1506.. 2008;6:1500-1506.
Perc
ent
Years after diagnosis
Age 40 – 64
Age 85 +Age 80 – 84Age 75 – 79Age 70 – 74Age 65 – 69
00 2 4 60
20
40
60
80
100100
•41,000 chronic AF treated by GPs in UK41,000 chronic AF treated by GPs in UK•Administrative database study Administrative database study •Diagnosed after Jan 2000Diagnosed after Jan 2000

0 2 4 60
20
40
60
80
100
Perc
ent
Years after starting treatment
Age 40 – 64
Age 85 +Age 80 – 84Age 75 – 79Age 70 – 74Age 65 – 69
Gallagher AM, et al. J Thromb Haemost. 2008;6:1500-1506
Uso de Warfarina en la práctica Uso de Warfarina en la práctica diaria:diaria:
DiscontinuaciónDiscontinuación

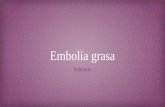
In Community Practice, Warfarin-Treated Patients In Community Practice, Warfarin-Treated Patients With Atrial Fibrillation Were in Therapeutic Range With Atrial Fibrillation Were in Therapeutic Range
51% of the Time51% of the Time
47473636
51515656
4949 52526363
5555
42425151
0
20
4040
6060
80
100
Samsa20002
n= 125
Samsa20002
n= 61
McCormick20013
n= 174
Matchar 20034*
n= 363
Matchar 20034*
n= 317
Matchar 20034*
n= 317
Go20035
n= 7445
Shen20076
n= 11,016
Nichol20087*
n= 756
Subtotal†Tim
e in
The
rape
utic
Ran
ge, (
%)
Tim
e in
The
rape
utic
Ran
ge, (
%)
Time in Therapeutic Range in Different Community-Practice StudiesTime in Therapeutic Range in Different Community-Practice Studies

Stroke. 2009;40:235-240Stroke. 2009;40:235-240
• 920 patients, acute stroke, known AF in Ontario 920 patients, acute stroke, known AF in Ontario 2003-72003-7
• no contra-indications to warfarinno contra-indications to warfarin


Warfarina: algunas conclusionesWarfarina: algunas conclusiones
50% of ideal patients started on warfarin50% discontinue within 3-5 years50% of those on warfarin have adequate
control of INRRisk of Bleeding (2-fold increase in ICH)Multiple drug and diet interactions

Ventajas y desventajas de losVentajas y desventajas de losNuevos anticoagulantesNuevos anticoagulantes

Nuevos anticoagulantes: Inhibición Indirecta de la TrobminaNuevos anticoagulantes: Inhibición Indirecta de la Trobmina
Pasos de la Coagulación Cascada de la coagulación
Iniciación
Propagación
Formación de Fibrina
TF/VIIa
X XI
IXaVIIIa
VaXa
II
IIaFibrinogen
Thrombin
Fibrin
RivaroxabanApixaban
BetrixabanEndoxaban
DU 176bDirect
binding
IdraparinuxIdrabiotaparinu
xIndirect
inhibition
Dabigatran etixilateDabigatran etixilateAZD-0837AZD-0837


Characteristic Dabigatran 110 mg
Dabigatran 150 mg Warfarin
Randomized 6015 6076 6022Mean age (years) 71.4 71.5 71.6Male (%) 64.3 63.2 63.3CHADS2 score (mean) 0-1 (%) 2 (%) 3+ (%)
2.1
32.634.732.7
2.2
32.235.232.6
2.1
30.937.032.1
Prior stroke/TIA (%) 19.9 20.3 19.8Prior MI (%) 16.8 16.9 16.1CHF (%) 32.2 31.8 31.9Baseline ASA (%) 40.0 38.7 40.6Warfarin Naïve (%) 49.9 49.8 51.4
Connolly SJ et al. NEJM 2009;361:1139-51
RELY- Baseline Characteristics

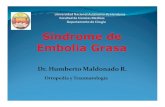
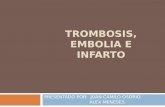
Stroke o Embolismo sistémicoStroke o Embolismo sistémico
0.50 0.75 1.00 1.25 1.50
Dabigatran 110 vs. Warfarin
Dabigatran 150 vs. Warfarina
Non-inferiorityp-value<0.001
<0.001
Superiorityp-value 0.34
<0.001
Margin = 1.46
HR (95% CI)
Warfarin betterDabigatran better
Connolly SJ et al. NEJM 2009;361:1139-51.

} 34% } 34% RRRRRR
Connolly SJ et al. NEJM 2009;361:1139-51
Y que pasa si no puedo indicar anticoagulantes?...doy Aspirina?Y que pasa si no puedo indicar anticoagulantes?...doy Aspirina?

Connolly SJ et al. NEJM 2011;364:806-17.
AVERROES Study


Connolly SJ et al. NEJM 2011;364:806-17.Connolly SJ et al. NEJM 2011;364:806-17.
Mejor para prevenir embolismo
Sin mayor riesgo de sangrado

Rivaroxaban Once-daily oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke
and Embolism Trial in Atrial Fibrillation
Efficacy:- Rivaroxaban was non-inferior to warfarin for prevention of stroke and non
CNS embolism.- Rivaroxaban was superior to warfarin while patients were taking study drug.- By intention-to-treat, rivaroxaban was non-inferior to warfarin but did not
achieve superiority.Safety:- Similar rates of bleeding and adverse events.- Less ICH and fatal bleeding with rivaroxaban.
Conclusion:- Rivaroxaban is a proven alternative to warfarin for moderate or high risk
patients with AF.


Ahrens I, et al. Thromb & Haemost 2011;115.

We suggest, that when OAC therapy is indicated, most patients should receive dabigatran in preference to warfarin. In general, the dose of dabigatran 150 mg po bid is preferable to a dose of 110 mg po bid (exceptions discussed in text). (Conditional recommendation. High Quality Evidence).
CCS-2010 AF GuidelinesCCS-2010 AF GuidelinesRecomendaciones de las Guías CanadiensesRecomendaciones de las Guías Canadienses

Hay algún rol para la Warfarina en el tratamiento de la FA?Hay algún rol para la Warfarina en el tratamiento de la FA?

31
ConclusionesConclusiones
1.1. Hay que conocer las guías: pero las guías NO reemplazanHay que conocer las guías: pero las guías NO reemplazanel juicio clínicoel juicio clínico
2. Hay que evaluar el riesgo de embolia en pacientes con FA:2. Hay que evaluar el riesgo de embolia en pacientes con FA:pero también hay que evaluar el riesgo de sangradopero también hay que evaluar el riesgo de sangrado
3.3. Hay que conocer la evidencia que guía nuestras accionesHay que conocer la evidencia que guía nuestras acciones4.4. Hay que elegir lo mejor para cada paciente en particularHay que elegir lo mejor para cada paciente en particular5.5. Hay que mantener la balanza en su punto justoHay que mantener la balanza en su punto justo
EMBOLIA SANGRADO